
Abstract
Purpose:
We evaluated the use of periureteral injection of botulinum toxin type A (Botox®, BTX-A) to facilitate passage of ureteral stones in a porcine model. We believe that reducing detrusor muscle tone around the intramural ureter may facilitate passage of ureteral stones through the ureterovesical junction.
Materials and Methods:
With complete Institutional Animal Care and Use Committee approval, artificial stones (BegoStone plus) were placed by retrograde ureteroscopy into the proximal ureter using fluoroscopic guidance using an in-vivo porcine model. Six animals underwent periureteral BTX-A injection 30 U/mL to three locations around the ureteral orifice, and six animals were in the control group undergoing periureteral injection of physiologic saline.
Results:
There was a significant decrease in time to stone passage in the BTX-A group compared with the control group, 2.6 ± 1.3 vs 6.8 ± 2.9 days, respectively (p = 0.018). None of the animals had evidence of vesicoureteral reflux postprocedure (N = 0/12).
Conclusions:
Preliminary results suggest that periureteral injection of BTX-A facilitates ureteral stone passage in this model. BTX-A may provide a simple, office-based endoscopic treatment option for ureteral stones. Further studies would be necessary to evaluate its efficacy in humans compared with traditional medical expulsive therapy.
Introduction
M
The botulinum toxins are derived from the gram-positive coccus Clostridium botulinum. 5 Botulinum toxin type A (Botox®, BTX-A) is an inhibitor of presynaptic acetylcholine release that causes a flaccid paralysis of striated and smooth muscle. 5 Its function derives from its ability to cleave SNAP-25, a type of SNARE protein, which is essential for synaptic vesicle fusion that releases acetylcholine. 5 BTX-A was introduced in 2000 as a treatment option for overactive bladder with injections into the bladder causing relaxation. 6 In 2010, theorizing that stent-related symptoms may be due to detrusor muscle spasm in and around the intramural ureter, Gupta et al. have suggested a role for periureteral injection of BTX-A to decrease pain associated with ureteral stents. 7
Our hypothesis is that periureteral injection of BTX-A decreases detrusor muscle tone around the intramural ureter and facilitates passage of ureteral stones through the UVJ, decreasing time to ureteral stone passage. To evaluate the effects of this intervention, we conducted a controlled trial of ureteral stone passage in a novel porcine model with endpoints of stone passage rates, time to stone passage, and cystogram-assessed vesicoureteral reflux (VUR).
Materials and Methods
The study was approved by the University of Wisconsin–Madison Institutional Animal Care and Use Committee. A total of 12 mixed, large, white, female gilt pigs weighing 50–60 kg underwent ureteroscopic placement of an artificial stone into the proximal ureter after general anesthesia was induced with Telazol (7 mg/kg IM), xylazine (2.2 mg/kg IM), and atropine (0.05 mg/kg IM). Endotracheal intubation was then performed and anesthesia was maintained with isoflurane; propofol (4–6 mg/kg IV) was utilized as a supplemental anesthetic during the procedure as needed. Animals were placed in a dorsal lithotomy position and prepped according to clean–contaminated surgical principles (Fig. 1). Preprocedural cefazolin (1 g IV) was administered.

Surgical positioning female pigs were placed in a dorsal lithotomy position under general anesthesia with endotracheal intubation. C-arm fluoroscopy was utilized for endoscopic placement of an artificial ureteral stone. Color images available online at
The artificial stones were made of BegoStone plus (Bego USA, Smithfield, RI), which has been previously shown to have similar mechanical properties as the most common type of kidney stones in humans, calcium oxalate. 8 BegoStone does not soften in urine and is ideal for artificial stones in live animal studies. 8 A mold was developed to make 5 mm artificial stones using a human stone fragment to give an irregular surface contour (Fig. 2). A mixture of 5 g BegoStone to 1 mL water was used. To make the artificial stones densely radiopaque for monitoring of stone passage by fluoroscopy, we placed a thin flexible metallic wire into the center of the stone mixture. The stones were allowed to harden within the mold for at least 24 hours before use.
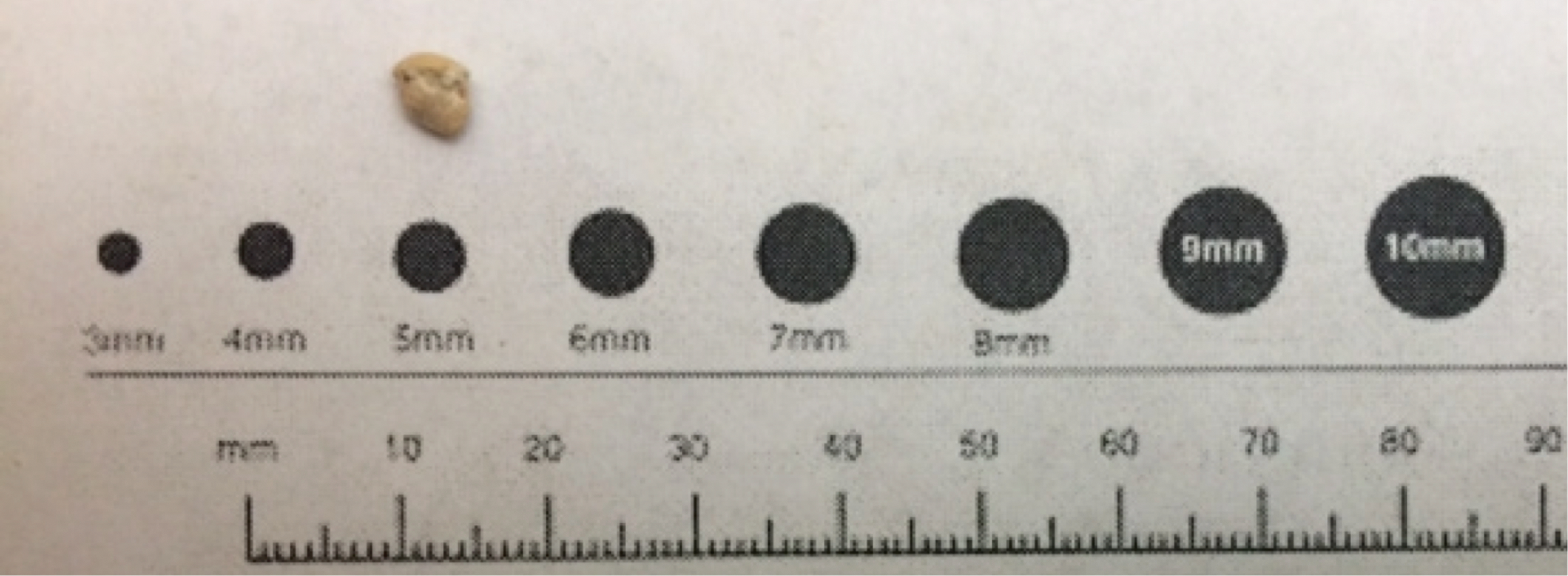
Five millimeter artificial stone. The artificial stones were made from BegoStone with use of a mold to create irregular contour and 5 mm in size. A thin metallic wire was inserted in the center of the stone to make it densely radiopaque. Color images available online at
Flexible cystoscopy (Olympus CYF-3; Olympus Medical Systems Corp., Tokyo, Japan) was performed to identify the ureteral orifice, and a hydrophilic-tipped guidewire was passed under C-arm (OEC 9800; General Electric Healthcare, Cleveland, OH) fluoroscopic guidance to the level of the renal pelvis (Fig. 3). A 5F ureteral access catheter was advanced over the wire to the proximal ureter to perform a retrograde pyelogram using contrast to confirm proper placement of the guidewire. A stiff guidewire was then placed, and a ureteral access sheath 12/14F was placed over the guidewire into the distal ureter. The 5 mm artificial stone was placed within an NCircle® basket (Cook Medical, Bloomington, IN) through the sheath with the flexible ureteroscope (Olympus URF type P2; Olympus Medical Systems Corp.). After the stone was deposited in the proximal ureter (between L3 and L4 vertebrae) with visual and fluoroscopic confirmation, all devices were removed.
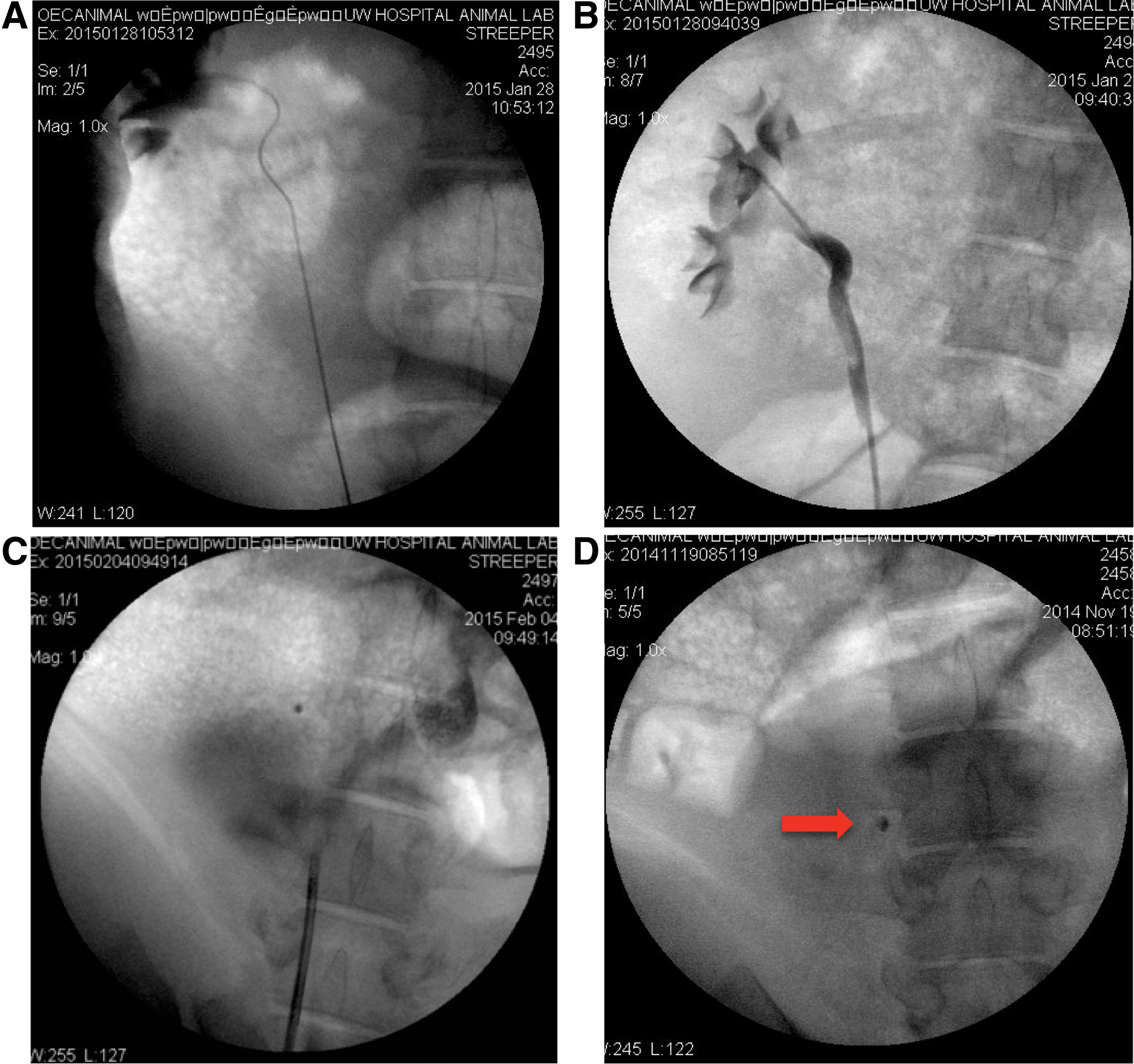
Endoscopic placement of artificial stone using fluoroscopy. A hydrophilic guidewire was passed under fluoroscopic guidance to the level of the renal pelvis
Six pigs were included in the intervention arm, and a flexible cystoscope with a flexible needle was used to inject 30 U/mL of BTX-A into the ipsilateral periureteral detrusor in three locations (medial, lateral, and inferior to ureteral orifice) for a total of 90 U in 3 mL. This concentration was made by mixing 3.3 mL of physiologic saline with one vial, 100 U of BTX-A. The control group, six pigs, received three similar ipsilateral periureteral 1 mL injections of physiologic saline for a total of 3 mL.
Every 2–3 days, stone position was monitored through fluoroscopic imaging of the animals under sedation. In addition, the animals were monitored daily by our animal care team for signs of pain, including increased irritability, vocalization, lack of appetite, lethargy, and reluctance to move. All animals received a nonsteroidal anti-inflammatory drug (NSAID), flunixin (1 mg/kg IM), at the time of stone placement. Additional pain medication (carprofen or fentanyl patch) was available in the protocol, but none of the animals needed additional analgesics. We evaluated renal function and hydration status using urine-specific gravity (SG), which was collected preprocedure and after stone passage. After passage of the stone, we performed a cystogram using 240 mL of contrast under gravity to evaluate for VUR. The animals were subsequently euthanized.
A t-test was used to compare days to stone passage between the two groups. The paired t-test was used to compare pre- and postprocedure creatinine level and urine SG. A p-value <0.05 was considered to be significant.
Results
All of the animals passed their stones with an overall time to stone passage of 6.3 ± 4.6 days. The BTX-A group (N = 6) had an average of 4.5 ± 4.8 days to stone passage, compared with 8.0 ± 3.9 days in the control group (N = 6) (p = 0.196). The data points were placed on a scatter plot, and there were two animals that, one in each arm of the study, were more than 1.5 standard deviations (SD) above the overall average (Fig. 4). After removal of these two animals, the BTX-A group (N = 5) had an average of 2.6 ± 1.3 days to stone passage, which was significantly less than the control group (N = 5) at 6.8 ± 2.9 days (p = 0.018). There was an animal in the control group with a time to stone passage of 2 days, which was >1.5 SD below the group average (Fig. 4). Upon removal of this animal, the BTX-A group (N = 5) time to stone passage remained significantly less than the control group (N = 4, 8.0 ± 1.2 days, p < 0.001).

Days to stone passage. The circles represent the control group, and the diamonds represent the BTX-A group. The y-axis plots the days to stone passage for each animal on the x-axis, and the error bars represent ±1 standard deviations (SD). The BTX-A group (N = 6) had an average of 4.5 ± 4.8 days to stone passage, compared with 8.0 ± 3.9 days in the control group (N = 6) (p = 0.196). Two animals, one in each arm of the study, were more than 1.5 SD above the overall average. After removal of these two animals, the BTX-A group's days to stone passage were significantly less than the control group (p = 0.018). There was an animal in the control group with a time to stone passage >1.5 SD below the group average. Upon removal of this animal, the BTX-A group's time to stone passage remained significantly less than the control group (p < 0.001). BTX-A, botulinum toxin type A. Color images available online at
None of the animals had evidence of VUR on cystogram after stone passage. No adverse reactions such as urinary retention, renal failure, infection, or allergic reactions occurred. There was no need for postprocedure carprofen or fentanyl patch for additional pain medication, as none of the animals displayed signs of pain.
There was no difference between the BTX-A and control group in the average urine SG preprocedure (1.01 ± 0.004 vs 1.01 ± 0.004, p = 0.74), urine SG post-stone passage (1.01 ± 0.010 vs 1.02 ± 0.005, p = 0.39), creatinine level preprocedure (1.13 ± 0.1 vs 1.13 ± 0.1, p = 1.0), or creatinine level post-stone passage (1.26 ± 0.2 vs 1.38 ± 0.18, p = 0.36). In addition, there was no difference in the overall change of creatinine or urine SG values between the groups throughout the study period, p = 0.79 and 0.33, respectively.
Discussion
To our knowledge, this is the first study to examine the effects of periureteral injection of BTX-A on the passage of ureteral stones. These preliminary results demonstrate that the use of BTX-A periureteral injection decreases the time to passage of ureteral stones.
BTX-A is a potent inhibitor of presynaptic acetylcholine release, inducing muscle paralysis that is harnessed in a variety of FDA-approved medical indications, including dystonias, blepharospasm, chronic migraine headache, and detrusor overactivity. 9 –12 The drug's mechanism of action has already become familiar to the urologic community as an alternative to chronic oral anticholinergic therapy for overactive bladder, but has also been reported and widely used for other urologic applications such as detrusor sphincter dyssynergia (DSD) and chronic pelvic floor pain. 13,14 While the introduction of alpha antagonists as MET agents has significantly changed the modern management of ureteral stones, there remain patients who still require surgical intervention for their stones. In this regard, BTX-A may provide a promising addition to the armamentarium available to urologists, particularly since BTX-A injection in an office setting has already been reported for conditions such as DSD and esophageal dysfunction. 15,16
The porcine model has been previously utilized to evaluate pharmacologic effects on the ureter and found to replicate human ureteral responses, including ureteral relaxation with alfuzosin, doxazosin, vardenifil, nifedipine, verapamil, theophylline, and hydrocortisone. 2,17 –21 The urinary systems of pigs are similar to humans, including having striated muscle in the bladder. In addition, previous research describes the feasibility of flexible ureteroscopy in the female pig with endoscopic placement of artificial stones. 22,23 This study provides the basis for further investigation of BTX-A in the human model.
There is a theoretical risk that paralysis at the ureteral orifice with periureteral injection of BTX-A may cause temporary VUR. However, none of the animals had VUR demonstrated on cystogram postinjection. Other potential risks would include bleeding at injection site, pyelonephritis, and urinary retention if there is diffusion of BTX-A to other areas of the bladder. None of the animals demonstrated postprocedure adverse reactions. There was no difference in pre- and post-stone passage urine SG or creatinine level, suggesting that the animals maintained adequate hydration status and medications did not affect renal function.
Limitations of the study include the following: small sample size, use of ureteral access sheath for placement of stone, porcine anatomy that is similar, however, not identical to humans, and use of an NSAID and imaging to evaluate stone passage was every other day. The small sample size was likely the reason for a lack of significance in the unadjusted calculations. Use of a ureteral access sheath was necessary to be able to advance the stone in a retrograde manner. The insertion of the sheath may have had an effect on stone passage through the UVJ; however, no dilation of the orifice was necessary before placement for the animals included in the final analysis. It is unknown what effects the ureteral access catheter had on the ureteral orifice, whether there was sustained dilation or a degree of edema and whether this varied among the animals. Both groups were treated equally, but this is a limitation of our study. As seen in the human population, there was a variance in the caliber of the porcine ureters. Two animals had narrow caliber ureters making stone placement difficult. Both of these animals had a time to stone passage of 14 days, >1.5 SD from the overall average. There was one animal in the control group that had a capacious ureter, and the time to stone passage was 2 days, >1.5 SD below the group average. It may be useful in future studies to compare the caliber of the distal ureter/UVJ among animals using a focused retrograde pyelogram, which may also be used to evaluate the effect of a ureteral access sheath for stone placement. Use of a NSAID may be a potential confounder, but all animals received the same dosing regimen. Daily imaging would be preferable to evaluate more precisely the number of days to stone passage; however, this would have required daily fasting before administration of the sedation required for imaging acquisition, possibly leading to malnourishment of the animals. Future studies in humans would allow for more frequent imaging to more precisely evaluate stone migration, and time to stone passage, of BTX-A injection compared with traditional MET.
We believe that cystoscopic periureteral BTX-A injection may provide an office-based option that may facilitate passage of ureteral stones and obviate the need for surgical intervention. This may be beneficial for patients who are poor surgical candidates or in patients who want to avoid the additional risks of surgery. The procedure is straightforward, using a flexible needle through a flexible cystoscope in both sexes. A vial of 100 U of BTX-A (Botox) costs approximately $400. Further studies would be necessary to evaluate the cost-effectiveness and appropriate indications compared with other treatment modalities.
Conclusions
Periureteral injection of BTX-A improved stone passage of ureteral stones in the porcine model. This study provides a proof of concept on which subsequent investigations may be modeled. Further studies would be necessary to evaluate its efficacy in humans compared with traditional MET.
Footnotes
Author Disclosure Statement
No competing financial interests exist.