
Abstract
Background and Purpose:
Miniatured percutaneous nephrolithotomy (PCNL) techniques such as micro-PCNL (microperc) and ultramini-PCNL (UMP) are usually indicated for renal stones <2 cm. We present our preliminary report of treating patients with 2 to 3 cm renal stones using UMP in a semisupine combined lithotomy position associated with a retrograde ureteral access sheath (UAS).
Methods:
From April 2013 to January 2014, we implemented 13F UMP for 22 patients with renal stones that were 2 to 3 cm with the patient positioned in a 45-degree semisupine combined lithotomy position. A retrograde 9.5/11.5F UAS was placed for maintaining low intrarenal pressure and debris drainage. Flexible ureteroscopy was used for stones inaccessible through the primary percutaneous tract in two patients. A 200-μ holmium laser was used for stone disintegration. Intrapelvic pressure was measured using an open end 5F ureteral catheter inserted through the UAS.
Results:
All 22 cases were completed successfully. The mean preoperative stone size was 26.6 ± 4.7 mm (range 21–32 mm), mean operative time was 85.7 ± 18.0 minutes (range 47–112 min), and mean hemoglobin drop was 1.2 ± 0.3 g/dL (range 0.5–2.2 g/dL). Intrapelvic pressure during the surgical procedure ranged 5 to 10 cm H2O. The mean hospital stay was 3.1 ± 1.8 days (range 2–5 d). Complete stone clearance was 18/22 (81.8%) with solo UMP and 20/22 (90.9%) when associated with retrograde intrarenal surgery (RIRS). No major intra- or postoperative complications occurred.
Conclusion:
Implementation of UMP for the treatment of patients with renal stones 2–3 cm is feasible and safe. The procedure is less invasive and has a faster recovery period. Intraoperative retrograde UAS decreases intrarenal pressure, facilitates removal of stone fragments, and also allows simultaneous RIRS for stones in an inaccessible calix.
Introduction
I
On the other hand, retrograde intrarenal surgery (RIRS) has been found to be an effective and safe treatment option for even larger renal stones >2 cm; however, the greater re-treatment rate to reach a satisfactory SFR, steep learning curve, and high cost has been its major concern. 6,7 This makes PCNL a treatment choice for even smaller calculi in many centers. 8
Trauma to renal parenchyma and bleeding are associated with the tract size. 9 To minimize tract-associated complications, various researchers have introduced smaller-size tract PCNL such as mini-PCNL (miniperc), 10 micro-PCNL (microperc), 11 and ultramini PCNL (UMP). 12 Because of the decreased size of the scopes and sheath, however, the operative time as well as the potential chances of elevated intrapelvic pressure during the procedure are increased. 11,13,14 This limits the procedure for small-size stones and increases the possibility of systemic absorption of irrigation fluid containing bacteria or endotoxins, contributing to postoperative fever or even sepsis.
In this research work, we evaluate the outcome of UMP through a 13F percutaneous tract with the patient in a semisupine combined lithotomy position to manage 2 to 3 cm renal stones and simultaneously use a retrograde ureteral access sheath (UAS) to improve irrigation and maintain low intrapelvic pressure during the procedure.
Methods
Design and settings
From April 2013 to January 2014, we performed the procedure on 22 patients with renal stones that were 2 to 3 cm. All procedures were performed at our center by a single experienced surgeon (KX). Informed consent forms were signed by all enrolled patients.
Preoperative evaluation of patients included routine blood and urine tests, coagulation profile, urine culture, and imaging series including radiography of the kidneys, ureters, and bladder (KUB), intravenous urography, ultrasonography (US), and/or CT scan. Patients with positive urine culture were treated with appropriate antibiotics before PCNL. Stone size was calculated by measuring the longest diameter on preoperative imaging.
The procedures were performed with the UMP set (Schölly Fiberoptics GmbH, Denzlingen, Germany), which includes (1) an ultrathin telescope, 1 mm in diameter with a 0-degree view and a resolution of 17,000 pixels, (2) a 6F inner sheath, and (3) an outer 13F sheath (Fig. 1). The outer sheath has a tube of 3F welded to its inner wall and finally connected to a port outside. This port is used to inject saline during removal of stone fragments. The scope is fitted into the inner sheath, and the sheath has separate ports for irrigation and laser fiber (Fig. 2b).
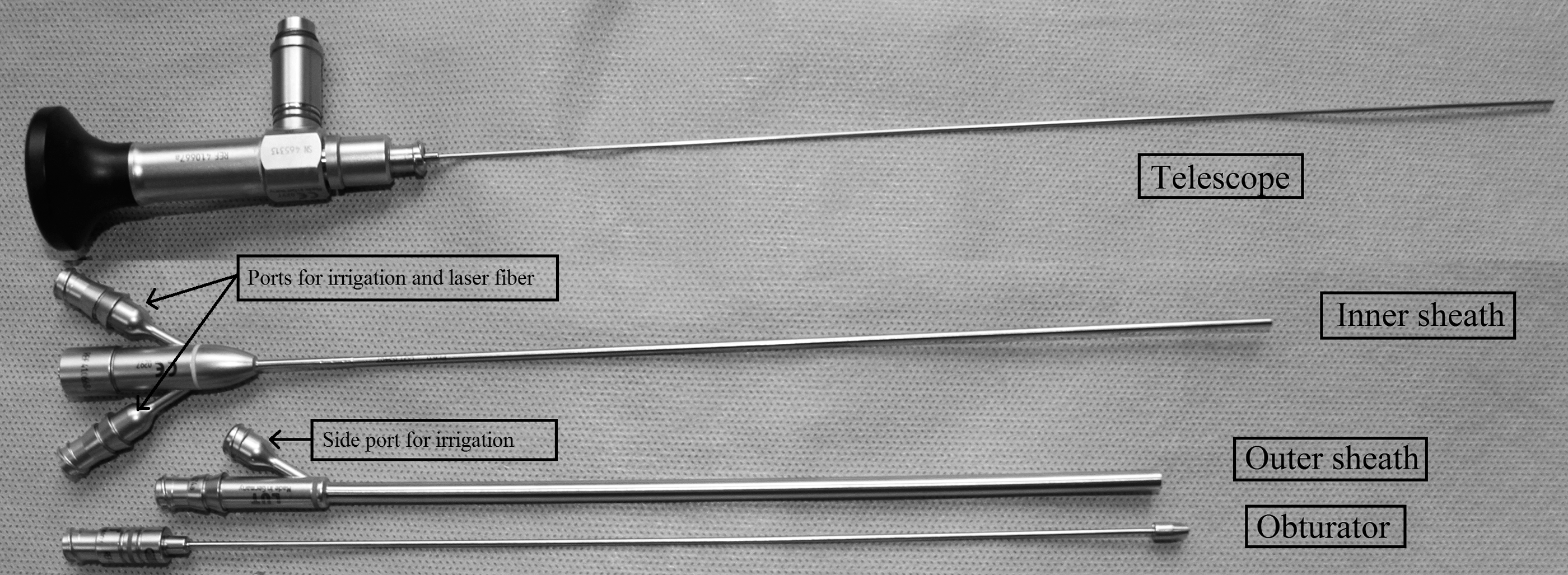
The UMP set: Telescope, inner sheath, outer sheath, and obturator. UMP = ultramini percutaneous nephrolithotomy.

Operative technique
With epidural anesthesia, patients were placed in a semisupine combined lithotomy position with the operating side elevated at 45 degrees. The ipsilateral leg was fully extended while the other was flexed, thus allowing a simultaneous retrograde approach throughout the procedure (Fig. 1a). A 8/9.8F Wolf semirigid ureteroscope (Richard Wolf, Germany) was used to confirm the ureter was free of stones or strictures, a 0.032-inch (0.81-mm) nitinol guidewire (OptiMed Medizinische Insturmente GmbH, Germany) was placed into the renal pelvis and, along the guidewire, a 9.5/11.5F (Flexor, Cook, Bloomington, IN) UAS was positioned possibly close to the renal pelvis.
Then, irrigation with 50 mL saline was through the UAS obturator to dilate the renal collecting system, facilitating puncture in the nonhydronephrotic kidney. Initial puncture into the dominant calix was made with an 18-gauge coaxial needle under US-guidance through a needle guide system attached to 3.5-MHz probe (Aloka Ultrasound System, Japan).
A successful puncture was confirmed by the efflux of irrigation fluid through the puncture needle; a guidewire was then introduced through the needle sheath into pelvicaliceal system. 10F and 14F fascial dilators were then sequentially used to dilate muscle and fascial layers. The UMP outer sheath was placed into the target calix along the guidewire. Nephroscopy was performed with the UMP nephroscope, and a peristaltic pump was used to irrigate saline. A 200-μ holium laser fiber (Lumenis GmbH, Germany) with energy output of 0.8 to 1.5 J at 10 to 15 Hz was then used to disintegrate stones into fragments of 2 to 3 mm.
The fragments were actively flushed out of the collecting system by creating an eddy flow of the irrigation fluid around the fragments either by irrigating through the scope and removing the scope rapidly out of the sheath or by manually injecting saline through the side port of the outer sheath after removing the nephroscope. The retrograde ureteral sheath served as an outflow tract for irrigation fluid as well as removal of stone fragments.
After endoscopic and US confirmation of no detectable stone fragments, a Double-J stent was placed anterogradely or retrogradely, and an 8F nephrostomy tube was placed into the collecting system and fixed. A 5F open-ended ureteral catheter was inserted intraoperatively into the renal collecting system retrogradely via the UAS and connected to the IBP channel of the anesthesia patient monitor with a baroreceptor to monitor the real-time renal pelvic pressure (Fig. 1c).
The nephrostomy tube was removed within 24 hours, and the urinary catheter was removed 48 hours postoperatively. Blood loss was calculated as the change in hemoglobin concentration between values in the preoperative and 24-hour postoperative complete blood cell count. KUB radiography was performed after 24 to 48 hours to access initial stone clearance. A residual stone of ≤4 mm was considered “stone free.” The Double-J stent in stone-free patients was removed at 2 to 4 weeks. In patients with residual fragments, the auxiliary procedures were planned at 4-week follow-up depending on the size and location of residual fragments detected in repeated KUB radiography.
Results
All 22 cases were successfully completed through a single 13F access tract with the patient positioned in a 45-degree semisupine combined lithotomy position. The patient demographics and perioperative data are listed in Table 1. The retrograde 9.5/11.5F UAS could be positioned without difficulty, and no patients needed balloon or coaxial dilation of the distal ureter. All punctures were US-guided, and the mean tract creation time was less than 3 minutes. RIRS was simultaneously used for removal of stones (>4 mm) inaccessible through the primary nephroscopy tract in two patients. The operative time was longer (maximum 112 min) in patients with hard stones and multiple caliceal stones necessitating simultaneous RIRS.
Tract creation time was the time puncture to successful placement of UMP sheath.
Operative time was the time from cystoscopy to placement of the nephrostomy tube.
SD = standard deviation; BMI = body mass index; SWL = shockwave lithotripsy; PCNL = percutaneous nephrolithotomy; UMP = ultramini percutaneous nephrolithotomy; RIRS = retrograde intrarenal surgery; ESWL = extracorporeal shockwave lithotripsy.
The mean hemoglobin drop was 1.2 ± 0.3 (range 0.5–2.2) g/dL, and no patient needed blood transfusion or embolization treatment. In this series, 18/22 (81.8%) of patients who underwent solo UMP and 20/22 (90.9%) who underwent UMP associated with simultaneous RIRS had no residual calculi. In two (9.1%) patients with residual fragments, one underwent a second UMP procedure 2 weeks after the initial UMP session and the other one needed SWL.
Fever (T >38.5°C) occurred once on the first postoperative day in one (4.5%) patient treated with combined RIRS and had a slightly longer operative time (110 min); it responded well with antibiotic treatment. Clinically insignificant hematuria lasting for more than 48 hours postoperatively was seen in two (9.0%) patients; it was managed conservatively. No other complications such as urosepsis, pneumothorax, injury to adjacent organs, or urine extravasation occurred.
Chemical analysis revealed pure calcium oxalate in three patients, pure calcium phosphate in two, a mixture of calcium oxalate and calcium phosphate in five, pure uric acid in one, and struvite in one. The remaining 10 patients had various other mixtures of stone types.
Discussion
Tract size is associated with renal parenchyma injury and, hence, blood loss, which is one of the most worrisome complications of PCNL. 9 Recent technical development has allowed smaller tract PCNL for nonbulky stones. Various researchers have reported the mini-PCNL technique through tract sizes ranging from 11F to 20F to be feasible and demonstrated reduced bleeding, hospital stay, and postoperative analgesics requirement when compared with standard PCNL. 8,10,15 –17 Giusti and colleagues, 13 however, found a 13F tract led to limited irrigation flow and necessitated more extensive stone fragmentation, leading to prolonged operative time.
Recently introduced single-step microperc through a 4.85F tract and holium laser lithotripsy has been appreciated by researchers for its high SFR of 82% to 93%, lower invasiveness, and faster recovery. The inability to completely remove the stone fragments, low visibility even with minimal hemorrhage, and limited maneuverability, however, seems to have limited it for small stones. Elevated intrarenal pelvic pressure because of the small sheath size and fluid intravasation has been its other concern. 11,18,19
UMP uses a special 6F mininephroscope to perform PCNL through an 11–13F metallic sheath. The early studies have shown minimal complication rate, a high SFR, and a very low auxiliary procedure rate; however, it is best for managing stones <20 mm, lower calix stones, and stones in children. 12,20 In our study, we have used UMP for stones of 20 to 30 mm, which led to a longer mean operative time. It is logical that the longer operative time and larger stone burden might increase the risk of bleeding. In our study, however, the mean blood loss was minimal without necessity of blood transfusion or embolization.
To diminish parenchymal bleeding, it is important to establish the percutaneous tract through the fornix of the posterior calix traversing minimal caliceal tissue to avoid injury to any interlobar arteries and large intrarenal vessels; avoid overdilation of the tract causing perforation of the renal pelvis with risk of laceration of the hilar vessels; adopt smaller tract size; minimize angulation of the dilation system, working sheath, and nephroscope shaft; avoid extensive torquing and use of flexible nephroscopes for calculi in inaccessible calices. 9
The intrapelvic pressure during PCNL can be elevated because of insufficient drainage of intrapelvic fluid through decreased interspace between the scope and the sheath. It can occur under conditions such as acute deflection of the scope to reach a stone in a remote target calix, the tip of scope positioned in a calix with a narrow neck or a caliceal diverticulum, the tip of the sheath located in the renal parenchyma causing collapse of parenchyma and urothelium around the endoscope, extraction of stone fragments with the forceps, or a stone in the sheath. Thus, renal pelvic pressure is likely to increase rapidly within a short time, which easily affects the renal structure and function.
Systemic fluid absorption may occur during PCNL through pyelovenous-lymphatic backflow, pyelotubular backflow, and forniceal rupture leading to fluid overload and may be clinically significant in patients with compromised cardiopulmonary or renal status, and in pediatric patients. Absorption of infected stone debris and bacteria released from the nidus of an infected stone on disintegration may lead to bacteremia, postoperative fever, and occasionally urosepsis.
Studies have shown that pyelovenous backflow can occur at pressures as low as 10 to 20 mm Hg. 21,22 Wang and associates, 23 in an animal study, found that as the perfusion pressure exceeded 20 mm Hg, the purulent infected kidney exhibited degenerative necrosis of the renal tubule, and the changes were more evident when the perfusion pressure was further increased to 40 mm Hg. In clinical practice, maintaining an intrapelvic pressure of less than 30 mm Hg is recommended during percutaneous intrarenal procedures. 21,22,24
Zhong and colleagues, 14 who measured renal pelvic pressure during minimally invasive PCNL through a 14 to 18F percutaneous tract, found that a 14F tract brought higher renal pelvic pressure than other larger tract groups and also higher accumulated time of renal pelvic pressure >30 mm Hg to cause fever from backflow. In research by Dogan and coworkers, 24 they found that 21% (17/81) of the patients had postoperative fever and suggested the absorption of perfusion fluid to be a high risk factor.
Urologists must be conscious of the potential fluid extravasation and absorption and attempt to prevent elevated intrarenal pressures during PCNL, especially when the collecting system contains infected urine or an infected calculus and in small tract PCNL in which the operative time tends to be longer and the interspace for fluid drainage is limited. Researchers have mentioned the significance of UAS in improving drainage and decreasing intrarenal pressure during ex vivo percutaneous nephroscopy, 25 and as well facilitating removal of stone fragments during SWL. 26
During our study, we found that the use of UAS efficiently facilitated irrigant drainage and maintained low intrarenal pressure (5–10 mm Hg) throughout the procedure even with high-pressure irrigation using a peristaltic pump. The improved irrigation flow rendered good visualization and facilitated rapid removal of stone fragments through the access sheath. UAS also allowed flexible ureteroscopy in two patients for managing stones in calices beyond the reach of the percutaneous access tract. This increased the stone clearance and lowered the chances of hemorrhage because of excessive torquing of the tract. In addition, an access sheath allowed passive elimination of small stone fragments throughout the procedure (Fig. 1d).
The routine use of UAS during flexible ureteroscopy has been found safe and beneficial for better visibility, lowering of intrapelvic pressure, and improving stone clearance. Lallas and associates, 27 evaluating ureteral blood flow, found a minimal decrease of 25% below baseline with a 10/12F UAS compared with other larger sizes and suggested that UAS can induce transient ureteral ischemia and promote an acute inflammatory response; however, it seldom causes ischemic necrosis. Delvecchio and colleagues 28 in their retrospective study did not find any evidence of ureteral stricture attributable to use of the UAS.
All the procedures in our study were completed with the patient in the 45-degree semisupine combined lithotomy position, which is similar to the Galdakao-modified supine Valdivia position. 29 Compared with the conventional prone position, this position eliminates the need for intraoperative change in patient position, provides a more comfortable position for the patient, and allows better patient monitoring for the anesthesiologist; simultaneous retrograde access was possible when needed. 29 Because the access tract is horizontal, it contributes to maintaining low intrapelvic pressure, and the stone fragments can be easily flushed out. The other advantage of this position is the comfortable sitting position for the surgeon during stone management. 30 The US guidance avoids the radiation hazard for both patient and operative team and prevents injury to the visceral organs. 9
The limitation of the study includes the nonrandomized controlled nature of the study. It was a prospective experimental case control designed study. Further studies of a randomized controlled nature on a larger number of patients, with stone size less than 2 cm and 2–3 cm, may provide us a valid conclusion with meaningful statistical power.
Conclusion
Implementation of ultramini PCNL for the management of renal stones 2 to 3 cm is feasible and safe. The procedure is less invasive and has a faster recovery period. An intraoperative retrograde ureteral sheath allows the possibility of simultaneous RIRS, decreases intrapelvic pressure, and facilitates removal of stone fragments.
Footnotes
Author Disclosure Statement
No competing financial interests exist.