
Abstract
Ultrasound-guided renal access for percutaneous nephrolithotomy (PCNL) is a safe, effective, and low-cost procedure commonly performed worldwide, but a technique underutilized by urologists in the United States. The purpose of this article is to familiarize the practicing urologist with methods for ultrasound guidance for percutaneous renal access. We discuss two alternative techniques for gaining renal access for PCNL under ultrasound guidance. We also describe a novel technique of using the puncture needle to reposition residual stone fragments to avoid additional tract dilation. With appropriate training, ultrasound-guided renal access for PCNL can lead to reduced radiation exposure, accurate renal access, and excellent stone-free success rates and clinical outcomes.
Introduction
U
While ultrasound-guided PCNL has been described in Asia and Europe, utilization in the United States has been limited. We present two approaches—transverse and longitudinal—for ultrasound-guided needle access into the collecting system for PCNL. We also present the novel use of ultrasound-guided needle puncture to reposition residual stone fragments into areas accessible through the initial renal access tract, sparing the patient from additional tract dilation and increasing procedural stone clearance rates through a single tract. With appropriate training and experience, urologists in a diversity of practice settings in the United States can implement these techniques.
Technique
Setup and ultrasound imaging
1. Before the procedure, collect preoperative urine for culture and sensitivities. Prior stone culture results may be helpful, if available, in the case of recurrent stone formers. Computed tomography imaging is often used to delineate renal and perirenal anatomy, as well as stone characteristics (Fig. 1). Administer preoperative antibiotics according to the institutional antibiotic guidelines.
2. Determine the method of anesthesia based on patient comorbidities. We find that general anesthesia with endotracheal intubation reduces movement and maximizes accuracy for instrument placement.
3. Position the patient in the supine or lithotomy position to facilitate placement of an externalized ureteral stent. This can be used intraoperatively for retrograde saline injection if caliceal dilation is needed.
4. After intubation, reposition the patient into the prone position.
5. Use a curved array ultrasound transducer in the 3.5 MHz range to visualize the renal parenchyma, collecting system, stones, and surrounding organs. As a general guideline, the depth of the ultrasound should be set to the 8–12 cm range. Selection of the actual depth should depend on maximizing the size of the kidney on the imaging screen. Gain should be set to the midrange so as to increase the contrast of the stone and needle against the collecting system and renal parenchyma to clearly visualize these points of interest. Areas of hyperechoic signal accompanied with postacoustic shadowing localize renal stones.
a. Doppler flow can facilitate visualization of vascular structures both within and surrounding the kidney. 8 If the calices are difficult to visualize, gentle, active, or passive retrograde injection of saline through the externalized ureteral catheter can be done. While diuretic administration has been shown to transiently dilate the calices and improve access, 1 we do not routinely administer diuretics for these cases.
6. Using ultrasonography, determine the target calix. The posterior calix is chosen in most instances, except when the stone is present in the otherwise inaccessible anterior calix.
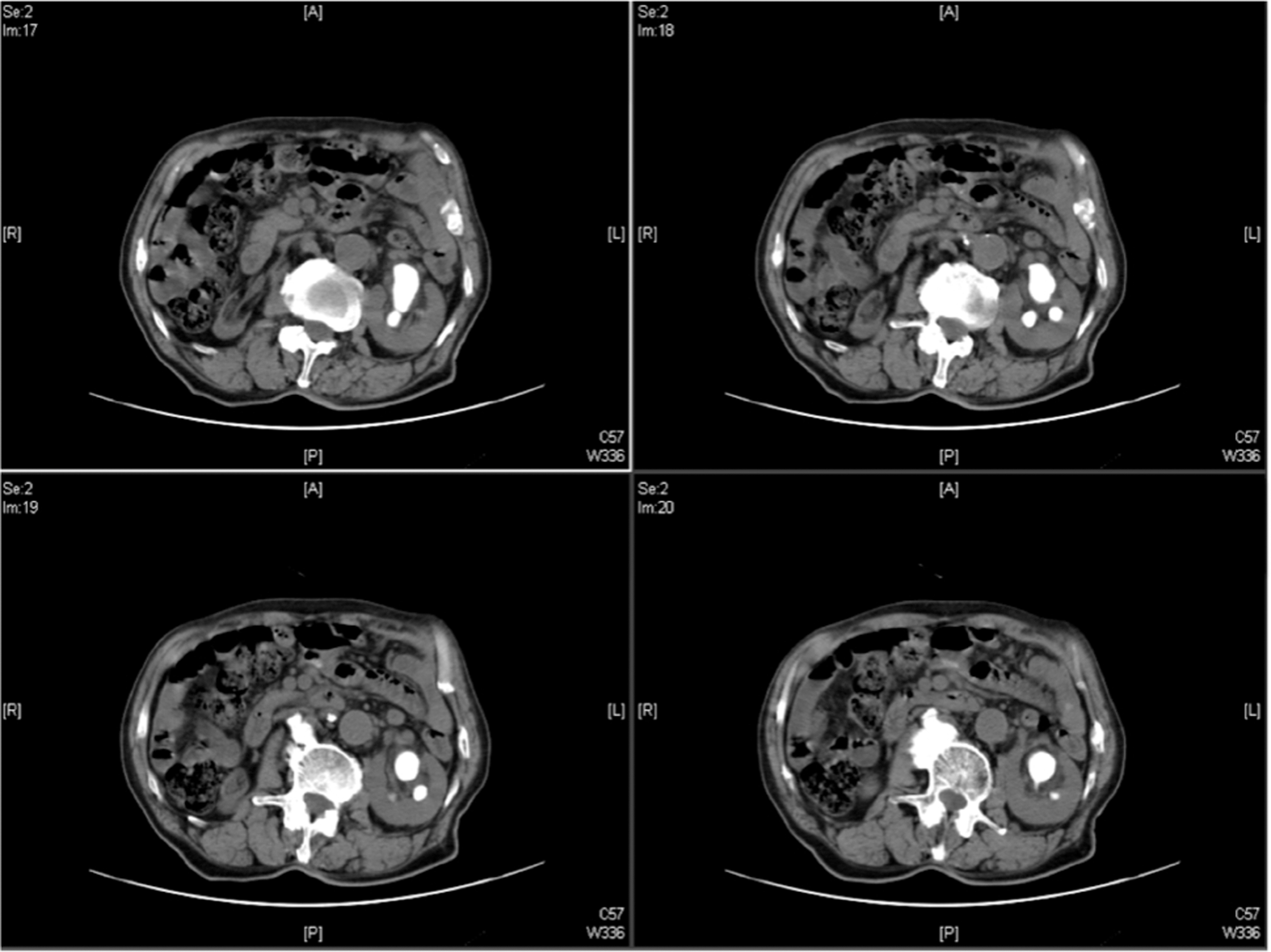
Computed tomography (CT) scan demonstrating a large left kidney staghorn calculus.
Ultrasound-guided puncture in the longitudinal or transverse imaging planes (Step 7 or 8)
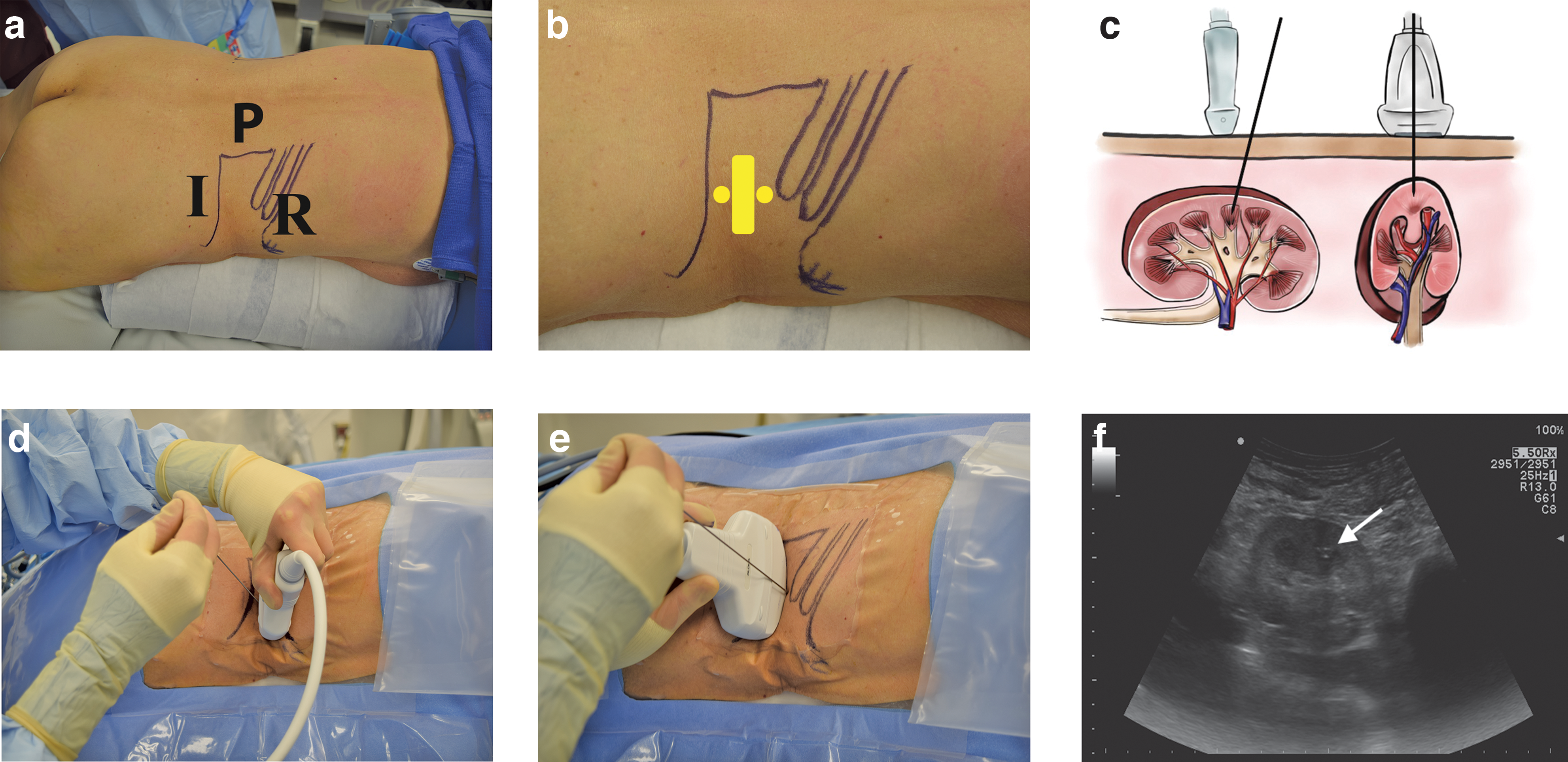
7. Longitudinal needle insertion (Fig. 2)
a. Using an 18- to 24-gauge needle with an echogenic tip, puncture the skin either in front of or behind the probe such that it travels parallel to the long axis of the probe (Fig. 2A).
b. Keeping the entire needle fully visualized from skin to kidney (Fig. 2F, white arrow), direct the tip of the needle into the end of the chosen calix (Fig. 2B, yellow dots; Fig. 2C). Close coordination between the hand holding the ultrasound probe (to maintain good visualization of the caliceal target) and the hand holding the needle (to bring the needle into the imaging plane) is required Fig. 2D,E. Ultrasonographic imaging can be used to avoid puncturing the surrounding viscera, such as the colon, spleen, and liver. Doppler signal can be used to identify blood vessels to avoid them within the kidney as well.
c. Avoid skin entry with the needle at too oblique an angle, which can make subsequent dilation and access more challenging. This is particularly relevant in lower pole access, in which oblique needle insertion from the caudal position behind the probe can result in the nephroscope abutting the patient's iliac crest (Fig. 2D).
8. Transverse needle insertion (Fig. 3)
a. Using the access needle, puncture the skin orthogonal to the long axis of the probe (Fig. 3B).
b. Continuously sweep the probe back and forth to visualize the needle path and guide the needle tip to the target calix (Fig. 3C). Similar to the longitudinal needle insertion technique, ultrasonographic imaging can be used to avoid puncturing the surrounding viscera and blood vessels.
c. Avoid the surrounding viscera, such as the colon, spleen, and liver. Doppler signal can be used.
d. The needle can be inserted into the skin at any distance from the side of the ultrasound probe (Fig. 3C,D), allowing a greater range in the angle of entry and avoiding rib shadowing.

The longitudinal approach to renal access.
The transverse approach to renal access.
Tract dilation
9. Tract dilation can be performed under ultrasonographic or fluoroscopic guidance, depending on the surgeon's comfort level with each imaging modality.
10. Once caliceal entry with the access needle is confirmed, remove the needle stylet and advance a guidewire into the collecting system through the needle and create a 1-cm skin incision surrounding the wire. We routinely use a J-tipped coaxial guidewire for maintenance of access and for dilation, although selection of the wire type will vary depending on the surgeon's preference.
11. Dilate the tract with a 10F fascial dilator, followed by a safety wire introducer. Through the safety wire introducer, insert a second coaxial guidewire into the collecting system and remove the introducer. Secure the safety wire to the drapes. Use either a serial dilator system or a balloon dilator for further fascial dilation, and position the access sheath for entry into the collecting system over the guidewire.
12. An offset rigid nephroscope and lithotripter device can be used for stone fragmentation and removal.
13. After stone removal, a nephrostomy tube and/or ureteral stent can be placed for renal drainage as clinically indicated.
Ultrasound-guided needle repositioning of residual stone
1. Intraoperative imaging may reveal the residual stone in an inaccessible location from the initial access tract, often due to the sharp angle of the infundibulum used for access relative to the residual stone location.
2. Under ultrasound guidance, insert a 24-gauge percutaneous renal access needle into the calix containing the residual stone.
3. Use the needle tip to dislodge the stone from the lower calix and push it into the renal pelvis, where it can be accessed, fragmented, and removed through the original access tract (Supplementary Video S1; Supplementary Data are available online at
Equipment
1. Ultrasound with transducer in the 3.5 MHz range
2. Eighteen- to 24-gauge needle with an echogenic tip
3. J-tipped coaxial guidewires
4. Fascial dilators
5. Safety wire introducer
6. Access tract serial or balloon dilator set with sheath
7. C-arm with omnipaque if needed for tract dilation
8. Rigid nephroscope and lithotripter device for lithotripsy
9. Nephrostomy tube or stent as clinically indicated
Role in Urologic Practice
Indications and contraindications for ultrasound-guided renal access are similar to fluoroscopic renal access. Ultrasound-guided renal access can be used for a range of stone configurations, including single pelvic or caliceal stones, renal units containing multiple stones, or staghorn calculi. Ultrasound guidance is preferred in special populations such as children and pregnant women to minimize radiation exposure. While the presence of hydronephrosis may facilitate ultrasonographic renal imaging, it is not required for efficient needle puncture.
Difficulty with needle visualization by ultrasound carries a risk of inaccurate needle placement and perforation of the surrounding viscera and vasculature. Published literature shows that the most common complications of ultrasound-guided PCNL by urologists are urinary-tract infection (1.1%), hemorrhage (1.9%), sepsis (0.76%), inferior vena cava injury (0.15%), gallbladder injury (0.15%), and death (0.3%). 8 Major complications occurred in 3.3% of patients and minor complications in 5%. 8 Multiple studies have demonstrated no difference in hospital stay, stone-free rates, or postoperative complication rates between patients who undergo ultrasound- versus fluoroscopy-guided renal tract access for PCNL. 4,9 One case-matched study comparing outcomes of ultrasound- and fluoroscopy-guided PCNL in 5806 patients found that postoperative hemorrhage and blood transfusion rates were significantly higher in the fluoroscopy group (11.1% vs 3.8%, p = 0.001), although they noted the use of larger access sheaths in the fluoroscopy group (22.6F vs 29.5F, p < −0.001) and longer hospital stays in the ultrasound group (5.3 vs 3.5 days, p < 0.001). 10
Utilizing ultrasound to achieve percutaneous renal access for PCNL has been established as safe and effective, with excellent clinical outcomes. Used in combination, ultrasound and fluoroscopy during PCNL can achieve comparable clinical outcomes and stone-free rates relative to fluoroscopy alone. 11,12 A randomized prospective trial comparing outcomes of ultrasound-guided PCNL access to traditional fluoroscopic access in 224 patients demonstrated increased accuracy of puncture, fewer number of puncture attempts, shorter operative time, and reduced radiation exposure time, with similar rates of procedural success and length of hospital stay for the ultrasound group. 7 In another study, urology residents undergoing PCNL training were able to achieve decreased radiation exposure time and higher accuracy of puncture for pure ultrasound-guided PCNL, although 6 of 32 patients required fluoroscopic adjustment. 12 In a single-center study of 700 patients who underwent complete ultrasound-guided PCNL in China, 92.6% of patients with a single calculus and 82.9% of patients with staghorn or multiple stones were rendered stone free. 13 In comparison, fluoroscopy-guided PCNL resulted in a 98.5% clearance rate for a solitary stone and 71% for complex staghorn stones in another study. 14
In this study, we describe two methods for ultrasound-guided renal access during PCNL, which can be implemented in most operating rooms in the United States. While a learning curve exists to master these techniques, their adoption may lead to reduced radiation exposure for patients, urologists, and ancillary health providers when performing PCNL. Using an access needle to reposition residual stone(s) into an accessible calix is a novel application of ultrasound during PCNL. This technique presumes that the stone being repositioned is small enough to pass through the infundibulum to an accessible area of the kidney, such as the renal pelvis. Flexible nephroscopy and laser lithotripsy through the initial tract remain our first-line approach to reaching residual stone fragments. However, needle repositioning may be helpful when the angle of the calix harboring the residual stone is too sharp from the access tract of entry for a flexible nephroscope to navigate. However, there are potential risks to applying this technique. New needle punctures carry a small risk of infection, bleeding, and tissue injury and should only be attempted in cases where a stone is amenable to safe displacement. However, a primary advantage of this technique is that it may help the surgeon avoid the morbidity associated with dilation of multiple renal access tracts. 11,15,16 Ultrasound-guided stone repositioning may be a pragmatic and safe strategy for patients undergoing PCNL and merits future study.
There are advantages and disadvantages to both the transverse and longitudinal approaches for ultrasound-guided percutaneous renal access. With the longitudinal needle technique, the trajectory of the needle can be fully visualized. However, the needle must be perfectly aligned with the plane of ultrasound imaging. This can be challenging particularly when the skin-to-stone distance is long. Failure to image the needle tip can result in inadvertent injury to the surrounding structures. In the longitudinal approach, the needle sometimes enters the skin at an oblique angle, which may make subsequent tract dilation and lithotripsy more challenging. In the transverse approach, the needle can enter the skin at a greater range of distances from the probe head and angles to the skin. Thus, rib shadowing is more easily avoided. However, then the needle is never fully visualized and the operator must adjust the imaging plane constantly to coordinate with needle advancement. These advantages and disadvantages should dictate the use of each technique specific for the patient's body habitus, renal anatomy, and stone location.
The importance of reducing radiation exposure should not be underestimated, both for the physician as well as the patient. Over the course of their careers, urologists may be exposed to radiation on a regular and cumulative basis, 17,18 and patients with recurrent stones may be subjected to repeated radiation exposure during evaluation and subsequent procedures. 19 –21 This is particularly relevant in younger patients as radiation exposure is correlated with increased risk for malignancy over time. 22 Replacing fluoroscopy with ultrasound for renal access, as well as for stone repositioning, may mitigate these healthcare risks.
Footnotes
Acknowledgments
The authors thank Catherine Tsai for providing the medical illustrations used in Figures 2 and ![]() . Funding source: K12-DK-07-006: Multidisciplinary K12 Urologic Research Career Development Program (TC).
. Funding source: K12-DK-07-006: Multidisciplinary K12 Urologic Research Career Development Program (TC).
Author Disclosure Statement
The authors declare no conflicts of interest.
Abbreviation Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.