
Abstract
Purpose:
Ureteroureterostomy (UU) is a useful surgical option for the management of duplication anomalies as well as obstructed single system ureters for children. We aimed to evaluate the safety, efficacy, and outcomes of robot-assisted laparoscopic UU (RALUU) compared with open UU (OUU) in the pediatric population.
Patients and Methods:
A retrospective review was performed at two institutions including six surgeons' experience with all cases of RALUU and OUU from January 2005 to June 2014. Indications for a surgical procedure included duplex systems with an upper pole ectopic ureter, obstructed ureterocele or lower pole vesicoureteral reflux, and obstruction in a single system. Transureteroureterostomy, laparoscopic UU, and major reconstruction cases where UU was the secondary procedure were excluded.
Results:
There were 25 RALUU and 19 OUU cases included. All cases involved duplex systems except two proximal to distal anastomoses in single system obstructed kidneys. RALUUs were more likely to be performed proximally (P = 0.01) and with the use of cystoscopy and stent placement (P = <0.0001). Operative times and estimated blood loss were similar between the two groups. Postoperative complications included four febrile urinary tract infections in each group, one recurrence of nonfebrile urinary tract infection in the open group, and one postoperative obstruction at the ureterovesical junction because of attempted stent placement necessitating nephrostomy tube placement in the open group. This OUU patient was the only one to demonstrate more severe hydronephrosis after surgery on initial follow-up imaging that was again unrelated to the open UU procedure. RALUU had shorter hospital stays by 0.5 days (P = 0.04).
Conclusion:
Robot-assisted laparoscopic UU is a safe and effective alternative to open UU in children with duplication anomalies and single system obstructed ureters. Operative times and complication rates were comparable with slightly shorter length of hospitalization in robotic cases.
Introduction
W
Robotic ureteroureterostomy (RALUU) has been commonly performed in children with duplicated collecting systems that may be associated with an ectopic ureter, ureterocele, or vesicoureteral reflux. 4 –6 No studies have been performed to date comparing robotic cases with open ureteroureterostomy (OUU). Therefore, we aimed to evaluate our bi-institutional experience of robotic versus open ureteroureterostomy (UU) in the pediatric population.
Patients and Methods
After Institutional Review Board approval, a retrospective review was performed at two institutions including six surgeons' experience with all cases of RALUU and OUU from January 2005 to June 2014. Cases were identified using Current Procedural Terminology codes of 50760 (ureteroureterostomy), 50770 (transureteroureterostomy) and 50949 (unlisted laparoscopy procedure, ureter); however, transureteroureterostomy, pure laparoscopic UU cases, and major reconstruction cases where UU was the secondary procedure were excluded. Indications for a surgical procedure included duplex systems with a superior moiety ectopic ureter, obstructed ureterocele or inferior moiety vesicoureteral reflux, and midureteral obstruction in a single system.
Patient demographics, surgical technique, outcomes, and complications were analyzed. For robotic UU cases, two configurations of port placement were used based on surgeon preference. For proximal ureteroureterostomy, an 8.5-mm camera trocar was placed at the umbilicus, and two 5-mm robotic arm trocars were placed midline or slightly laterally toward the site of surgery, approximately four fingerbreadths above and below the umbilicus. Alternatively, for a distal anastomosis, an 8.5-mm umbilical camera port was used with two 5-mm trocars on either side of the umbilicus at the level or just inferior of the umbilicus.
For open UU cases, typically a flank or Pfannenstiel incision was made. For RALUU, a cystoscopy with ureteral stent placement was routinely performed at the beginning of the case. Use of a stent extraction string was surgeon dependent. Stents were otherwise placed at the discretion of the surgeon for open cases. Foley catheters were routinely placed in all patients from both cohorts; however, Penrose drains were variably placed in open cases. Location of the anastomosis was also decided on an individual basis for both robotic and open cases.
Complications were graded based on the Clavien classification system. 7 For initial follow-up imaging, a renal ultrasonogram or furosemide diuretic renogram was obtained to assess the degree of hydroureteronephrosis or drainage at 4 to 14 weeks postoperatively. Categoric data were analyzed using the Fisher exact test or chi-square test. Normally distributed continuous data were analyzed using the Student t test (two-tailed). A P value of <0.05 was considered statistically significant.
Results
Twenty-five RALUU and 19 OUU cases were included (Table 1). There were14 patients excluded from analysis: 8 patients underwent a transureteroureterostomy, 1 patient underwent a laparoscopic UU, 2 patients underwent a UU as a secondary procedure, 2 patients were coded as having a UU but actually underwent pyeloplasties, and 1 patient had no medical records available. Mean age of patients was 6.1 years in the robotic cases and 3.9 years in the open cases (P = 0.18) with similar mean weights between the two groups (P = 0.27).
RALUU = robotic ureteroureterostomy; OUU = open ureteroureterostomy.
All cases involved duplex systems except two proximal to distal anastomoses in single system obstructed kidneys because of midureteral strictures. In the RALUU cases, three of the three (100%) patients with ureterocele underwent endoscopic puncture of the ureterocele before the ureteroureterostomy, while in the OUU cases, two of the four (50%) patients with ureterocele underwent prior endoscopic puncture.
RALUUs were more likely to be performed in a proximal location near the kidney (P = 0.01), while OUUs were more likely to be performed distally near the bladder (P = 0.04). Cystoscopy with stent placement was performed in all RALUU cases and in 8 of 19 (62%) open cases (P = <0.0001). Fourteen (74%) OUU patients, however, had a Penrose drain placed, while none of the RALUU patients had a Penrose drain placed (P = <0.0001). There was no difference in the need for a secondary procedure for stent removal between the two groups (P = 0.99). All patients in both groups had a Foley catheter placed intraoperatively.
There was no significant difference in mean operative times between the two groups (inclusive and exclusive of cystoscopy with stent placement) (P = 0.20 and P = 0.92, respectively) (Table 2). The only additional procedures performed concurrent to the UU were a laparoscopic contralateral heminephrectomy during one RALUU case and a laparoscopic appendectomy and contralateral ureteral reimplantation in two separate OUU cases that were all excluded from the operative time analysis. Mean estimated blood loss was equivalent between the two groups (P = 0.54). There were no cases of conversion to open in the RALUU group and only one intraoperative complication in the OUU group where a vaginal injury occurred. Robotic cases had slightly shorter lengths of hospital stay at a mean of 1.6 days versus 2.1 days in the open group (P = 0.04).
Postoperative complications included four febrile urinary tract infections in each group and one recurrence of nonfebrile urinary tract infection in the open group. In addition, one 6-month-old OUU patient was found to have more severe hydronephrosis on initial follow-up imaging. On further investigation, a postoperative ureterovesical junction obstruction developed in the patient from creation of an intimal flap during attempted stent placement that necessitated temporary nephrostomy tube placement.
Finally, of all patients with preoperative hydronephrosis (n = 22 in the RALUU group and n = 17 in the OUU group), RALUU had higher rates of improved or resolved hydronephrosis or improved drainage compared with OUU on initial follow-up imaging (P = 0.03) at a mean time interval of 10.2 weeks from surgery for robotic cases and 7.9 weeks for open cases (P = 0.42). This may be because of the moderate, negative correlation seen between use of ureteral stent from robotic cases and degree of postoperative hydronephrosis (rho = −0.53). In addition, the degree of hydronephrosis improvement between the two groups was similar (Fig. 1).
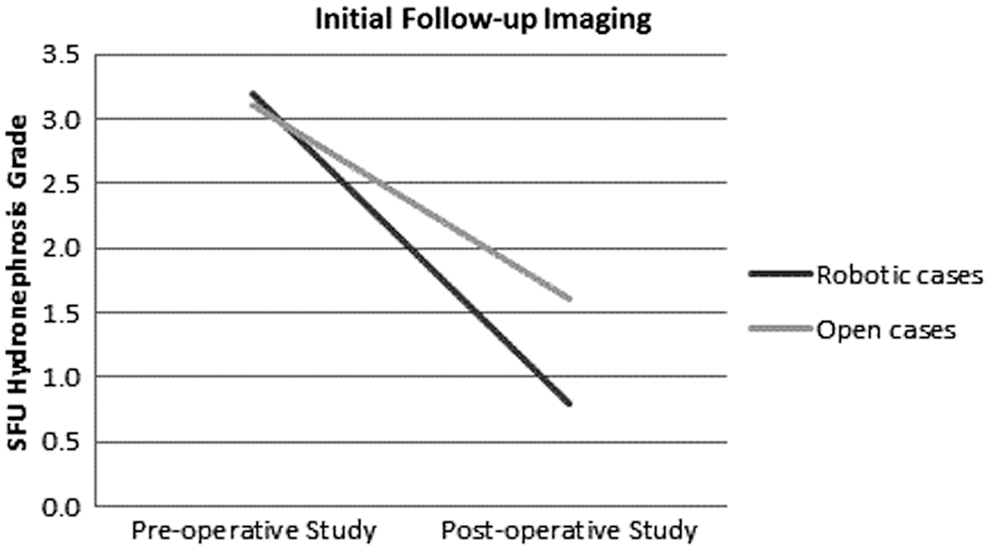
Mean Society of Fetal Urology (SFU) hydronephrosis grade preoperative and postoperative for robot-assisted and open ureteroureterostomy cases.
While all patients undergoing RALUU were imaged with ultrasonography after the surgical procedure, three patients undergoing OUU were imaged with diuretic renography, and all showed improved drainage. These results did not change on subsequent available imaging studies except in two patients, both in the open cohort. The one OUU patient with worse hydronephrosis from ureterovesical junction obstruction eventually showed improved drainage on diuretic renography after removal of the nephrostomy tube 6 weeks after placement. Another OUU patient initially showed stable hydronephrosis postsurgery but later a diuretic renogram revealed improved drainage. Mean overall follow-up was similar between the two groups (16.4 months for RALUU vs 11.6 months for OUU, P = 0.30).
Discussion
UU has been shown to be an effective intervention for the management of anomalies associated with ureteral duplication. 8 As minimally invasive surgical techniques have advanced, both laparoscopic and robot-assisted laparoscopic surgical procedures have been successfully introduced into the pediatric population. 1 While many descriptive studies have demonstrated the safety and efficacy of RALUU in pediatric patients, 4 –6 our study aimed to compare outcomes of RALUU versus OUU.
The RALUU outcomes of our study with regard to length of stay, operative times, and complications were comparable to those in the existing literature. 4 –6 The more recent modified laparoscopic UU studies do report slightly shorter operative times and lengths of stay. 9,10 Grimsby and associates 9 introduced a new laparoscopic technique that delivered the duplex ureters through a small inguinal incision for an extracorporeal anastomosis and reported a mean length of hospital stay of less than 24 hours for both laparoscopic and open cases. These authors compared their new laparoscopic surgical technique with their open cases and found no difference in operative time, length of stay, complication, or success rate. 9
Within our cohort, our RALUU patients were most often discharged the day after operation, and on postoperative day 2 for those undergoing OUU. It is unclear whether this discrepancy is because of quicker recovery times in the aforementioned studies or the results of different conventions of individual surgeons or institutions. Current literature does not specifically state criteria for discharge. Within our dual institution study, length of stay was decreased by 0.5 days in the RALUU patients.
Overall, our patient demographics did not differ significantly between the RALUU and OUU groups. It was notable, however, that distal anastomoses near the level of the bladder were performed more for the OUU patients, while proximal anastomoses were performed more often in RALUU patients (P < 0.05). The choice of location of the anastomosis is multifactorial, including surgeon preference, degree of ureteral dilation, and location of the surgical scar for the open cases.
All patients in the RALUU group did undergo cystourethroscopy and ureteral stent placement before the robotic procedure, and six of these patients needed a second procedure for stent removal. The decision to leave a stent with an extraction string and duration of stent placement were surgeon dependent. While all RALUU patients had a ureteral stent placed intraoperatively, only eight (42%) patients in the open group had a stent placed; however, these patients were more likely to have a Penrose drain placed (74% vs 0% in the robotic cases). Studies may be warranted regarding the necessity of ureteral stent placement in the minimally invasive approaches. It is the authors' impression that stent placement provides greater assurance of early drainage without urinary leakage. Using an extraction string has been effective in the great majority of patients and avoids the need for a second anesthetic.
Although there was no difference in complication rates between the two groups, there was more improvement of hydronephrosis or drainage on imaging in the robotic cases (86%) compared with the open cases (53%). There was no significant difference in the time interval between operation and imaging between the two groups. Of note, within our practice, ultrasonography is the primary modality for imaging after UU surgery, and all RALUU patients were followed with postoperative ultrasonography. Three of the OUU patients were initially re-imaged with diuretic renography for which all showed improved drainage.
It is possible that a difference was seen in postoperative imaging between the two groups because of the moderate, negative correlation seen between use of an indwelling stent (mostly used in robotic cases) and degree of postoperative hydronephrosis. In addition, our overall sample size was small given that several patients did not have imaging after operation. Although there were a larger number of patients with stable hydronephrosis in the open group, the drainage pattern was unknown given the lack of renography.
As shown in Figure 1, the degree of hydronephrosis improvement between the two groups was similar. There did not appear to be any patients who needed repeated surgery because of a failed procedure in either group within the follow-up time. Also, of all patients, only one patient (from the open cohort) actually showed more severe hydronephrosis because of failed stent placement on follow-up imaging. After nephrostomy tube placement because of ureterovesical junction obstruction, the follow-up nephrostogram at 6 weeks revealed passage of contrast easily into the bladder, and the nephrostomy tube was removed. Given the variability in times of the resolution of hydronephrosis and/or drainage, it is reasonable to infer that the success rate of robotic surgery, based on imaging, is more likely equivalent as opposed to superior to open surgery.
Our results support the current accepted practice that the use of the RALUU has comparable outcomes to OUU for children with duplication anomalies and single system obstructed ureters. The use of robotics in the pediatric population is still in its infancy, and the question of cost-effectiveness within this procedure is still not established. Limitations of our study include our retrospective analysis and overall small sample size.
We attempted to increase our sample size by collaborating between two institutions. Given that UU is one of several ways to manage duplication anomalies, however, the numbers of cases are limited, and the decision to perform this surgery over other alternatives is mainly surgeon dependent. In addition, the decision to perform a robotic versus open approach is surgeon dependent, and therefore this variability may affect overall outcomes. It is somewhat reassuring that our patient demographics between the two groups were similar, limiting selection bias.
Further investigations are certainly warranted to study the role of robotic surgery for the correction of ureteral duplication anomalies using standardized selection criteria and more robust outcomes analysis.
Conclusion
RALUU may be a safe and effective alternative to open operation for children with duplication anomalies and single system obstructed ureters. We found comparable operative times, estimated blood loss, and complication rates with slightly shorter lengths of hospital stay and higher rates of improved hydronephrosis or drainage during initial follow-up imaging (possibly because of increased stent use) within our robotic cohort compared with OUU. Large-scale and prospective studies are still warranted to demonstrate a superiority of one technique over another in addition to realistic cost comparisons.
Footnotes
Acknowledgments
We would like to acknowledge Hannah Agard, MD, for contributions in data collection for the study. We would also like to acknowledge the surgeons who performed the surgical procedures in the study including H. Gil Rushton, MD, Hans Pohl, MD, S. Scott Sparks, MD, and Naida Kalloo, MD.
Author Disclosure Statement
No competing financial interests exist.