
Abstract
Objective:
The goal of this randomized controlled trial was to compare the outcomes of robot-assisted laparoscopic donor nephrectomy (RDN) with standard laparoscopic donor nephrectomy (LDN).
Materials and Methods:
Forty-five voluntary kidney donors (27 for right subgroup and 18 for left subgroup) who met inclusion and exclusion criteria were randomized into 2 groups, RDN and LDN in 1:2 ratio. Primary endpoints were visual analogue scale (VAS) pain scores, analgesic requirement, and hospital stay of donors. Secondary endpoints were donor's intraoperative and postoperative parameters, graft outcomes, and donor surgeon's difficulty scores.
Results:
All procedures were completed without any intraoperative complications. VAS pain scores at 6, 24, and 48 hours (p = 0.00), analgesic requirement (p = 0.00), and hospital stay (p = 0.00) were less in RDN than in LDN. Longer graft arterial length could be preserved with robotic approach on right side (p = 0.03) but not on left side (p = 0.77). The RDN group required more number of ports (p = 0.00), longer retrieval time (p = 0.00), and warm ischemia time (WIT) (p = 0.01). Total operative time (p = 0.14), hemoglobin drop (p = 0.97), postoperative donor complications (p = 0.97), and the recipient estimated glomerular filtration rate at 9 months (p = 0.64) were similar in both groups. Difficulty scores of console surgeon were less in most steps on right side but not on left side. Patient-side surgeon in RDN had higher difficulty scores for retrieval.
Conclusion:
RDN is safe and is associated with better morbidity profile than LDN. Robotic approach provides technical ease and facilitates preservation of longer length of renal artery on right side. Left RDN is associated with longer WIT; however, this does not translate into poor graft outcome.
Introduction
D
Materials and Methods
The study was started after approval from an institutional review board. Study enrollment time was from March 2014 to February 2015. Inclusion criterion was live-related voluntary kidney donor approved by institutional medical, ethical, and legal boards for transplantation. Exclusion criteria were donor unwilling for inclusion in the study, body mass index (BMI) >35 kg/m2, multiple arteries and veins, and ipsilateral adrenal adenoma. Primary endpoints were the postoperative visual analogue scale (VAS) pain scores at 6, 24, and 48 hours, analgesic requirement in the first 48 hours, and hospital stay of the donors. Secondary endpoints were donor's intraoperative and postoperative parameters, such as hemoglobin drop, preserved graft arterial and venous length, TOT, retrieval time (RT), WIT, number of ports, donor creatinine at 1-month follow-up, and intraoperative and postoperative complications with the Clavien–Dindo complication scale. Recipient-related secondary endpoints were estimated glomerular filtration rate (eGFR; Cockcroft–Gault) at 7 days and 1, 3, 6, and 9 months, graft-related complications, and graft loss. Surgeon's difficulty scores for different steps of surgery were also analyzed. A total of 45 donors were to be enrolled into the study, with an enrollment ratio of 1:2 in robotic:laparoscopy arm, for establishing mean pain score difference of 1 with standard deviation of 1 to reject the null hypothesis that the means of robotic and laparoscopic pain scores are equal, with a probability (power) of 0.871 and the type 1 error (α) of 0.05. The sample size was calculated with power and sample size program version 3.0.7.
Forty-five live-related voluntary kidney donors who met inclusion and exclusion criteria were planned for right (n = 27) or left (n = 18) donor nephrectomy. They were randomized into the robotic (Da Vinci Si™; Intuitive Surgical®, Sunnyvale, CA) or laparoscopic approach for donor nephrectomy with the chit method (Fig. 1).
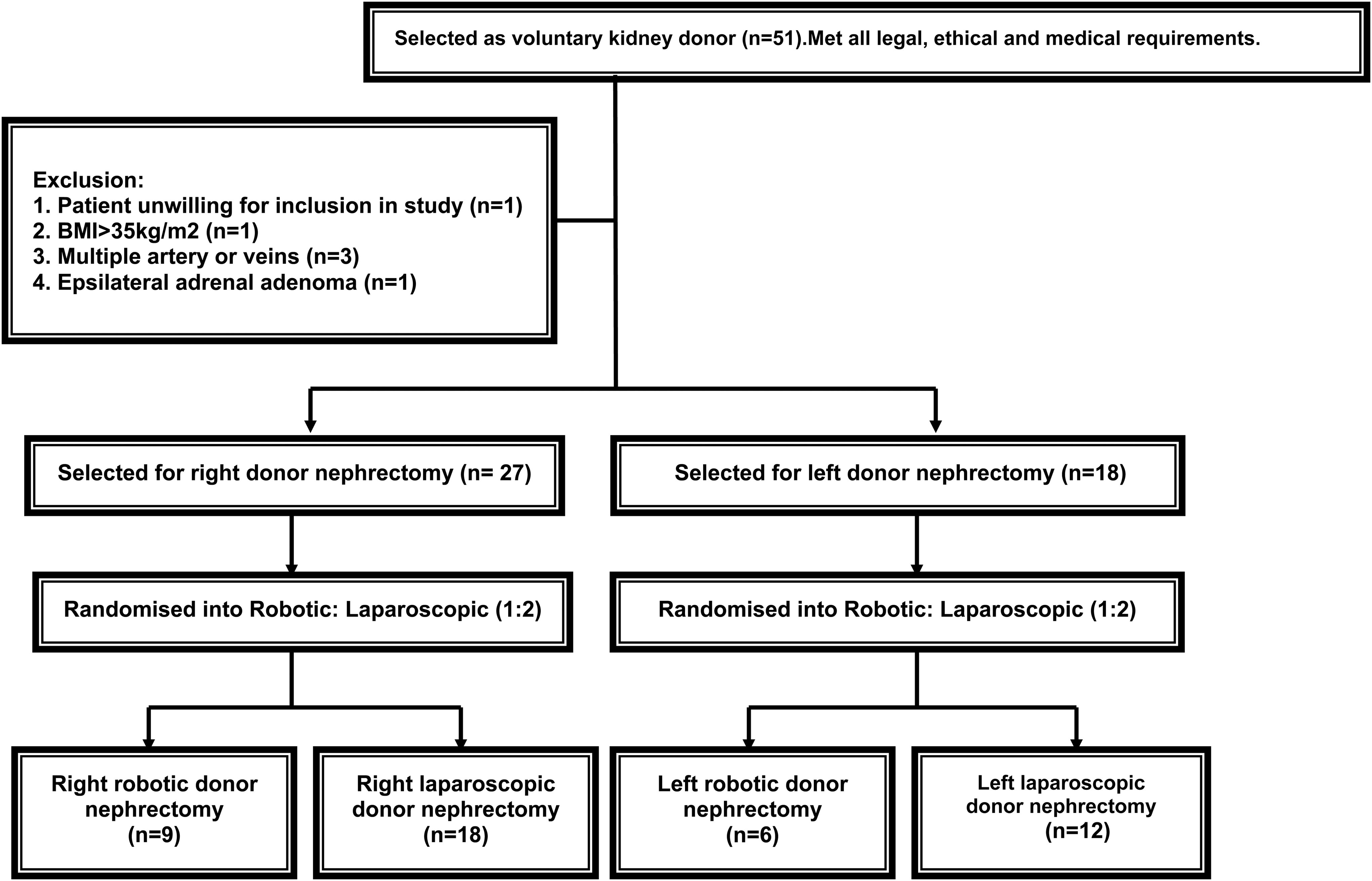
Flowchart showing the randomized enrollment of the voluntary kidney donors.
Parameters noted in all donors preoperatively were age, gender, comorbidities, previous surgeries, eGFR (Cockcroft–Gault), serum creatinine, BMI, and length of renal artery and vein (up to the level of bifurcation) on CT angiography.
RDN and LDN were performed by same two surgeons with expertise in robotic surgery as well as laparoscopic surgery. Patient-side surgeons in RDN were those with expertise in laparoscopic surgery. The operative room team in both groups was same.
In right LDN, access was achieved from three 12-mm ports for camera and working and two 5-mm ports for lifting the ureterogonadal packet and liver retraction. In 9 of 18 cases, an additional 12-mm port was placed from the Pfannenstiel retrieval wound for insertion of vascular stapler. In left LDN, two 12-mm ports for camera and working and two 5-mm ports for working and lifting the ureterogonadal packet were used. Three left LDN could be managed without port for lifting the ureterogonadal packet. In left RDN, three 8-mm robotic working ports and two 12-mm ports, one for the robotic camera and another bedside surgeon's working port, were used. In right RDN, in addition to the above-mentioned ports, one more 12-mm port in the Pfannenstiel retrieval wound for stapler insertion was used in 7 of 9 cases, and one 5-mm port for liver retraction was used in all cases.
The steps of the surgery were similar in LDN as well as RDN. The difficulty scores (VAS score 0–10; 0 being easiest and 10 being most difficult) of donor surgeon were noted for bowel reflection, lifting the ureterogonadal packet, hilar dissection, upper pole dissection, clipping and dividing the ureterogonadal packet, clipping renal artery and vein, transecting renal artery and vein, and retrieval of graft in the laparoscopy group. In RDN, the console surgeon's difficulty scores were noted for bowel reflection, lifting the ureterogonadal packet, hilar dissection, upper pole dissection, and transecting renal artery and vein, and bedside surgeon's difficulty scores were noted for clipping and transecting the ureterogonadal packet, clipping of renal artery and vein, and retrieval of graft.
A 5- to 7-cm Pfannenstiel incision was placed and deepened to the level of parietal peritoneum at the beginning of surgery for graft retrieval. Mannitol was given intravenously before transecting ureterogonadal packets. After transecting, the ureter brisk urine output was observed from the transected ureter before clipping of hilar vessels. After transecting renal vein, graft was freed of lateral attachments and kept free in the peritoneal cavity. After incising this parietal peritoneum in the Pfannenstiel incision, graft is retrieved in longitudinal axis by hand introduced into the peritoneum by donor surgeon in LDN and patient-side surgeon in RDN. During retrieval, undocking of the fourth arm of robot was necessary in most of the cases with RDN. Local anesthetic was not infiltrated in wound or instilled intraperitoneally. The length of artery and vein up to bifurcation was noted on bench. Arterial or venous length sacrificed during clipping = preoperative length on CT angiography – length on bench. RT was considered from clipping of artery up to the retrieval from donor. WIT was considered from clipping of artery up to reperfusion of the kidney with perfusion fluid till the time when efflux from renal vein is clear. Docking time was noted in robotic cases. Donors were discharged when they were allowed full oral diet, passed motions, and were ambulant and comfortable.
Statistical analysis was performed with Statistical Package for the Social Sciences version 15.0. The analysis was performed for comparing RDN with LDN. A subgroup analysis was performed to compare right RDN with right LDN and left RDN with left LDN. The chi-square test and Student's t-test were used for categorical and continuous variables, respectively.
Results
Both the RDN and LDN groups as well as right and left donor subgroups had similar demographic parameters (Table 1).
BMI = body mass index; LDN = laparoscopic donor nephrectomy; RDN = robot-assisted laparoscopic donor nephrectomy.
All 15 RDN were completed without conversion to LDN or open donor nephrectomy. All 30 LDN were completed without conversion to open donor nephrectomy. In all the RDN and LDN, the ureter was traced down and transected at the level of pelvic brim. There were no intraoperative complications in any RDN or LDN. All the recipients (n = 45) in both groups had good urine output on table after vascular anastomosis.
The analysis of intraoperative and postoperative donor parameters, recipient and graft outcomes, and subgroup analysis are shown in Table 2. Donor VAS pain score at 6, 24, and 48 hours, analgesic requirement, and hospital stay were less in the RDN group compared with the LDN group (Fig. 2). There was no significant difference in donor's TOT, hemoglobin drop, complications and serum creatinine at 1 month, recipient eGFR at 7 days and 1, 3, 6, and 9 months (Fig. 3), or graft complications between the RDN and LDN groups. More ports were necessary in RDN in either of the subgroups. The RT was higher in the RDN group. The WIT is higher in the RDN group overall as well as in the left subgroup. However, it is not significantly different in the right subgroup.
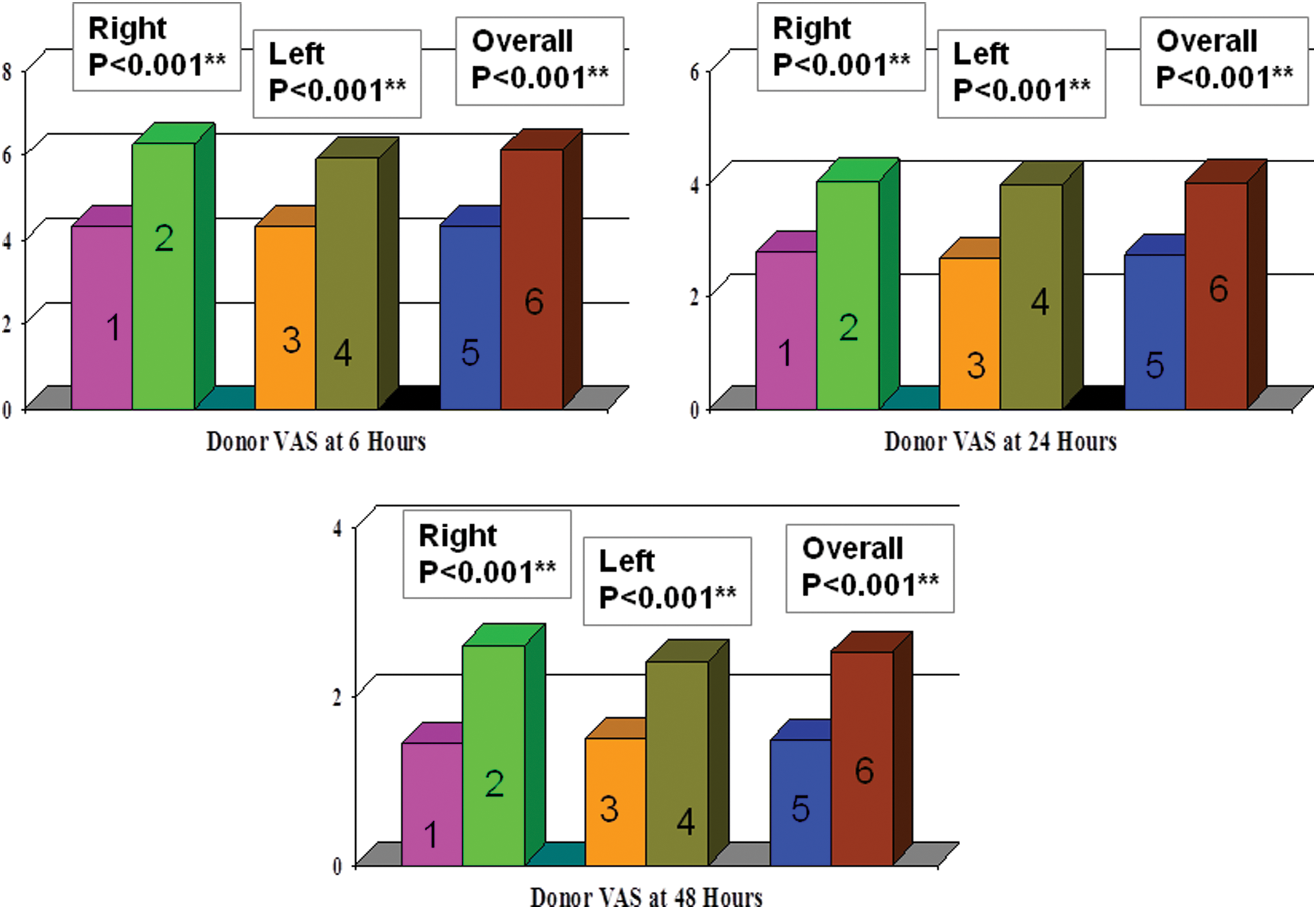
Comparison of donor visual analog scale pain scores in RDN and LDN groups at 6, 24, and 48 hours. Bars 1, 2, 3, 4, 5, and 6 represent right RDN, right LDN, left RDN, left LDN, all RDN, and all LDN, respectively. LDN, laparoscopic donor nephrectomy; RDN, robot-assisted laparoscopic donor nephrectomy. Color images available online at
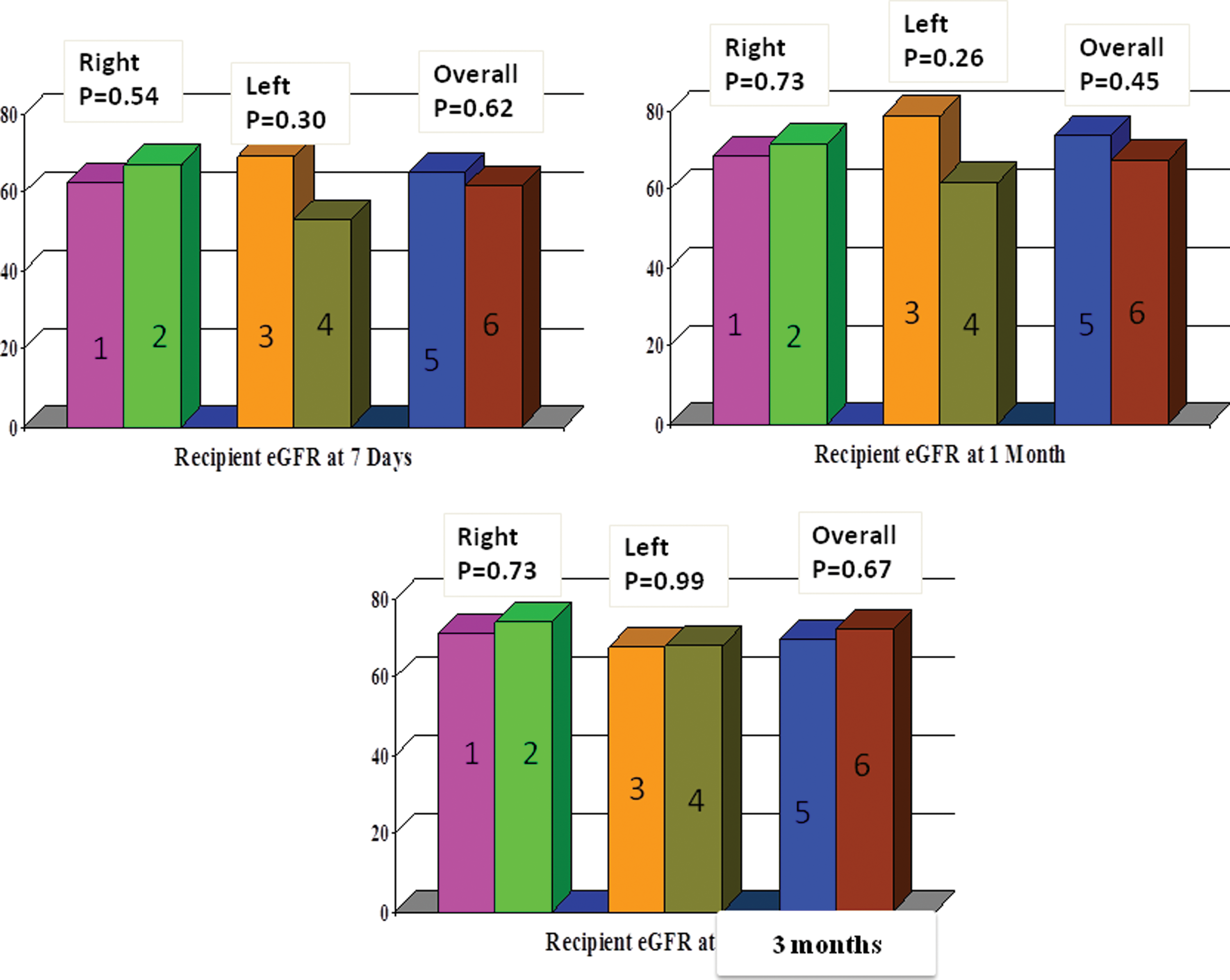
Comparison of recipient eGFR at 7 days and 1 and 3 months in RDN and LDN groups. Bars 1, 2, 3, 4, 5, and 6 represent right RDN, right LDN, left RDN, left LDN, all RDN, and all LDN, respectively. Color images available online at
eGFR = estimated glomerular filtration rate; N.A. = not applicable; VAS = visual analog scale.
In right RDN, longer artery length could be preserved compared with right LDN. This was not found in the left subgroup. There was no difference in sacrificed length of vein during clipping in RDN or LDN in both subgroups.
Two surgeons (one on console and one on patient side) were necessary in RDN compared with single donor surgeon in LDN. The difficulty scores of surgeons are compared in Table 3. The VAS score of patient-side surgeon in RDN was higher in graft retrieval compared with that of donor surgeon in LDN in both right and left subgroups. In the right subgroup, the VAS scores of RDN surgeons were less than those of LDN surgeon, except the step of upper pole dissection and adrenal sparing, which had similar VAS scores. In left subgroup, the VAS scores of RDN surgeon and LDN surgeon are similar, except the step of renal artery and vein transection, which was easier in the RDN group.
Discussion
Most important in introduction of any new technology is safety associated with the technique. This is more so in transplant because donor as well as graft safety are at stake. As found in our study, the RDN is a safe technique. It is associated with similar, immediate, and early postoperative outcomes in donors as well as corresponding recipient's graft function. Previous literature also suggests that RDN is safe. 5,8,9
A study comparing robotic surgery with laparoscopy suggested that the robotic approach is associated with less pain than the laparoscopic approach. 10 The possible reason for less pain in robotic surgery is robotic arms, which are pivoted around the port site moved at fixed remote center. So there is less leverage around the port site and lesser pressure at port sites, which lead to lesser trauma to abdominal wall tissues around the port. Our study suggested that RDN is associated with lesser pain score and lesser analgesic requirement compared with LDN. This also translates into earlier recovery and discharge from the hospital. Although the voluntary kidney donors donate with altruistic purpose, any donor will prefer an approach that further reduces the morbidity associated with donor surgery. It is for this reason that live donor nephrectomy rates increase after the advent of LDN compared with open donor nephrectomy. 11,12 RDN may further reduce morbidity associated with donor nephrectomy.
Most of the transplant centers prefer left-sided graft kidney over right in view of small right vein length and the need for retrocaval dissection or flipping of the kidney on right side to achieve good graft artery length. 13,14 In right donor nephrectomy cases with early branching artery, it is particularly important to do retrocaval dissection to get a good common stump. Retrocaval dissection is also necessary for getting inferior vena cava (IVC) cuff in cases with small renal vein and to free up the tissues behind renal vein so that stapler blade can slide behind renal vein. If right lumbar veins are entering IVC posteriorly near the opening of renal vein, then retrocaval dissection helps in taking care of lumbar veins. 13 This retrocaval dissection is technically a more difficult maneuver, which is never necessary on the left side. Studies also propose that the robotic approach with its three-dimensional vision, seven degrees of freedom, higher magnification, and enhanced dexterity compared with the standard laparoscopic approach facilitates the renal hilar dissection. 15 In our study, we found that the VAS score of donor surgeon for right hilar dissection was lesser in RDN than in LDN. The right kidney was flipped in two RDN. The preserved renal artery length was more in right RDN than in right LDN. The technical ease was felt in right RDN compared with right LDN in all steps other than upper pole dissection and retrieval. However, it is worth noting that this technical ease did not reach a level of significance in any steps of left RDN vs LDN except transecting of renal artery and vein. The sacrificed length of artery or vein length was not different in left RDN and LDN. This suggests that the robotic approach may provide some technical advantages compared with the laparoscopic approach on right side but not so significantly on left side. At the time of writing this article and during the conduct of this study, instruments, such as robotic vascular stapler and so forth, were not available. Availability of such instruments will further reduce the role of patient-side surgeon and may influence the technical ease of this surgery. It may also reduce the steep learning curve associated with LDN. 9
The TOT was not different in RDN and LDN. However, the WIT was significantly more in the left RDN group than in the LDN group (p = 0.01, power of test for this parameter = 87.8%), which is definitely a matter of concern. The RT was more in RDN in both subgroups. The difference in WIT did not reach a level of significance on right side. Possible cause for this increased WIT and RT in RDN is the necessity to undock the fourth arm during retrieval. This is also a cause for increased patient-side surgeon's VAS score for retrieval in RDN.
The increase in WIT does not translate into recipient graft function in a limited range of time. 16,17 The recipient graft-related complications or eGFR was not different between the RDN and LDN groups at 7-day and 1-, 3-, 6-, and 9-month follow-ups in our study as well.
We acknowledge the limitation of our study that although it is well powered for its primary endpoints, it is less powered for few of the secondary endpoints. The longest recipient graft follow-up is 1 year in our study, and we do not have any longer follow-ups. Donors were not blinded for the type of the treatment. However, it was not possible to blind donors about the type of treatment because of the nature of surgery. Donors were informed and explained, and they consented for the type and nature of surgery, either robotic assisted or standard LDN. Last but not least, our study does not focus on the economic aspects of comparison between RDN and LDN. The RDN increased the cost of surgery for donor nephrectomy. 18 It remains to be determined if the benefits of RDN in reducing donor morbidity and technical ease associated with it outweigh the cost implications associated with it.
Conclusion
RDN is a safe procedure and is associated with better postoperative pain scores, analgesic requirement, as well as lesser hospital stay compared with LDN. Robotic approach in right donor nephrectomy is associated with more technical ease to console surgeon compared with laparoscopic donor surgeon in most of the steps of surgery and facilitates preservation of longer length of right renal artery. However, there is no significant technical ease associated with left RDN compared with left LDN. Left RDN is associated with longer WIT than LDN; however, this does not translate into poor graft outcomes.
Footnotes
Acknowledgment
The authors thank Mr. Shashikant Chinchole for helping with the statistical analysis.
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.