
Abstract
Objective:
To understand the effective radiation dose during percutaneous cryoablation (CA) and radiofrequency ablation (RFA) and characterize variables that may affect the individual dose.
Materials and Methods:
The effective radiation dose was determined by conversion of the dose–length product from CT scans performed during percutaneous CA or RFA for patients with solitary renal masses (<4 cm) at four academic centers. Radiation dose per case was compared between patients and institutions using multivariate and univariate analysis. Lifetime attributable risk of cancer was calculated for each institution and utilized to determine the number needed to harm for a range of ages at the time of exposure.
Results:
One hundred twenty-three patients met the inclusion criteria with a mean age of 71 years. Sixty-nine percent of patients were male, mean body–mass index (BMI) was 29.4, and mean tumor size was 2.2 cm. The mean effective radiation dose per ablation was 40 mSv (range 3.7–147). On multivariate analysis, only BMI and institution were associated with the radiation dose. No significant difference in radiation exposure was seen for RFA or CA procedures.
Conclusions:
Radiation exposure during percutaneous ablation is similar to a multiphase CT scan. However, there is wide variability in individual treatment exposure, varying from 3.7 to 147 mSv, depending primarily on institution and BMI. Standardization of protocols is required to achieve as low as reasonably achievable levels of radiation.
Introduction
T
Initially reserved for poor surgical candidates, good intermediate to long-term oncologic outcomes have led to utilization of the technique in younger and healthier patients due to decreased morbidity, minimal blood loss, and improved renal preservation compared to radical and partial nephrectomy. 2 –6 Between 2004 and 2007, RFA and CA utilization rose from 2% to 7.5% for the treatment of T1a renal malignancies, 7 and as of 2008, nearly 95% of academic centers offered some type of ablative procedure. 8
While some percutaneous ablation is performed under ultrasound, the majority of cases are performed with CT guidance. 8 Despite the widespread use of CT imaging for percutaneous ablation, there is a paucity of information available regarding radiation exposure to the patient during these procedures. Recently, Arnold et al. retrospectively reviewed their extensive experience with percutaneous ablation and determined that the average treatment exposure of CA was higher, at 39.7 mSv compared to 22.2 mSv for RFA (p=0.001), likely secondary to additional images required for monitoring of the evolving iceball in CA. 9 While informative, the results from this single-institution series may not accurately reflect experience at other institutions, as there is no established imaging protocol for percutaneous ablations.
Repeated radiation over a patient's lifetime may pose a risk for development of secondary malignancies. 10 Increasing utilization of CT scans has brought a greater focus on minimizing this potential iatrogenic risk. 11 Not surprisingly, patients most susceptible to increased risk of secondary malignancy are those who require surveillance imaging for primary malignancy, such as those with SRM. 12 For this reason, all possible efforts to achieve as low as reasonably achievable radiation dosages should be sought in this susceptible population. To that end, we compared radiation exposure for a cohort of patients undergoing either CA or RFA at four separate academic institutions and evaluated as to which variables can be used to predict radiation exposure.
Materials and Methods
Following the Institutional Review Board approval from each institution (North Shore/Long Island Jewish, University of California, Irvine, University of Iowa, and University of Texas Southwestern), a retrospective review of patients with renal masses <4 cm treated with RFA or CA from January 2010 to May 2013 was performed. All patients were referred to the above institutions for the evaluation and treatment of at least one SRM. They were counseled on treatment options, including active surveillance, percutaneous ablation, and extirpative surgery. RFA and CA were offered when surgically appropriate. All of the procedures were performed with CT guidance and none utilized CT fluoroscopy. The majority of the procedures were performed as joint operations with an interventional radiologist and urologist. Patient demographics (age, gender, and body–mass index [BMI]), tumor characteristics (size, exophytic percentage, distance to collecting system, anterior or posterior location, and RENAL score), and complications were recorded.
The effective dose of radiation delivered to the patient was estimated using previously established methods. 13 Briefly, the dose–length product (DLP) (mGy·cm) for each scan was multiplied by the conversion factor for adult CT abdomen and pelvis CT scans of 0.015 mSv·mGy−1·cm−1, which estimates the amount of intra-abdominal radiation based on the output of radiation from the scanner. 14
Patient and tumor characteristics were compared using univariate analysis with Kruskall–Wallis and chi-squared tests. Multivariate linear regression was performed to determine the predictors of effective radiation dose. All analyses were performed using SPSS version 21.0. Statistical significance was set to 0.05.
Results
A total of 123 patients met the inclusion criteria. Sixty-eight (55%) underwent RFA, while 55 (45%) underwent CA. Median patient age was 71 years (interquartile range [IQR] 63–77). Table 1 lists patient and tumor characteristics. Institutions were statistically similar in age, BMI category, tumor laterality, tumor size category, tumor relationship to polar lines, and total RENAL nephrometry score. At least two institutions varied in the distribution of gender, American Society of Anesthesiologists (ASA) class, exophytic percentage, distance to collecting system, and anterior/posterior location.
p-Value <0.05 indicates that at least two of the institutions have a difference in distribution for that given characteristic.
ASA=American Society of Anesthesiologists; BMI=body–mass index; IQR=interquartile range; RFA=radiofrequency ablation.
Figure 1 demonstrates the effective radiation dose at each institution. On multivariate analysis, only BMI and institution were predictive of dose. Median effective dose was 43 mSv (IQR 9–65) for RFA and 30 mSv, (IQR 21–47) for CA (p=0.59). Institution 1 had the lowest median effective radiation dose of 3.7 mSv (IQR 5–8.2), while institution 2 had the highest median dose of 52.4 mSv (IQR 40–77.3). Both of these institutions utilized RFA. Institutions 3 and 4, which utilized CA, had similar median effective radiation doses of 29.6 (IQR 23.6–47.8) and 30.4 (IQR 18.7–44.6), respectively.

Effective radiation dose per institution. The middle horizontal line denotes median. The box denotes the interquartile range and the whiskers denote maximum and minimum. RFA = radiofrequency ablation; CA = cryoablation.
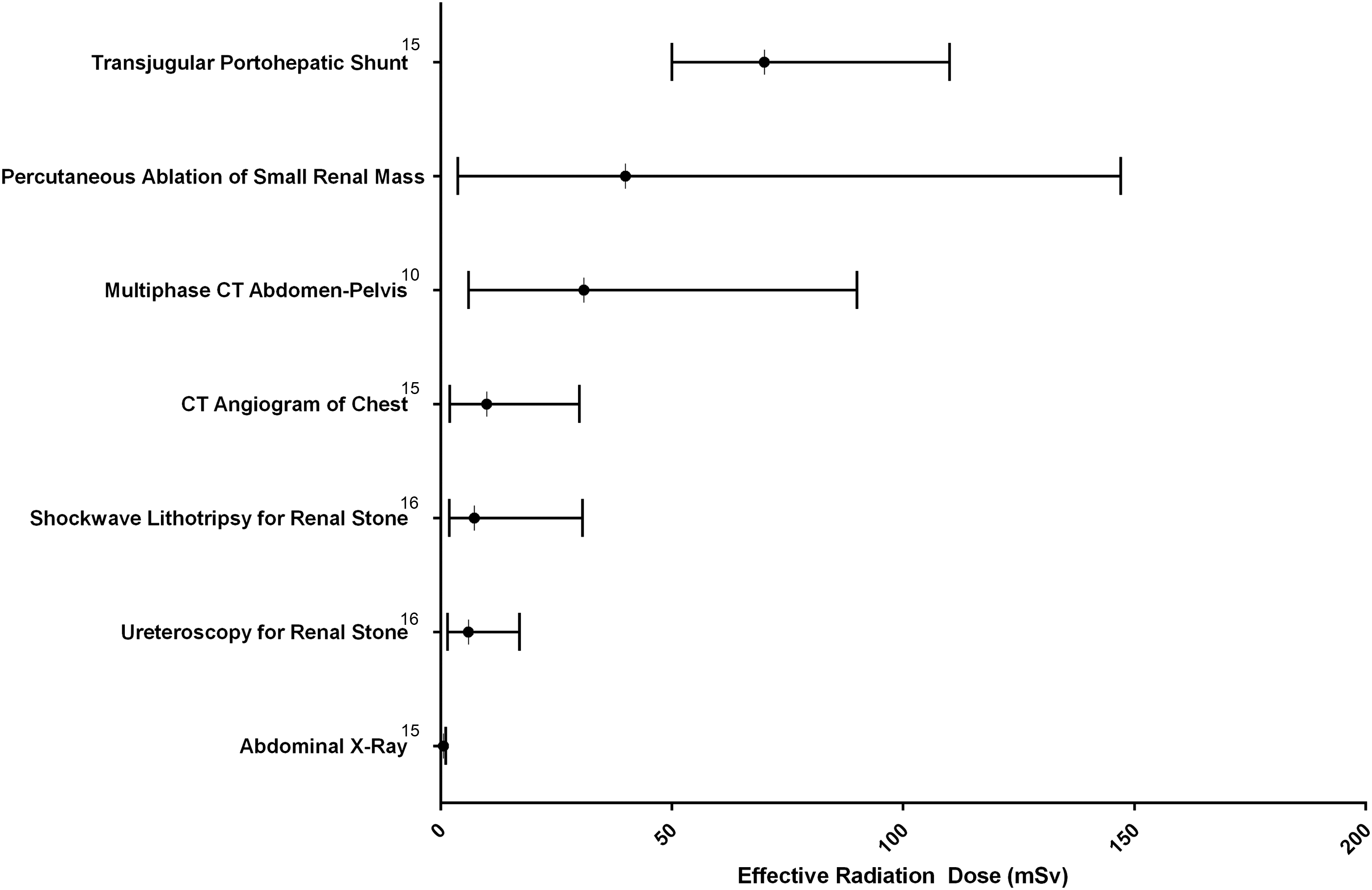
Figure 2 compares the cumulative median effective dose of percutaneous ablation of SRM to previously published radiation exposure during a range of commonly performed diagnostic and therapeutic modalities. 10,15,16 Fluoroscopy-utilizing procedures, such as ureteroscopy and shock-wave lithotripsy, typically result in less radiation than multiphase CT scans or percutaneous ablation of SRM.
Discussion
In the United States in 2006, ∼62 million CT scans were performed for a total of 440,000 person-Sv and dose of 1.4 mSv per person. 17 CT scans accounted for 49% of medical radiation exposure, which has doubled in the past 10–15 years. 18 On average, a noncontrasted CT scan of the abdomen and pelvis for an adult has an effective dose of ∼8–15 mSv, 10,15 whereas a multiphase scan of the abdomen and pelvis (e.g., CT urogram) may deliver as much as 43 mSv, depending on the institution. 11 Among our multi-institutional cohort of 123 patients undergoing percutaneous ablation, the mean effective radiation dose (40 mSv) was most similar to that of a multiphase abdominopelvic CT.
Both patient characteristics and ablative technologies likely contribute to overall radiation during cross-sectional imaging used for percutaneous ablation. Within our cohort of patients, however, the strongest predictor of overall radiation exposure was the institution performing the procedure, and aside from BMI, no other patient or tumor characteristics were associated with increased exposure. Likewise, the choice of technique (CA vs RFA) did not appear to influence total radiation, as the two institutions performing CA had similar exposures, with the RFA institutions on the extremes of the spectrum. In addition, the breadth of the interquartile range was nearly proportionate to the median dose (71%–86% of the median value) for each institution, suggesting that the institutional difference is likely a result of CT technique rather than patient or physician factors.
Arnold et al. recently published their experience in percutaneous ablation at a single institution over a 7-year time span. In their cohort of 41 cases, they demonstrated average radiation exposure of 39.7 mSv for CA and 22.2 mSv for RFA. Despite using a slightly different conversion factor of 0.017 mSv·mGy−1·cm−1, compared to our conversion factor of 0.015, our results were comparable, particularly with regard to CA. However, our study differs significantly as it demonstrates the importance of multi-institutional analysis, which reveals a large discrepancy between various centers of excellence. Furthermore, our study includes a much larger number of patients over a much shorter time period, which decreases the likelihood that technologic advancements in imaging devices could bias results. In addition, while the prior study found no difference in radiation exposure based on tumor diameter, ASA score, age, or gender (which were equivalent in both groups), our larger cohort made it possible to evaluate patient BMI as well as individual tumor characteristics, such as the polarity, exophytic/endophytic nature, anterior/posterior location, in relation to the collecting system, and the aggregate RENAL score.
Estimating the amount of radiation absorbed by the patient during a CT scan has proven to be complex. Using the DLP to calculate the effective dose has been utilized since 2000 and is a quick and convenient method. This method does have its limitations, including the fact that it does not account for patient body habitus as it is based on standardized phantoms of uniform shape. Despite requiring a higher radiation output for obese patients to obtain satisfactory image quality, adipose tissue has a radioprotective effect by shielding the organs and does not result in a proportional increase in organ-specific radiation dose. In other words, not all of the additional radiation that obese patients receive goes to the radiosensitive organs and may not necessarily be more carcinogenic. The effective dose does, however, allow for standardized comparisons of radiation exposure between studies and is quick, readily accessible, and frequently utilized for this purpose. 9,10,13,14,19
The total effective radiation dose limit in the United States established by the Nuclear Regulatory Commission is 50 mSv/year. 20 According to AUA guidelines, following ablation, CT scan or MRI should be performed at 3, 6 months, and then annually for 5 years. 21 If the median dose of radiation exposure is 43 mSv for each multiphase renal protocol CT, and the patient undergoes a scan for initial evaluation, percutaneous CT-guided ablation, and three follow-up appointments, then they could potentially be exposed to 175–225 mSv within the span of just over a year, with the ablation representing up to 2%–25% of the total exposure based on the lowest and highest means from the current study.
Further consideration should be made to the fact that approximately one-third of patients on active surveillance progress to treatment 22 and have often received significant radiation even before treatment. Importantly, the total radiation exposure can be further limited by decreasing exposure during diagnostic and follow-up imaging, as the range of exposure can vary widely (from 6 to 90 mSv) for a multiphase CT based on institutional protocols. 10
Total radiation exposure may also be limited through the use of renal ultrasound or MRI during the ablative procedure, although both of these carry significant potential drawbacks. Ultrasound is highly operator dependent and may be compromised by the presence of bowel gas or in patients with a large BMI. In addition, acoustic shadowing on the far side of the iceball leads to image degradation and may prevent adequate visualization of the tumor margin. MRI provides excellent soft tissue resolution with multiplanar imaging capability and lacks ionizing radiation, but is seldom utilized due to the need for specialized equipment, significant cost, and increased time required for image acquisition.
Radiation exposure during the procedure, while important, is only one aspect of the patient's care and should not supersede the importance of success and complications. Kim et al. reported an overall complication rate of 9% and a major complication rate of 2% with their single-center experience with CA. 23 Hui et al. found a similar major complication rate of 3% with RFA and CA combined in their meta-analysis of 665 tumors. 24 This is comparable to our overall complication rate. Major complications included pneumothorax (1), urinary extravasation (1), hematoma/hemorrhage (3), and pain requiring readmission (1).
While the short follow-up limits discussion of oncologic effectiveness, in this series we observed an overall initial success rate (absence of contrast enhancement 6 weeks following ablation) and short-term (mean 26.7 months) success rate of 100% for biopsy-proven renal cell carcinoma at the institution with the lowest effective radiation dose, suggesting that lower radiation exposure does not come at the expense of effectiveness.
As the majority of the procedures were performed as collaborative efforts between an interventional radiologist and a urologist, we do not believe that surgeon specialty is as important as the individual practices. Moreover, in our cohort, the most junior surgeon had the lowest radiation exposure, suggesting that protocol, rather than experience, is the key driver for reducing radiation exposure during percutaneous ablation.
To determine the key determinants of radiation exposure based on protocol, cases from Institution 1 (lowest radiation exposure) were compared to Institution 2 (highest exposure). Importantly, both of these institutions utilize a single RFA probe and all ablations in this series were performed with a single deployment, thus, there should be limited heterogeneity with regard to the probe placement technique. Based on this comparison, there are three key components that we recommend to be incorporated into future protocols to limit radiation exposure during percutaneous ablation, including limiting tube current milliamperes (mAs), limiting the number of images acquired to focus on the target zone, and limiting ancillary procedures such as CT-guided renal biopsy (see Appendix).
Tube current (the number of electrons accelerated across an X-ray tube per unit time, expressed in units of mA) is the most readily adjustable scanning parameter for reducing radiation dose in CT, with a direct linear relationship between tube current and radiation dose. For every 50% decrease in tube current, there is a corresponding 50% decrease in radiation dose associated with CT. Tube current for dose reduction can be adjusted with the manual selection of a lower fixed tube current or with automatic exposure control. Low-dose protocols for lung cancer screening are typically performed at a setting of no more than 40 mA for a standard patient. 25 Within urology, Poletti et al. found that detection of renal and ureteral stones can typically be determined with a setting of 30 mA, 26 while Kemper et al. demonstrated that a low-dose CT urography (CTU) protocol using 70 mA at 120 kVp can provide acceptable image quality for the excretory phase. 19 For the nephrographic phase of a CTU, Sung et al. observed that acceptable quality could be achieved with levels as low as 150 mA. 27
In the current study, we found that suitable image quality during needle placement can be achieved with an average setting of 70 mAs at 120 kV, which can decrease the mSv of a helical scan by 7–10-fold over higher fixed bore settings. We typically recommend localizing the tumor with a larger helical scan at a higher current (150 mAs) and then lowering the current for needle placement. Following approximate needle placement, we then repeat an additional higher current scan to adequately confirm placement. Exact settings for these scans may be altered based on patient body–mass as well as ability to identify the tumor extent (particularly if endophytic). Manipulation of voltage settings may further decrease radiation exposure; however, in our experience, settings lower than 120 kV result in unacceptable image noise, which may compromise probe placement.
The largest variability between individual cases typically comes during placement of the percutaneous probe due to variability in patient and tumor characteristics. The protocol during probe placement, therefore, is the most important factor in decreasing case to case variability. Radiation exposure during this portion of the case can be limited by using a limited sequence of images centered on the target region. Generally, placement can be attempted using as few as three images, 3–5 mm thick. With this technique, each three image series adds an effective dose of 0.165 mSv compared to a spiral sequence, where the effective dose is typically closer to 1.5 mSv. Following localization, a larger helical scan can then be used to determine appropriate placement before deployment. The effect on variability using this approach can be seen clearly for Institution 1 in Figure 1.
Another cause for variability in exposure during percutaneous ablation is the use of preoperative biopsy versus biopsy at the time of the procedure. When possible, patients can undergo biopsy before the procedure using ultrasound guidance. Nevertheless, for those who require biopsy at the time of the procedure, radiation can be limited by first placing the ablation probe and then following the angle of the probe with the needle and using a similar three image acquisition as explained above. With this approach, even if the biopsy is performed at the time of the procedure, the additive radiation dose should be negligible.
Specific limitations of this study include the retrospective nature, lack of defined institutional radiation protocols prohibiting direct comparison of specific scanning protocols, absence of radiation exposure data for specific portions of the procedure (i.e., probe placement, biopsy, iceball monitoring) precluding discussion of which has the greatest contribution, and absence of long-term follow-up, limiting discussion of the relationship of radiation dose during imaging on treatment efficacy. In addition, effective radiation dose estimates are modeled measurements rather than true measurements of radiation delivered.
Conclusions
This is the first large multi-institutional study evaluating radiation exposure from CT scans during RFA and CA of SRM. Contrary to a previously published study, we did not see a difference in radiation exposure between the two treatment modalities. In addition, we have provided a mechanism for decreasing the amount of radiation delivered during these procedures. On average, the typical radiation exposure is equivalent to a multiphase abdominopelvic CT scan, with the greatest predictors of radiation exposure depending on surgeon and patient BMI. As ablative therapies of renal masses are adapted to younger and healthier adults with longer lifespans, the amount of radiation delivered during ablation is likely to pose a greater risk of secondary malignancy. Further work is required to standardize treatment protocols among institutions to significantly reduce the amount of radiation exposure required.
Footnotes
Author Disclosure Statement
No competing financial interests exist.