
Abstract
Introduction:
Ureteroscopic stone extraction devices are effective tools in the management of urolithiasis, but on occasion, their improper use can cause injury to the ureter. Avulsion and perforation of the ureter as a result of excessive forces on the extraction device are some of the more serious complications of this treatment.
Materials and Methods:
In this article, avulsion and perforation forces were measured by two different test setups. Eleven clinicians were asked to apply three ranges of forces (safe, cautious, and dangerous).
Results:
The output force measurements were recorded and plotted for further analysis. The maximal average perforation forces were 7.13±2.36 N in the benchtop tests and 7.07±2.20 N in the ex-vivo porcine tests (P=0.54). The maximal average avulsion forces were measured to be 10.14±2.01 N in the benchtop tests. Although the average forces were similar in the proximal and distal parts of the ureter (P=0.27), higher values were recorded for the distal part. The operative time was noted to be significantly different in the safe and cautious force regions (P=0.006). The average forces were higher in the benchtop tests compared with the porcine ureter tests. The extraction forces were measured and were noted to be significantly different for attending physicians and residents. The results suggest the need for force feedback training for residents.
Conclusion:
The findings can be used to design a “smart device” that can provide visual force feedback to clinicians while they are operating, leading to improved patient outcome.
Introduction
T
Ureteroscopy is a minimally invasive and effective procedure; however, it still has the potential to cause injury. Complications during basketing might be minor (necessitating minimal intervention) or major (needing open or laparoscopic intervention). 4 –6 The rates of complications during stone manipulation are reported to be in a range of 0.1% to 10.64%. 7,8 Perforation and avulsion of the ureter are the most dreaded complications of ureteroscopy but are fortunately uncommon. The first cases of ureteral avulsion were reported by Hart 9 and Hodge, 10 and occurred as a result of excessive force and difficulty in manipulation of a ureteral stone with a kidney basket. 11 Avulsion is usually recognized immediately, because a segment of ureter is often removed with the stone that is trapped inside the basket. 12,13
The attempt to remove a large stone with the use of excessive force in a ureter with stricture (narrowing of the ureter) is a significant risk factor for ureteral avulsion and perforation. 14 In addition, because the proximal ureter has less muscle support, basketing a stone in this part of the ureter increases the risk of avulsion. 15
To avoid such serious complications, smart devices could potentially play a significant role in preventing these problems. 16,17 One of the most important elements of smart medical devices is the principle of feedback. 18 Such devices are designed in a way to support a flow of communication between the patient's body, the tool, and the surgeon. Because of these factors, force feedback has become an important focus in the design of new medical devices. 19 –21 Perforation and avulsion forces of a porcine ureter have been measured and reported in the literature. 22 In this article, the extraction and injury forces are estimated by 11 clinicians in two different tests. In both test setups, the results were measured using a miniature load cell and recorded by an automated data acquisition system.
Materials and Methods
There are different ways to measure forces, and load cells were selected as the best way for this application. 18 In this article, two tests were conducted: (1) Benchtop test and (2) an ex-vivo porcine test. Eleven clinicians participated in the test—two experienced attending surgeons and nine postgraduate urology residents (two fifth year, one fourth year, two third year, two second year, and two first year postgraduate year [PGY] residents). The P values were calculated with the Student t test statistical method (P values <0.05 were considered statistically significant).
Load cell force measurement test
A miniature, low force load cell (OMEGA® LCL-010 Series thin beam) with maximum load tolerance of 2 kg was used for the force measurements. The calibration of the load cell was performed by fixing it on an optic table and suspending various calibrated weights from it. Because of the low output voltage range of the sensor, an instrumentation amplifier was used to increase this range. The amplified voltage was fed to the DATAQ data acquisition system DI-710 (Fig. 1). The output voltage was displayed and recorded on a WINDAQ waveform browser for further analysis.
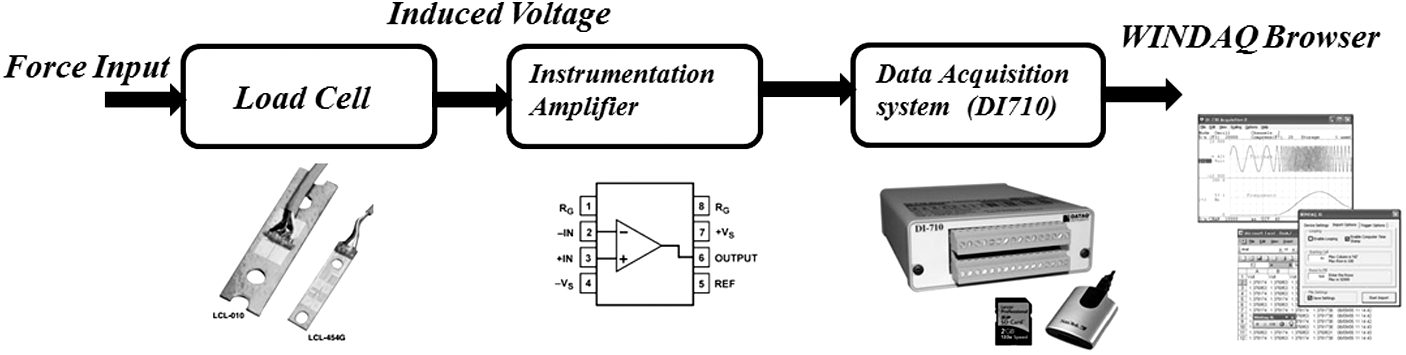
Block diagram schematic of forces measured by load cell.
The benchtop test setup is shown in Figure 2. In this setup, a basket handle was attached to the sensor to facilitate the test. Clinicians were asked to pull the handle downward to the extent that they felt it was absolutely safe for the ureter and then release it back. They were then asked to pull the handle to the extent that they felt they would have gone beyond their safety zone (perforation) and again release the handle. Finally, they were asked to pull the handle to the extent that they definitely felt they would have caused avulsion and then release the handle. Each of the three tests was run three times for distal and proximal parts of the ureter. The clinicians did not have a visual output (display or screen) for monitoring their applied forces.
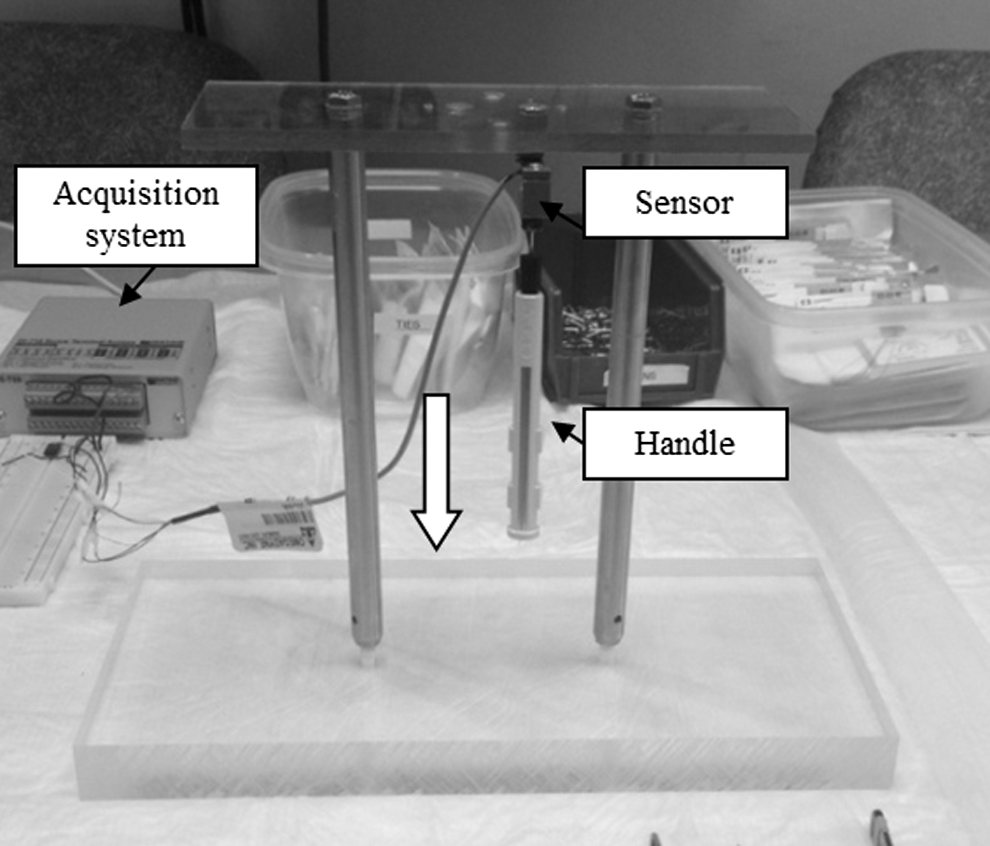
Benchtop test of load cell force measurement.
Ex-vivo force measurement test
An ex-vivo model was prepared using a porcine kidney with an intact ureter. This model simulated a human kidney and ureter in an operating room. Small stones (spherical) sizes 3.0 and 4.0 mm were used to simulate ureteral stones. A stricture was made on the porcine ureters and 1.5F tipless nitinol stainless steel baskets were advanced proximal to the stricture inside the ureter (Fig. 3). The external end of the basket was attached to the load cell (OMEGA® LCL-010 Series thin beam), and the load cell was fixed on a small platform (Fig. 3).

Preparation of the stricture in the ex-vivo porcine model (on right); kidney basket attachment to the withdrawal system (on left).
In the next step, the clinicians were asked to grasp the stone using the basket with the aid of a visual ureteroscope display, hold the handle securely, and then pull the withdrawal system (as a retraction procedure) to the extent they felt it was absolutely safe for the ureter, and then release the platform. They were then asked to pull the withdrawal system back to the extent that they thought they had gone beyond their safety zone (perforation) and again release the handle. Each test was run three times for the distal and proximal parts of the ureter, and the output was recorded for further analysis.
Results
The load cell OMEGA® LCL was calibrated, and the calibration curve was plotted and used for further analysis. Benchtop tests and ex-vivo porcine tests were run, and the results were analyzed in the WINDAQ and MATLAB commercial software platforms.
Bench top load cell test results
Figure 4 shows the output force of clinician 3 (one of the two attending clinicians with more than 25 years of experience) when operating in the proximal part of the ureter. Three runs were conducted, and each run was assigned a color. The safe, cautious, and, dangerous regions are shown in Figure 4 with arrows. The maximal average forces (MAF) for each clinician in the proximal and the distal ureter were calculated and plotted. The total MAF of safe forces was 4.59±1.25 Newton (N) in the distal and 4.19±1.07 N in the proximal parts of the ureter (P=0.27>0.05). MAF value in the cautious region were measured to be 7.64±2.49 N in the distal, and 6.63±2.23 N in the proximal (P=0.18) parts of the ureter. Finally, the MAF in the dangerous region was 10.47±2.49 N in the distal and 9.50±1.35 N in the proximal part of the ureter (P=0.16).

Output force of load cell (clinician 3) in the proximal ureter (benchtop test).
The results showed that for each clinician, the applied forces in the distal ureter were higher than in the proximal part of the ureter. By observing the results of each clinician in the green (safe), yellow (cautious), and red (dangerous) region in Figure 5, one can see less variation in the results for the control group (two attending surgeons). The variation increases when one gets to the less experienced clinicians. It is also observed that some of the residents applied either much higher or much lower forces during extraction.
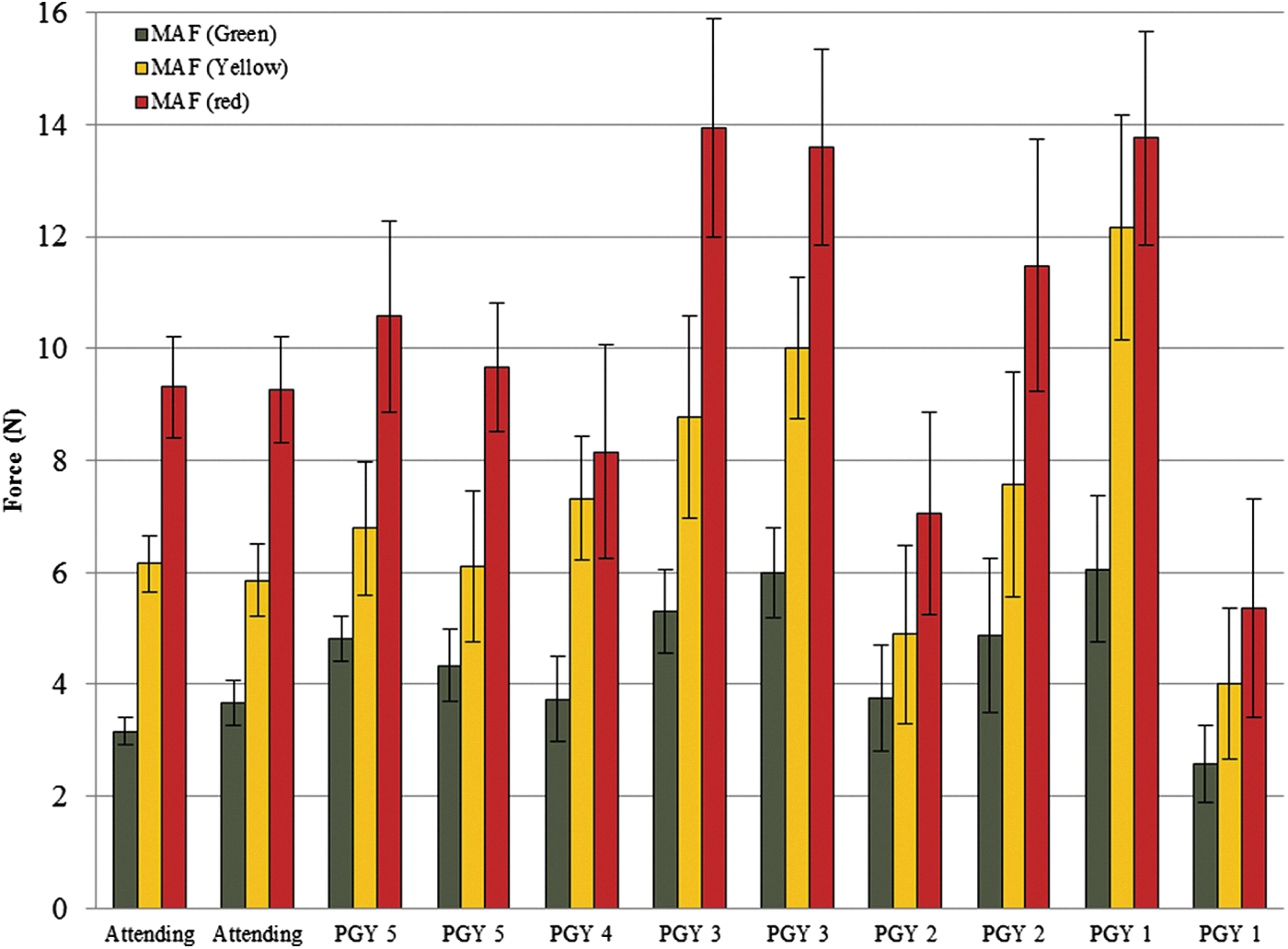
Average of proximal and distal maximal average forces (MAFs) of each clinician in the benchtop test for three regions. Vertical bars present standard deviation based on sample. PGY=postgraduate year.
Based on these finding, three groups were defined for the clinicians: The control group (G1) that included the attending physicians, the second group (G2) that included the fifth and fourth year (PGY4, PGY5) residents, and G3 that included the PGY1, PGY2, and, PGY3 residents. The standard deviation of the applied forces in these three groups was calculated. The variation in all three tests was significantly higher in G3 (P=0.02), and it decreased when it got to G1. The average forces of perforation and avulsion, in the control group, were measured to be 6.00±0.62 N and 9.28±0.83 N, respectively.
Ex-vivo porcine force test results
In this test setup, the applied force in the safe and cautious regions was measured, and the output of the load cell was plotted and analyzed. Figure 6 illustrates the three runs of a clinician in the proximal part of the ureter. The safe and cautious regions are shown with arrows in the figure.

Output force of clinician 3 in the proximal ureter (ex-vivo test).
The parameters that were calculated and analyzed in this test are given below: • MAF • Maximum time (Tm): The time from 5% of the maximum force to the peak of the curve. This parameter indicates the operative time. • Rise time (Tr): The time to reach 65% of the maximum forces. This parameter describes the speed of operation. • Work: The amount of work (or effort) by the clinician given by the area under each curve.
MAF results
The MAF in the green region were 4.88±1.67 N in the distal and 3.80±1.25 N in the proximal parts of the ureter. There was no significant difference (P=0.08) between these two values; however, the applied forces in the distal were higher than in the proximal parts. The MAF in the yellow region were 7.34±2.55 N and 6.81±1.86 N in the distal and proximal parts of the ureter, respectively (P=0.28). The difference between the MAF values in the proximal and the distal parts was higher in PGY1 and PGY2 groups. Figure 7 illustrates the average of the proximal and distal values of the clinicians in the green and yellow regions. The green bars show the MAF values in the safe region, and the yellow bars are the MAFs measured in the cautious region.

MAF values of each clinician in safe and cautious regions in ex-vivo porcine test.
The groupings were mentioned before, and this further validated the groupings. The variation between the applied forces in each group is plotted in Figure 8. As shown here, the variation in G3 is significantly higher than the control group. The variation in the yellow region in G3 was higher in the yellow region than in the green region.

Standard deviation of groups for green and yellow regions in the ex-vivo test.
Tm and Tr results
The average values of Tm and Tr are presented in Table.1. The Tm values in the distal and proximal parts of the ureter were not significantly different in the green region (P=0.09>0.05); however, these values were significantly different in the yellow region (P=0.01). The Tm value was noted to be significantly higher in the yellow region than in the green region (P=0.006). These results indicate that the clinicians spend more time in the proximal part of the ureter than in distal part of the ureter. Tm values had high variation in G3 (4.50±1.47 s) and G2 (4.22±0.76 s) in comparison with the control group (3.85±0.46 s). There was not a significant difference between the control and G2 (P=0.07); however, the Tm values in G3 were significantly different from the control group (P=0.01).
Significant at P value <0.05 by Student t test.
SD=standard deviation.
The Tr values in the distal and proximal ureter were not significantly different in the green region (P=0.07>0.05); however, these values were found to be significantly different in the yellow region (P=0.03). Although the Tr values were higher in the yellow region (1.85±0.50 s) than in the green region (1.70±0.28 s), they were not significantly different (P=0.4).
Work results
The area under the curves of each test was calculated and analyzed. The average work performed by clinicians in the green region (11.21±4.12J) was significantly different from the yellow region (13.73±4.61J, P=0.02). The average work was higher in the proximal part than in the distal part in both the green and the yellow regions. It was significantly different in the yellow region from the distal (12.47±4.88 J) to the proximal part of the ureter (15.00±4.60 J, P=0.004). There was a constant variation in the work performed by the control group; however, this value increased in G2 and even more so for the G3 (these groups had higher operative times and MAF values).
Force measurement results in the porcine test vs benchtop test
The MAF values in the yellow region for the benchtop test and the ex-vivo porcine test are shown in Figure 9. The results are similar (P=0.54) and consistent with each other; however, the MAF values in the porcine test are lower than the values in the benchtop load cell force test. The forces are compared in the green region, and they are not significantly different (P=0.48).
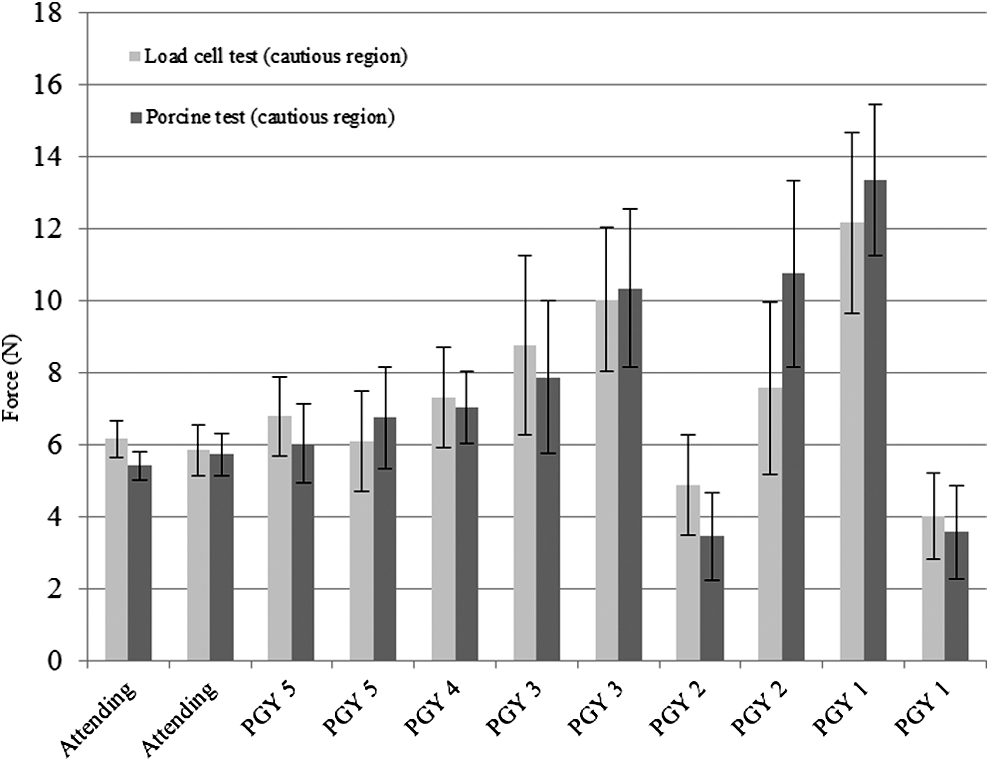
MAF values of each clinician in cautious region for both tests setups.
Discussion
Ureteroscopy and basket extraction is the most common method for removing ureteral stones, 23,24 and some complications are ureteral perforation, mucosal injury, ureteral rupture, and ureteral avulsion. 25 These complications may lead to increased operating room time, cost, and in some cases may have severe and lasting consequences. Ureteroscopic training devices help develop endourologic skills; however, they lack force feedback on how much force can be safe to avoid ureteral complications. This is one of the first studies to address the safe, cautious, and dangerous extraction forces in proximal and distal parts of the ureter.
A study found in the literature measured the perforation forces (6.98±1.14 N) and avulsion (9.84±1.86 N) in a pig ureter. 22 The results reported in this article are consistent with the forces reported in the literature. The forces needed to avulse the human ureter, however, would be less than in a porcine ureter. In this study, the clinicians were asked to run the tests and apply forces as much as they apply on a human ureter. The maximal average perforation forces were 7.13±2.36 N in the benchtop tests and 7.07±2.20 N in the porcine test model (P=0.54). The maximal average avulsion forces were measured to be 9.98±2.01 N in the benchtop tests and, as mentioned, are in good agreement with Pedro and colleagues.22
It is noted that in both tests, the differences in proximal and distal MAF values were not significant, but in all cases, the proximal forces were lower than the distal forces, and this may imply that the ureter is more vulnerable in its proximal area than in its distal area. In a recent study, the literature on ureteral avulsion was reviewed, and it was shown that most of the injuries were taking place in the proximal parts of the ureter. 8 The high variation between the applied forces in G3 and G2 compared with the control group G1 indicates that there may be an opportunity to create specialized training programs for residents using devices with force feedback. The measured MAF values were either lower or higher than the control group. The forces in the porcine test with visual feedback (the ureteroscope display) were less than the benchtop tests, which indicates the role of visual display in the extraction of the stone.
In addition, the operative time was noted to be higher in the proximal tests than in the distal test, and also this parameter was noted to be higher in the yellow region when compared with the green region. This result indicates that the clinicians may be acting more cautiously in the more sensitive parts of the ureter (proximal). The speed of extraction was calculated, and the results show that the clinicians spend more time (smaller) in getting to their maximum force values in the yellow region and especially in the proximal part of the ureter. There was a high variation in the time parameters of G3 and G2 in comparison with the control group (G1).
The main finding in this study is the comparison between the measured parameters in the control group and the second (G2) and third groups (G3), which indicates the need for specialized training of the residents on extraction forces. These results would help design a training device (or system) to let the urologist know when the applied forces are in the cautious region. Improved training of the urology residents on the extraction forces can only lead to improved patient safety as the residents become practicing clinicians.
It should be noted that the tests were run with the assumption of a healthy ureter. Ureteral abnormalities such as inflammation, urinary tract infections, stone configuration, and basket type can change the measured parameters.
Conclusion
A crucial contributing factor to a successful surgical procedure is sensory feedback. Complications of ureteroscopy usually involve the attempt to remove a large stone with extra forces using a kidney basket. 14 –17 To reduce these complications, urologists routinely manage the forces applied during stone extraction. This study quantifies the extraction forces and specifically addresses the need for force extraction awareness and developing aids for training. The measured force values can be used to design “smart devices” that can not only help during the training phase but can also aid in reducing the complication rates, leading to improved patient outcomes.
Footnotes
Author Disclosure Statement
No competing financial interests exist.