
Abstract
Introduction:
Flexible ureteroscopy (fURS) is increasingly used in the treatment of renal stones. However, wide variations exist in technique, use, and indications. To better inform our knowledge about the contemporary state of fURS for treating renal stones, we conducted a survey of endourologists worldwide.
Methods:
An anonymous online questionnaire assessing fURS treatment of renal stones, consisting of 36 items, was sent to members of the Endourology Society in October 2014. Responses were collected through the SurveyMonkey system over a 3-month period.
Results:
Questionnaires were answered by 414 surgeons from 44 countries (response rate 20.7%). U.S. surgeons accounted for 34.4% of all respondents. fURS was routinely performed in 80.0% of institutions, with 40.0% of surgeons performing >100 cases/year. Respondents considered fURS to be first-line therapy for patients with renal stones <2 cm and lower pole calculi. A substantial minority (11.3%) preferred fURS as a primary treatment modality for renal stones >2 cm. Basket displacement for lower pole stones was routinely performed by 55.8%. Ureteral access sheaths (UAS) were preferred for every case by 58.3%. Respondents frequently utilized high-power lasers and dusting techniques. Criteria for determining stone-free rate were defined as zero fragments or residual fragment (RF) <1, <2, <3, and <4 mm by 30.9%, 8.9%, 31.5%, 15.8%, and 11.2% of respondents, respectively.
Conclusion:
The overwhelming majority of endourologists surveyed consider fURS as a first-line treatment modality for renal stones, especially those <2 cm. Use of UAS, high-power holmium lasers, and dusting technique has become popular among practitioners. When defining stone free after fURS, the majority of endourologists used a zero fragment or RF <2 mm definition.
Introduction
T
Despite recent population-level evidence demonstrating increasing utilization of fURS, 2 –4 little information exists on contemporary practice patterns of fURS for the treatment of renal calculi. 5 While guidelines recommend fURS for treating renal stones <1.5 cm, 6 considerable differences exists among urologists in the technique, use, and indications of fURS. In particular, the variation in the use of disposable equipment, such as ureteral access sheaths (UAS) or nitinol retrieval devices, and the utilization of more powerful high-watt holmium laser systems in the modern era of fURS, have not been thoroughly evaluated. Recently, the European Association of Urology (EAU) conducted a survey on the use of fURS for the treatment of renal calculi in Europe. 5 To study a broader collection of urologists throughout the world, we modified this questionnaire and surveyed members of the Endourology Society about multiple facets of renal calculi treatment using fURS. Our specific aim was to explore differences in the fURS technique and practice among endourologists.
Methods
In October 2014, an anonymous online questionnaire characterizing fURS use in the management of renal stones was disseminated to all members of the Endourology Society through e-mail. The survey instrument contained 36 discrete questions divided into six domains to capture demographic information, level of surgeon experience, indications, surgical technique, postoperative stent management and tracking, and postsurgical follow-up. Questions were multiple choice with the option for free text responses. See Appendix for details on questions asked. Respondents were further subdivided based on region of residence for descriptive purposes such that those from North America, Europe, and other regions could be compared with respect to various responses.
The survey was conducted using the web-based SurveyMonkey system (Palo Alto, CA). Respondents were invited to participate through an introductory email from the Endourology Society membership office with a brief description of the survey and a hyperlink of the survey. A second reminder e-mail was sent a month later and the survey remained open for 3 months. The survey was deemed exempt from requiring review by the Institutional Review Board at the University of Michigan. To improve participation, a $200 award was offered to one respondent selected at random. The study was funded by the Endourology Division of the Department of Urology, University of Michigan.
Results
The survey was disseminated to ∼2000 members of the Endourology Society; 414 (20.7%) responded. Those responding represented 44 countries with the largest percentage of respondents practicing in the United States (34.4%), United Kingdom (9.8%), and Canada (5.3%) (Table 1). More than 60% of respondents were between the ages of 40 and 59; 2% were <30 years, 23% were between 30 and 39 and 14% were older than 60 years. Approximately 60% of respondents had completed an endourology fellowship, while 80.5% indicated they were a subspecialist with an interest in urinary stone disease.
The case volume of fURS performed annually is depicted in Figure 1; nearly 40% of respondents performed fURS more than 100 times per year. fURS was performed routinely in the institution of 80% of respondents.
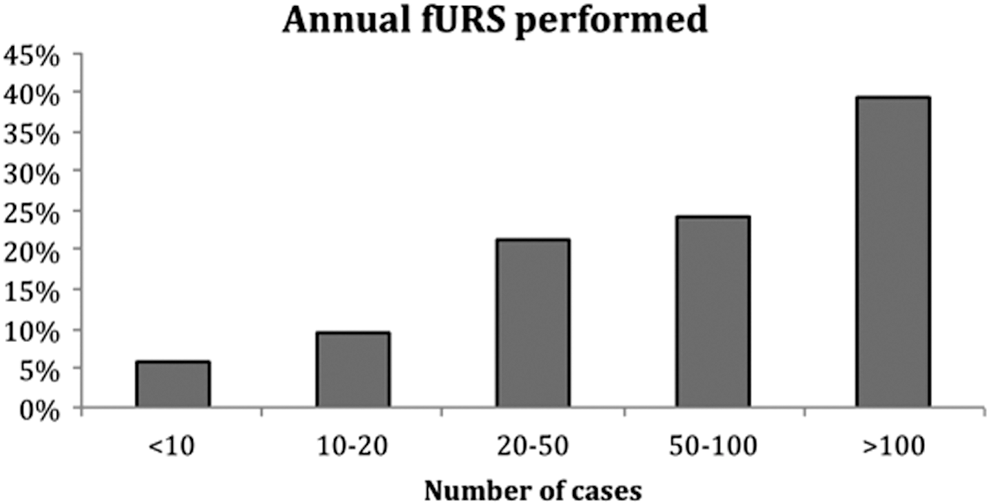
Number of flexible ureteroscopies (fURS) performed annually.
Indications and planning
With regard to indications and surgical planning, respondents overwhelmingly (96.4%) felt that fURS could be used as a first-line modality to treat renal stones. To this effect, there was a wide range of clinical situations in which respondents felt that fURS was an appropriate primary treatment, the most popular being stone in horsehoe kidney (72.1%) and stone in the lower pole (71%) (Fig. 2). Patients were considered for staged fURS (more than one URS planned in advance) when the renal stone size (cm) was 1–1.5 (9.7%), >1.5 (20.2%), >2.0 (27.0%), and >2.5 (16.3%).

Clinical scenarios in which fURS is appropriate first-line treatment for renal stones.
Surgical technique
When examining techniques, there was variability in the way urologists approached the ureteral orifice before advancing the ureteroscope. Whereas some placed working and/or safety wires (38.0%), others first performed semirigid ureteroscopy (19.7%), retrograde pyelogram (14.6%), or placed a UAS (25.7%). Only 1.9% of respondents performed fURS without a wire.
In the event that the ureteroscope was unable to be advanced beyond the ureteral orifice, 27.6% of respondents stated they would dilate the orifice with ureteral dilators, 27.4% stated they would dilate with a semirigid ureteroscope, 25.5% stated they would place a ureteral stent and arrange for fURS at a later date, 18.2% would perform balloon dilation of the ureteral orifice, 1.1% would switch to another treatment modality, and 0.2% would perform a ureterotomy.
UAS/basket retrieval
Indications for use of UAS during fURS are provided in Figure 3, with 58.3% of respondents stating that they prefer to use a UAS for every case. With regard to the strategy of whether to retrieve stone fragments or not, 26.7% of respondents actively retrieved all stone fragments, whereas 37.4% only retrieved large fragments—leaving those that were small enough to pass spontaneously (Fig. 4). When dealing with stones in the lower pole, most (55.8%) routinely used the basket displacement technique to move stones to a less dependent calix for fragmentation.

Indications for ureteral access sheath during fURS.
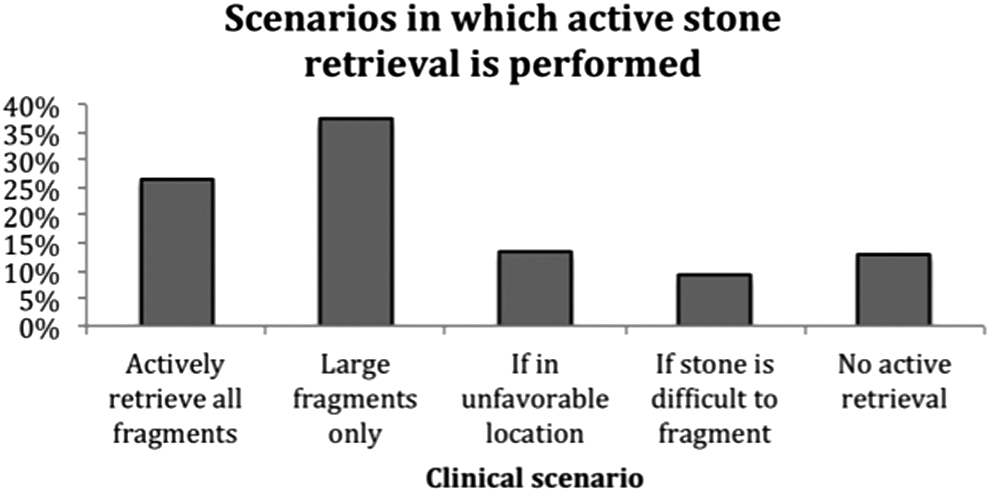
Responses to the questions “Regarding fragmentation of a stone and whether to retrieve fragments or not, what is your typical strategy?”
Holmium laser
Respondents uniformly utilized a holmium laser for stone fragmentation, and the vast majority worked in centers that owned their own laser (85.6%). High-power systems (≥100 W) were utilized by 41.1%, while lower power (20–30 W) systems were used by 44.2%. The majority of respondents (54.8%) preferred a 200-μm laser fiber size as their go to fiber. The dusting technique (i.e., low pulse energy and high frequency 0.2–0.5 J × 30–50 Hz) was used by 67% of the respondents.
Postprocedural aspects
Respondents indicated that in their practice, following completion of fURS, a ureteral stent was placed in all cases 63.9% of the time, whereas the remainder stated that a ureteral stent was only placed if warranted by intraoperative factors. Only 42.8% of respondents indicated that their practice maintained a stent registry to keep track of indwelling stents in patients (Fig. 5). Finally, respondents indicated that an abdominal radiograph, in combination with ultrasonography (40.8%), abdominal radiograph alone (32.8%), computed tomography (24.7%), or ultrasound alone (1.7%), was used to assess stone burden following fURS. The time point at which imaging was undertaken to assess the stone-free rate (SFR) varied (Fig. 6). Table 2 demonstrates the variation among urologists for determining what fragment size is important for defining the SFR.
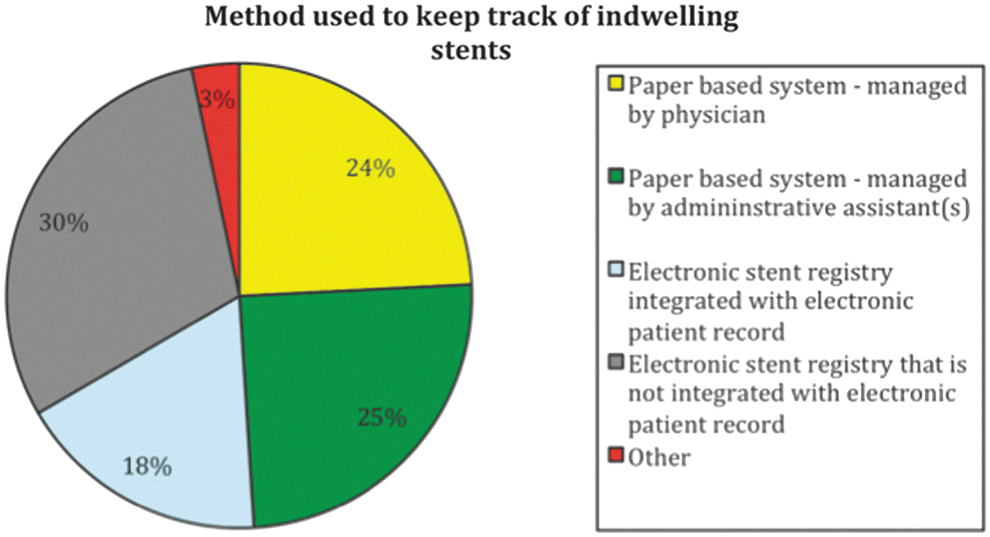
Strategies for ureteral stent management and tracking.
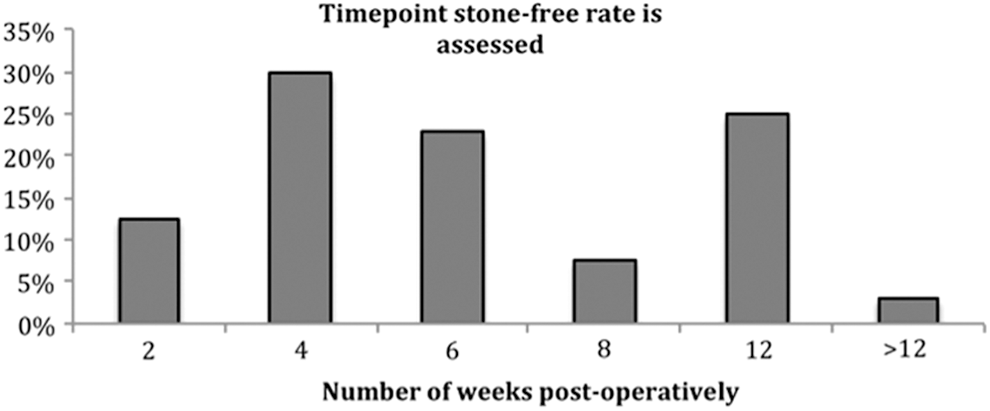
Time point after fURS when stone-free status is determined.
Variation in technique by geographic location
After subdividing respondents by location of residence (North America, Europe, other), differences were noted with regard to selected questions as indicated in Table 3.
For some questions, the two most common responses are provided for comparative assessment.
fURS = flexible ureteroscopy; KUB = kidney, ureter, and bladder radiograph; UAS = ureteral access sheaths; XR = X-ray; US = ultrasound.
Discussion
The present survey-based study was conducted to better understand the worldwide variation in the fURS technique and clinical practice. In summary, the majority of urologists who responded were fellowship trained and many estimated a volume of more than 100 procedures performed annually. Most respondents felt fURS was applicable to a wide range of clinical scenarios, including varying stone size, stone location, and anatomic variations. Furthermore, respondents routinely used UAS and were familiar with high-watt holmium lasers for fURS, as well as using new techniques such as dusting for stone fragmentation.
One interesting observation highlighted by the survey results was that urologists find fURS to be an acceptable surgical technique for a wide range of indications. Recent EAU guidelines state that fURS is a reasonable option for treatment of renal stones <2 cm. In the present study, more than 10% of respondents indicated that fURS was considered an appropriate treatment for stones >2 cm, a size that traditionally would be managed through PCNL. Moreover, despite a nonstatistical difference in SFRs reported in the prospective randomized controlled study comparing SWL with ureteroscopy for lower pole stones <1 cm, 71% of respondents felt fURS was the first-line therapy in this situation. 7
Two recent studies have demonstrated that fURS is a reasonable approach for renal stones >2 cm. In a meta-analyses of urinary stones >2 cm managed by fURS, Aboumarzouk et al. found that for a mean stone size of 2.5 cm, SFRs were 93.7% with a major complication rate of 5.3%. 8 A similar study by Breda and Angerri for stones >2.5 cm showed an overall SFR of 89.3% with a major complication rate of 8%. 9 The average number of treatments required per patient was 1.6 in each study. These studies highlight that the combination of technologic advances and endourologic expertise may be broadening the application of fURS, a clinical impression reflected by our survey.
Another observation made from our study was the frequency with which surgeons utilized the UAS. More than half of respondents indicated in the survey that they used a UAS for every case, whereas an additional 25% used it in selected clinical scenarios. Advantages of the UAS include improving longevity of the flexible ureteroscope 10 as well as decreasing intrarenal pressure during fURS. 11 The UAS is often used to ease stone retrieval, as noted by 31.0% of respondents. Despite these benefits, outcomes such as SFR, arguably one of the most important indicators of effective fURS, have shown mixed results. L'esperance et al. evaluated 256 patients undergoing fURS for renal calculi stratifying outcomes based on whether a UAS was used or not. The SFR in the UAS group was 79%, significantly higher than the non-UAS group (67%). 12 However, a more recent study did not find use of a UAS to be associated with improved SFRs with stone size being the only variable predictive of SFR on regression analysis. 13 The paucity of evidence is reflected in the variation of use by respondents in our survey.
Our study provided some interesting findings with respect to practice patterns surrounding active stone retrieval vs fragmentation. Specifically, many respondents actively retrieved stone fragments and only a few indicated that they seek to fragment the stone into pieces they feel will pass spontaneously, without any need for extraction. Certainly, debate regarding the optimal fragmentation and retrieval technique has been ongoing. 14 Currently, no Level 1 evidence is available that answers the following question: “should you perform active retrieval or is fragmentation only enough after fURS for renal stones?” More recently, newer laser lithotripsy techniques such as dusting utilizing high-watt holmium systems have been popularized. 15 Dusting uses a high-frequency, low-pulse energy setting, such as 30–50 Hz × 0.2–0.5 J, which seeks to fragment stones to fine powder and small fragments, and thus reduce the need to retrieve fragments. We were surprised to find out that two-thirds of respondents indicated using this technique. So far, there are limited clinical data as to whether this method has significant advantages over existing techniques, and further studies are needed to confirm its utility.
Interestingly, more than 63% of respondents indicated that a ureteral stent was left in place following fURS. There have been numerous clinical trials conducted to investigate the utility of routine ureteral stenting following ureteroscopy. A recent systematic review and meta-analysis by Nabi et al. found that patients in whom a ureteral stent was placed reported higher rates of dysuria, urgency, and frequency without a statistically significant increased SFR, although this was limited by study heterogeneity. 16 Given the uncertainty on this issue and lack of improvement in SFR reported in the meta-analysis, it is notable that so many respondents routinely stent their patients following fURS.
Our study has also provided some important information on determining the preferred method and criteria for determining the SFR after fURS. Approximately 75% used an abdominal radiograph, renal ultrasound, or a combination of the two as the imaging modality of choice for assessing residual stone burden. Most respondents use to perform this within 6 weeks following surgery. Certainly, use of ultrasound following URS is encouraged to rule out silent hydronephrosis, which can occur in up to 2%–5% of patients. 17 –19 Less agreed upon, however, is the definition of SFR following fURS. The term clinically insignificant residual fragment (RF) was introduced for asymptomatic noninfectious RFs <4–5 mm following SWL, and many studies adopted this metric when reporting the success of stone treatment. 20 However, recent computed tomography-based studies have shown that instead of RF ≤4 mm, sizes ≤2 or ≤3 mm might be more appropriate for determining the clinical significance of stone free and risk of retreatment after stone surgery. 21,22 The lack of consensus in our field about imaging utilization and criteria 23 is demonstrated in our study where nearly 30% felt stone free was defined as zero fragments on imaging, whereas the remainder felt RF <1–4 mm was appropriate.
Two prior surveys have investigated practice patterns surrounding upper tract urinary stone treatment use among urologists. 24,25 Bandi et al. surveyed members of the North Central Section of the American Urological Association in 2006 and found that fURS was largely reserved for proximal and distal ureteral calculi. Subcentimeter renal stones were largely managed with SWL, whereas larger stones were managed with PCNL. This is in contrast to our study, where upward of 90% of urologists indicated fURS an appropriate first-line therapy for renal calculi of varying sizes and location. Our results are similar to a recent EAU survey conducted by Sanguedolce et al. wherein 95% of surveyed urologists preferred fURS as first-line therapy for renal calculi for a variety of clinical scenarios, and where also use of UAS was prevalent. 5 Unlike our study, the EAU survey did not assess the use of holmium laser systems or practice patterns on postprocedure imaging and criteria for SFR.
The results of our study are useful in that they depict the demographics and practice patterns of an experienced group of specialty-trained urologists. However, certain limitations must be acknowledged. First, this study represents a highly specialized cohort of urologists, and thus, the findings may not be generalizable to general urologists without specialty training in endourology. In addition, our survey response rate of 21% is suboptimal and may influence the generalizability of our results. Furthermore, due to a general lack of rigorous level-one evidence regarding the benefit of several techniques described in the article (UAS use and dusting), observations from respondents serve more as descriptive findings rather than evidence of appropriate use. Moreover, the cost implications of technologic innovation with lack of proven benefit outside of observational studies must be considered carefully when treating patients with renal stones. Finally, there is always the possibility that due to reporting bias, opinions reflected in this survey do not necessarily mirror clinical practice. Nevertheless, our study response rate is similar to prior endourology surveys, 24 and even higher than more recent ones to Endourology Society members. 25 Finally, it is possible that some urologists may not be fully aware how best to utilize the holmium laser power settings, and further survey-based studies are needed to verify our findings.
Conclusion
The use of fURS for treating renal calculi has expanded such that it is considered first-line therapy by endourologists for varying stone sizes, stone locations, and anatomical variations. UAS, high-power holmium lasers, and dusting technique are now utilized on a regular basis. When defining stone-free status after fURS, the majority of urologists surveyed used a zero fragment or RF <2 mm definition. Although there is consensus regarding certain aspects of fURS technique and practice, several controversies still exist that merit further investigation.
Footnotes
Acknowledgments
We thank Greg Mowatt from the Department of Urology for helping with the IRB application, as well as Michele Paoli from the Endourology Society for assistance with disseminating the survey to its members.
Author Disclosure Statement
Khurshid Ghani is a consultant for Lumenis, Inc., and Boston Scientific.
Abbreviations Used
Appendix—Survey Instrument
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.