
Abstract
Purpose:
Longitudinal assessment of prostatic obstruction has historically been assessed with urinary peak flow rates (PFR). In this observational study, we assess the impact of prostate removal on preoperative and postoperative PFRs after robot-assisted radical prostatectomy (RARP).
Patients and Methods:
A single surgeon (TA) performed RARPs between 2002 and 2007. Men underwent routine preoperative uroflowmetric testing: 550 qualified for analysis with a sufficient voided volume (VV) of 150 mL preoperatively and at least once postoperatively. Continence and self-assessed American Urological Association (AUA) symptom and urinary quality of life (QoL) questionnaires were queried. Uroflows were analyzed preoperatively, short-term (3–15 mos), long-term (>2 y), and by age decades, lower urinary tract symptoms (LUTS) groups, and pathologic weight cohorts.
Results:
AUA and QoL scores improved from 8.1 and 1.6 at baseline to 4.4 and 1.0 at intermediate-term follow-up, P<0.01. Mean PFRs improved from a baseline 18.0 mL/s to 28.3, 30.8, and 36.5 at 3 months, 9 months, and >5 years follow- up (all P<0.001). Postvoid residual (PVR) volumes declined from 99 mL preoperatively to 24 mL at >5 years (P<0.01). Likewise, all age, LUTS, and prostate weight cohorts had significant improvements in PFR and PVR and stable voided volumes throughout the study.
Conclusion:
The natural history of prostatic obstruction for men 40 to 80 years typically reveals reduction of mean PFRs. We observed that removal of the prostate resulted on average with a near doubling of PFRs and decreased PVRs (>50%) by 3 months. After RARP, the average PFR was reset to 25–30 mL/s, and these results were seen across all age, LUTS, and prostate weight groups; the gains remained stable 2 to 4 years after operation.
Introduction
A
Studies documenting changes in uroflowmetry in patients undergoing radical prostatectomy (RP) are limited and primarily short term. 4 –6 In 2000, Stanford and coworkers 7 proposed that RP was associated with a decline in urinary function, specifically related to incontinence and a 16% stricture rate. Song and colleagues 8 examined 72 men at 36 months with urodynamic evaluation and found deterioration in bladder volume and a small increase in PFR from 17 to 19 mL/s in men undergoing nerve-sparing RP.
This article demonstrates a significant reduction in voiding domains but an increase in reservoir domains between the preoperative and 36 month evaluations. 8 We have previously reported the long-term stability of PFRs and VVs in 100 men 1 to 9 years after open RP and found no declines by age or follow-up time. 9 This study, however, lacked preoperative uroflow data, which prevented preoperative and postoperative intrasubject comparisons. Thus, there are conflicting findings reported in the literature of bladder function as men age post-RP. Also, to our knowledge, there are no studies evaluating uroflowmetry in patients undergoing robot-assisted radical prostatectomy (RARP).
The purpose of our extensive study was to quantitatively measure and compare uroflowmetry in men before and after RARP and to determine whether these results would be durable postprocedure across specific groups or all men, and to examine how age impacts these results. Although improvement after RP may be self-evident, quantitation of this benefit is not clearly established, nor is the stability over time. 4 –6,8 Men at risk for bladder obstruction may well deteriorate as they age, and the role of an ablative treatment, i.e., RARP, may benefit these men, in contrast to other prostate cancer therapies.
Patients and Methods
With Institutional Review Board approval (HS # 98-84), a prospectively maintained database of RARPs performed by a single surgeon (TA) between 2002 and 2007 was queried. The van Velthoven stitch was used in all patients. 10 Of 666 men in the series, prospective uroflowmetric testing was performed on 644 (97%) men; however, 550 (83%) qualified for analysis with a sufficient VV of 150 mL. Of the 550 men providing preoperative uroflows, those voiding >150 mL at 3 months were 303 (55%); 9 months, 181 (33%); 15 months, 148 (27%); and 2 to 4 years, 147 (27%). Men were also classified by age decades: 40–49 (n=35), 50–59 (n=185), 60–69 (n=262), and 70–80 (n=68).
All men were asked to fill out American Urological Association Symptom Score (AUASS, International Prostate Symptom Score) and Bother/QoL score 11 questionnaires, perform uroflowmetry, and undergo bladder ultrasonography to measure postvoid residual (PVR) before operation and at each follow-up visit. All subjects were asked to report to each clinic visit with a full bladder for standard electronic uroflow testing (Dantec 1000), followed by PVR measured via transabdominal ultrasonography. The Dantec device was set to a maximum reading of 51 mL/s. Men were considered inadequately filled if VVs were <150 mL at any time point and therefore were not included in the final analysis. 12 For consistency, the uroflow graphs were manually evaluated for voiding artifacts (i.e., eliminating false spikes because of straining).
Continence post-RP was defined as completely pad free, 13 and data were only available for 536 men. Patients were asked to mail in a continence card with the date they became pad free. Five men with fossa strictures met inclusion criteria and were included for completeness. All men without self-catheterization or an indwelling catheter were considered continent before the surgical procedure.
Statistical calculations were performed using SAS statistical software. 14 Comparison of uroflows was analyzed at each time point (unpaired) and directly to baseline (paired). All analyses are unpaired unless specified. The cohort was analyzed according to short-term follow-up (3–15 mos), long-term follow-up (>2 y), pathologic prostate weight groups, LUTS groups, and age groups (40–49, 50–59, 60–69, and 70–80). All box and whisker plots are represented by the following: Bar represents the interquartile range, whiskers represent the minimum and maximum, and red marks are the means.
Results
Baseline demographics for the entire cohort are listed in Table 1. The average age at baseline was 61.1 years (range 41–80). For the 56 patients with >5-year uroflow data, the mean follow-up was 6.4 years (range 4.9–10.1). One year pad-free continence was 90% (480/536). Bladder neck contracture (BNC) rate was 1.1% (6/550), and the fossa navicularis stricture rate was 1.8% (10/550).
BMI=body mass index; preop=preoperative; PSA=prostate-specific antigen; AUASS=American Urological Association Symptom Score; QoL=quality of life; GS=Gleason Score.
Figure 1 depicts the overall mean PFRs for all men at each follow-up time point. All PFRs rapidly improved from a baseline of 18.0 mL/s to 28.3 mL/s at 3 months with marginal improvement thereafter; however, all measured PFRs were significantly improved from baseline (all P≤0.001). The interval from baseline to 3 months was significant (P<0.001
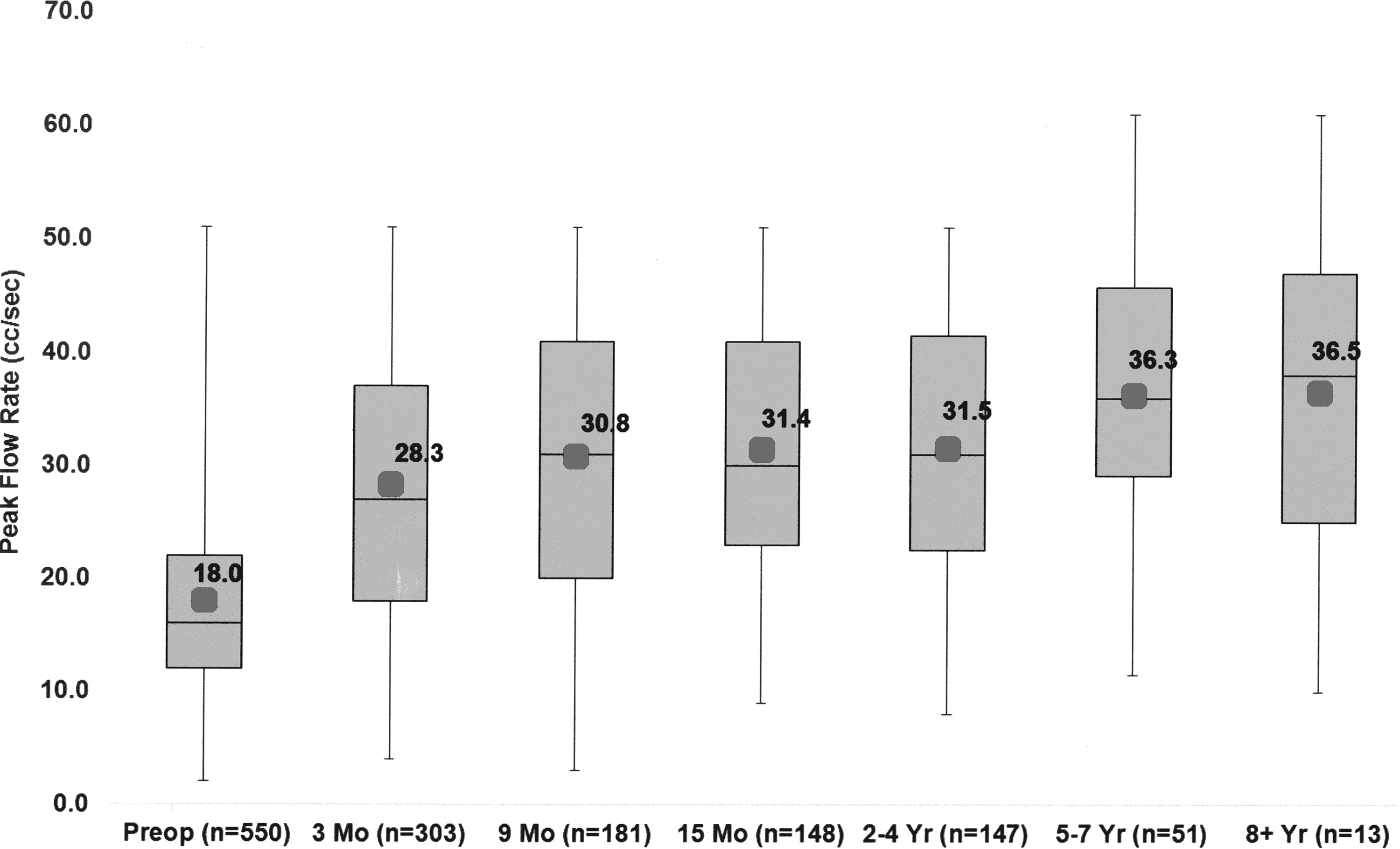
Unpaired analysis of peak flow rates at each follow-up time point. Figure bars represent the interquartile range (IQR). The whiskers represent data within 1.5 of the IQR, with the minimum and maximum of this range represented by the ends of the whiskers. The gray dots mark the means. Preop=preoperative.
PVR residual volumes for all men, on average, significantly declined from 3 months and steadily declined thereafter at 2 to 4 years postoperatively versus baseline (Table 2, all P<0.001). Voided volumes also declined ∼8% (385.6 mL to 353.9 mL) at 3 months in all men (P<0.001) and remained stable long term>4 years (all P>0.40). Overall change in the study cohort's mean preoperative and postoperative AUASS improved from 8.1 at baseline to 7.0 at 3 months and to 4.4 at >4 years (n=87). The QoL/Bother Scores mildly worsened at 3 months (1.6 to 2.0); however, they improved at 9 months to 1.4 and remained stable >4 years postoperatively at 1.0. Men with baseline moderate or severe LUTS found average 1.0 to 1.5 point QoL reductions by 9 months.
All follow-up groups were significantly improved versus baseline measurement; all P<0.01.
LUTS=lower urinary tract symptoms; AUA=American Urological Association.
Short-term results
Men with paired preoperative and 3-month uroflows drastically improved their PFRs ∼ 52%, from 18.6 to 28.3 mL/s (P<0.001). PVRs declined 53% from 99.5 to 46.5 mL, and VVs decreased 15% from 419 to 354 mL (all P<0.001). At 3 months, the percentages of men showing an increase in PFR by >200% was (12.9 %), 101%–200% (19.2 %), 51%–100% (18.2 %), and 0%–50% (28.1%). PFRs were lower than baseline in 21.5%. We did not find any differences in flow rates in the men with bladder neck reconstructions at 3 months versus those without reconstruction, P=0.76.
Long-term results
Figure 1 shows that the mean PFRs remain consistent through years 2 to 4 and do not decline even in the men with >5-year uroflow data (P=0.15). For 147 men with paired baseline and 2 to 4 year PFRs, 60% of men improved >50% over baseline PFRs and 40% improved one- to twofold. PVRs in the 147 paired men declined by 70%, from 96.1 mL to 28.8 mL, and VVs decreased 15%, from 417 to 357 mL (all P<0.001).
Prostate weight cohorts
Men were grouped by prostate weights of <40, 40–79, and 80+ grams, and at baseline were significantly different, P<0.001, Figure 2. Beginning at 3 months through 2 to 4 years, all three groups remained similar in PFRs, all P>0.33, and all groups saw improvements averaging 11–14 mL/s over baseline.
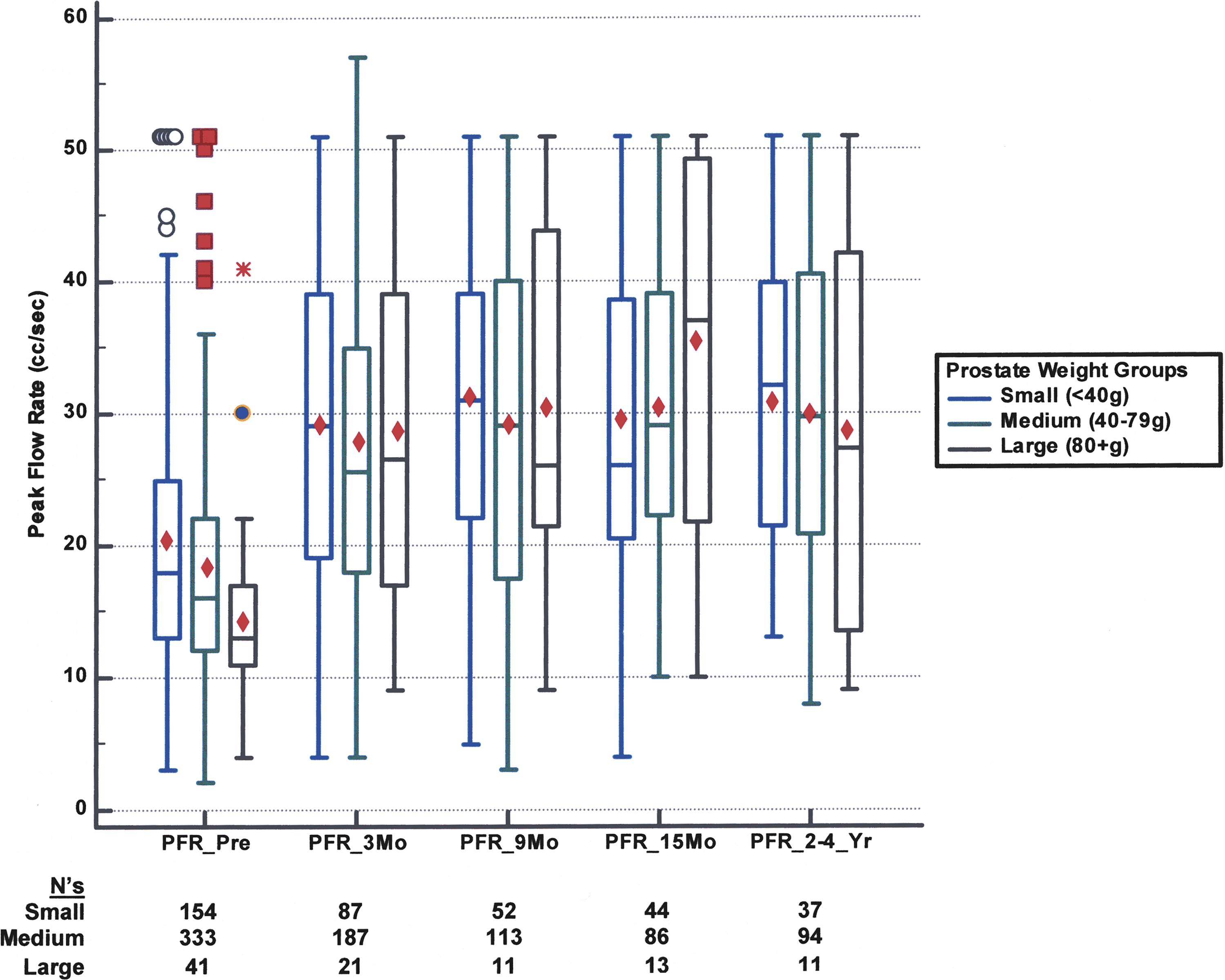
Changes in peak flow rates (PFRs) by prostate size over time compared with preoperative baseline.
Mean PVRs for prostate weight groups of <40, 40–79, and 80+ grams, were disparate at baseline and declined at 3 months and remained improved 2 to 4 years versus baseline (Table 2, all P<0.001). We note the three prostate weight groups, while significantly different at baseline (P<0.001), had no significant differences long term, P=0.70. In men with a potential for bladder outlet obstruction (BOO) over time, such as prostate size ≥80 grams, 50% have PFR ≤12, and 19% have PVR ≥300 mL at baseline; however, they find similar improvement as smaller prostates at 2 to 4 years.
LUTS cohorts
Figure 3 shows that men with moderate/severe LUTS found an average gain of 84% in PFRs at 2 to 4 years and gained half of the baseline differential between mild LUTS, but still lagged significantly below mild LUTS long term, P<0.01. Men with mild LUTS improved only 53% over baseline at 2 to 4 years. Both groups of LUTS men found immediate relief at 3 months and were clinically similar in PFRs.
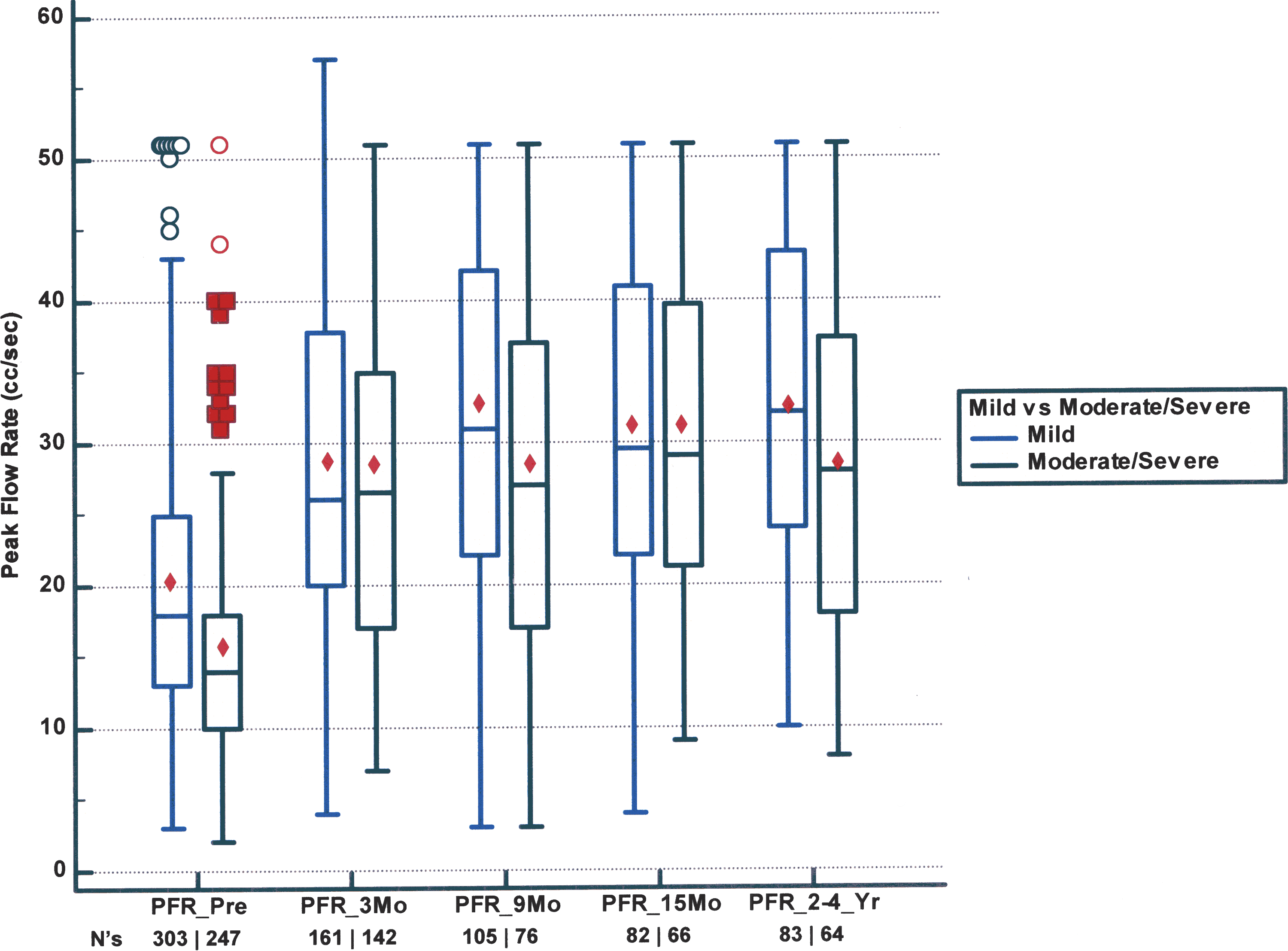
Changes in PFRs over time by groups with mild or moderate/severe lower urinary tract symptoms.
Mean PVRs for LUTS groups AUA ≤7 versus AUA ≥8 declined at 3 months and 2 to 4 years versus baseline (Table 2, all P<0.01) post-RARP. Likewise, in men with moderate/severe LUTS, 41% have baseline PFR ≤12 mL/s, and 30% have PVR ≥200 mL but their PFRs improve 84% over baseline at 2 to 4 years (Fig. 3), resulting in the residual subscore of the AUA improving on average 0.5 points or more. Similar results were found between the two LUTS groups with long-term PVRs ranging 23 mL to 31 mL.
Age cohorts
All age cohorts showed statistically significant increases in PFRs at 3 months (P<0.001) (Fig. 4). Men aged 40 to 69 had similar improvement in PFRs to >30 mL/s while in men ≥70, PFRs lagged, approaching only 25 mL/s, and remained stable over time within the age cohorts. Although men ≥70 years improved significantly in their PFR at 3 months (P=0.001), they did not fully reach the mean PFR of men <70 (P=0.05) (Fig. 4). Across each age cohort, average PVRs declined ∼50% at 3 months and steadily declined even >5 years postoperatively (P<0.001). Preoperative and postoperative VVs were similar in men 40 to 69 (417.3 mL to 413.7 mL, P>0.05), but mildly decreased by 12% in men ≥70 (334.4 mL to 295.9 mL).
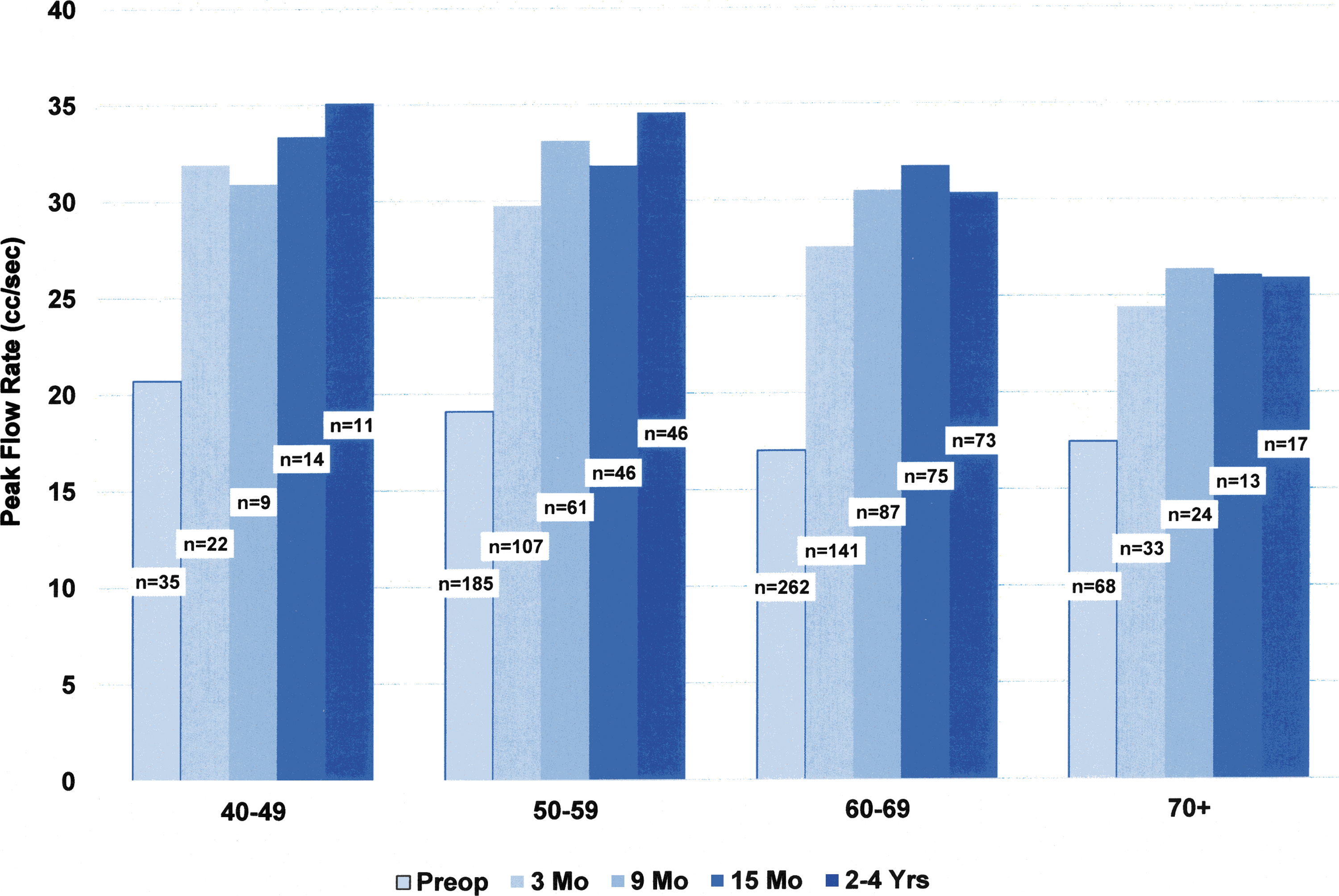
Change in PFRs for men by age decades after robot-assisted radical prostatectomy.
Discussion
An important finding of this study is that most men see dynamic improvement in PFRs beginning at 3 months to 28.3 mL/s, which increases significantly short term. More than 75% of men demonstrate immediate improvement, 34% of whom experience a one- to twofold increase in PFR. Clinically significant reductions in PVRs also occur by 3 months.
Our current study confirms improved PFR after RARP, as initially reported in open RPs. 4,5,15 Our findings are similar to those of Masters and Rice 6 who reported an average of 11.6 mL/s increase in PFRs from baseline in 108 men and PFRs rising to 24 mL/s at 20 months in 30 men. 6 Our data differs from Song and associates 8 who reported a small post-RP increase in PFR of 16.5 mL/s at baseline to 18.5 at 3 years. This difference in PFRs between our study and that of Song and associates 8 is because of how PFR was measured. The voiding phase during urodynamics is usually performed through a catheter, which can cause underestimation of PFR, depending on the size of catheter used. 16 –18
A second finding of this study is that PFRs remain stable over time when compared either by baseline PFR or age cohorts, because 82% improve over baseline and 40% display one- to twofold increases in PFR. These gains remain durable 4 years postoperatively. These findings are contrary to the natural progression of BPH and decreased PFRs that occur as men age. 1,2,19 –22 PVRs declined at 3 months and continued to decrease with durable long-term progress because, on average, men return to 80% to 90% of their preoperative bladder volumes after RARP, a trend also seen in Asian population results. 8 There is a risk of prostatic regrowth after bladder outlet procedures such as TURP, resulting in decreased PFRs over time 3 and possible need for a repeated procedure, which is not seen after RARP.
The third finding of this study is that age is not a barrier to improvement. A population-based study by Roberts and colleagues 2 at the Mayo Clinic of normal men of 10-year cohorts for ages 40–49, 50–59, 60–69, and ≥70 demonstrated declining median PFRs of 21.2, 21.3, 16.3, and 14.2 mL/s, respectively by age decades, as well as percentage PFR decreases per year of −1.1, −2.7, −2.3, and −6.2. Figure 4 shows similar baseline PFRs in our age distributed population; however, post-RARP PFRs increased by 50% to 75% across all age cohorts and does not show the age-related decline that was reported in the Olmsted population. 1,2
Our current study not only confirms the long-term uroflowmetry stability reported in our previous study of men undergoing open RP 9 but also demonstrates significant improvement only 3 months after surgery. In addition, we have shown that these findings are durable 4 years after RARP. It appears that across the age cohorts, the clock is reset before the onset of BPH generating mean PFRs of >30 mL/s for men 40 to 69 and >25 mL/s in men ≥70 years.
Surgical procedures have associated patient risks; consequently, great care is given to minimize harm. RP has a secondary benefit by extirpating the prostate gland with its associated BPH component that restricts the urethra, limiting urinary flow. A further observation of this study is that men generally return to pre-BPH flow rates regardless of baseline age, prostate weight, or AUA Symptom Scores, demonstrating no significant differences long term, except in men with baseline moderate/severe LUTS having diminished levels versus mild LUTS.
Essentially the obstructive increases in prostate weight do not appear to be a barrier to return preonset BPH uroflowmetry; however, patients should be advised that long-term differences between mild to moderate/severe LUTS may indicate that storage symptoms may not fully resolve after RARP in the latter even at long term. An important secondary finding is that PVR is significantly reduced to <50 mL across groups, and patients at risk for long-term BOO will find relief with RARP versus nonsurgical prostate cancer treatments.
RARP and open RP improve uroflowmetry in men undergoing the surgical procedure, a benefit not demonstrated in alternative treatments such as active surveillance or radiation therapy, 23 where progression over time is likely. Consideration should be given to preoperative urinary function when counseling men about treatment options for prostate cancer, especially when definitive treatment is indicated. Intuitively, urologists expect some uroflowmetric relief, but customarily this is not measured by standard postoperative instruments and rarely included in the discussion of treatment options for prostate cancer. Removing the prostate impacts a direct and measurable benefit to AUASS and uroflowmetry that cannot be quantified by outcome questionnaires—e.g., Bother Score and Expanded Prostate Cancer Index Composite—especially when compared with other treatments. 6,.24,25
Uroflowmetry is a simple, noninvasive, and clinically useful test to infer the presence of BOO—e.g., stricture or BNC—for additional workup, especially when combined with PVR and PFR. A recent meta-analysis showed that PVRs measured by bladder scan correlated highly with PVRs measured by catheterization. 26 Uroflowmetry has important limitations that warrant caution when interpreting results. While uroflowmetry detects patients with low flow rates, it cannot differentiate impaired detrusor contraction from BOO. 27,28 Patients with high-flow obstruction will be missed by uroflow alone. More invasive, pressure-flow studies (urodynamics) are needed for such evaluations, but were too expensive and time consuming to be performed on such a large population with little symptomology. 29 Uroflowmetry does not detect changes in detrusor function after RARP.
A limitation of the current study is that men performed only one uroflow per clinic visit, where multiple studies may be more accurate. Age cohort studies such as this are less powerful than repeated measure designs; however, to have men enthusiastically repeat uroflows, with full bladder volumes >150 ml without fail consistently at all follow up-visits over a 10-year period is very challenging. Also, our institution is a referral-based center of many men who reside outside the local area, thus limiting follow-up, especially in that all uroflowmetry was performed on site for consistency. Men with VVs <150 mL were excluded from this study, but there was no difference in baseline characteristics between the study cohort and excluded men. These limitations should not overly distract from the usefulness that RARP has on improvement in PFRs.
Conclusion
The natural history of prostatic obstruction for men 40 to 80 years typically reveals reduction of mean PFRs. We observed that removal of the prostate resulted on average with a near doubling of PFRs and decreased PVRs (>50%) by 3 months postoperatively. In men with longer follow-up, mean PFRs remained stable or increased. These results were seen across all age groups, LUTS groups, and prostate weight groups, and the gains remained stable 2 to 4 years after operation.
Footnotes
Acknowledgments
We thank Andrea Cabarras for her diligence in data collection in this study, and Lisa Guzman for the many years of clinical measurement of uroflow/PVR in this study.
Author Disclosure Statement
No competing financial interests exist.