
Abstract
Objectives:
To establish patterns of anatomic changes relevant to the kidney and colon during positional change between the supine and prone positions as noted on CT scans performed during percutaneous cryoablation for renal cortical neoplasms (RCN).
Methods:
Nineteen patients undergoing percutaneous cryoablation for RCN with abdominal CT scan in both the supine and prone positions were included in the study. We documented the anterior/posterior, medial/lateral, and cranial/caudal anatomic changes of the kidney, kidney rotation, and the proportion of the kidney whose access was limited by the liver, spleen, and lung. We also calculated the length of the percutaneous access tract and the distance between the colon and kidney in hilar position as well as the anterior/posterior location of the colon relative to the kidney.
Results:
In the prone position, the kidney lies significantly more anteriorly on both sides: 4.7 cm vs 4.3 cm (L) and 4.4 cm vs 4.1 cm (R) (p = 0.02 and p = 0.03, respectively). On prone CT images, both kidneys are more cranial when compared with the supine position: 80.4 mm vs 60.8 mm (L) and 87.2 mm vs 57.4 mm (R) (p = 0.002 and p < 0.001, respectively). The skin to tumor distance is significantly shorter in the prone position (p < 0.0001 [L], p = 0.005 [R]). The colon lies closer to the hilum of the kidney and is more posteriorly located in the prone position: 1.21 cm vs 1.04 cm (L) and 0.80 cm vs 0.70 cm (R) (p = 0.005 and p = 0.005, respectively). In the prone position, the lung covers a significantly larger proportion of the right kidney (27.3 mm vs 6.05 mm, p = 0.0001).
Conclusions:
We documented clinically significant anatomic alterations between supine and prone CT imaging. The changes associated with the prone position modify percutaneous access, particularly for right upper pole tumors. Prone imaging before surgery may be helpful in selected cases.
Introduction
T
Technical improvements in cryoablation and imaging technologies and promising intermediate-term outcome data have broadened the indication of renal cryoablation to younger well-informed patients with a desire for minimally invasive treatment. 3 As noted with the transition from open surgery to less invasive approaches, such as the laparoscopic and robotic techniques, renal cryoablation has been transitioning to percutaneous access to optimize the minimally invasive nature of the technique.
During percutaneous renal cryoablation, postural alterations or injection of saline are used to hydrodissect vulnerable structures, such as the bowel, to avoid injury. Occasionally, when patients are placed in the prone position, we have noted anatomic alterations that make safe percutaneous renal cryoablation difficult or impossible. The last-minute discovery that the tumor is not amenable to a percutaneous approach is a function of most imaging being performed in the supine position. We noted that certain anthropometric alterations occur when comparing patients in the supine and prone positions. These anatomic changes are highly salient with regard to the feasibility and safety of percutaneous ablation for the given patient and have not been previously evaluated in this population. As such, we sought to investigate the anatomic changes in the position of the kidneys and surrounding anatomic structures between supine and prone CT scans.
Materials and Methods
Internal review board approval for data collection was obtained. A total of 60 patients presented with renal masses for percutaneous cryoablation between January 2008 and November 2011. Of the 60 patients, 19 patients were identified in whom films were available and who underwent abdominal CT scans in the supine (preoperative) and prone (intraoperative) positions without bolsters applied during the procedure. As part of our routine, all scans were obtained at the end of inspiration. Retrospective measurements were performed on axial CT slices with adjustment to the tilt on the OsiriX MD, a 64-bit dicom viewer (Pixmeo, Geneva, Switzerland), by a single urologist (A.L.). In addition, we evaluated tumor characteristics as well as peri- and intraoperative complications.
The anterior/posterior position of the kidney was defined as the distance of the anterior edge of kidney to the posterior edge of the vertebral body at the level of the renal hilum. The medial/lateral position of the kidney was evaluated by measuring the distance from the medial border of kidney in the hilar position to the midsagittal anterior–posterior line through the vertebral body (Fig. 1). We determined the cranial/caudal position of the kidney on axial CT slices. We established the distance between the tip of the 12th rib (fixed site) and the most superior component of the kidney by multiplying CT slice thickness by the number of slices separating these two sites.
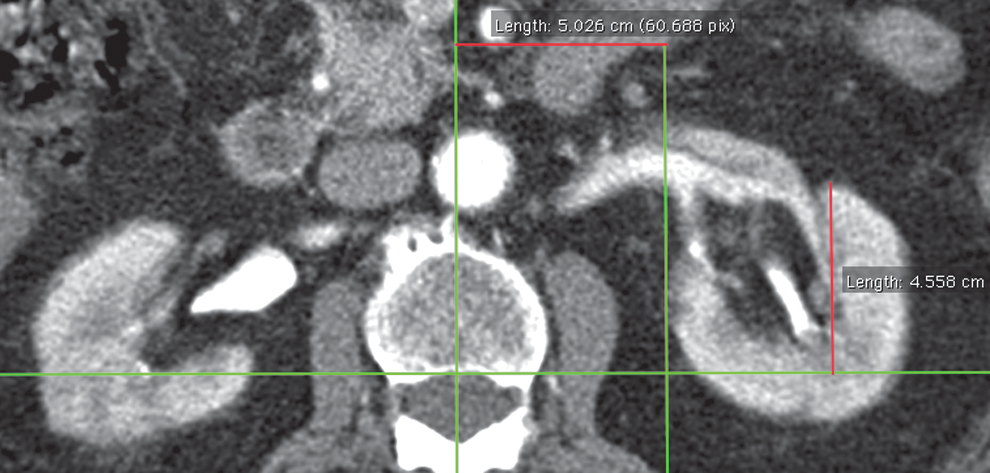
Measurement of anterior/posterior and medial/lateral positions of the kidney.
The kidney angle was defined as the angle between the midsagittal anterior–posterior line through the vertebral body and an imaginary line drawn through the medial and lateral edges of the renal operculum (Fig. 2). Further measurements included the amount of kidney covered by the liver/spleen/lung—after determination of the lowermost portion of the liver/spleen/lung on the axial CT slice, we scrolled the CT slices up and measured the distance to the upper pole of the kidney by counting the number of CT slices and calculated the distance by multiplying the number of slices with the slice thickness.

Measurement of kidney angle.
The cryoablation tract length was defined as the shortest distance between the skin edge and the midtumor medial to the tip of the 12th rib. This entry point is normally used for percutaneous access. The quantity of perirenal fat was measured as the perpendicular distance between the posterior surface of the kidney and the internal margin of the iliopsoas muscle at the level of the renal hilum.
The distance of right (hepatic) and left (splenic) colonic flexure to the posterior part of the vertebral body was measured at the level of the renal hilum. At this position, we also evaluated the shortest distance between the colon and the most medial positioned part of the kidney (Fig. 3).

Measurement of colon position.
Statistical analysis
Statistical analysis was conducted using the SPSS version 20 (IBM, Chicago, IL). A paired Wilcoxon rank test was used with p-values <0.05 considered statistically significant.
Results
Nineteen patients (13 men and 6 women), with a mean age of 72.7 years, underwent abdominal CT scans in both the prone and supine positions without bolsters. Both kidneys (left and right sides) are more anteriorly located in the prone position: 4.72 cm vs 4.29 cm for the left side and 4.41 cm vs 4.06 cm for the right side (p = 0.02 and p = 0.03, respectively). There was no change in the medial/lateral position between the prone and the supine scans (4.00 cm vs 4.12 cm [left kidney, p = 0.122] and 4.24 cm vs 4.15 cm [right kidney, p = 0.809]). We noted that bilateral kidneys had a significantly more cranial position on prone imaging when compared with the supine images: 80.4 mm vs 60.8 mm for the left kidney and 87.2 mm vs 57.4 mm for the right kidney (p = 0.002 and p < 0.001, respectively) (Table 1).
There was no significant change in the angle of the kidney between the prone and supine positions (L: 41.1° vs 43.4°, p = 0.573; R: 42.9° vs 44.7°, p = 0.122, respectively).
We established the skin edge to tumor distance as the percutaneous puncture tract length. This distance was significantly shorter on prone CT imaging: 6.47 cm vs 7.84 cm (right side) (p < 0.0001) and 6.04 cm vs 6.81 cm (left side) (p = 0.005).
On the right side, the lung covers a significant larger amount of kidney in the prone position (27.3 mm vs 6.05 mm, p = 0.0001). However, on the left side, there was no significant change in the amount of lung covering the kidney (14.2 mm vs 8.05 mm, p = 0.253). There was no significant difference in the amount of kidney covered by the spleen or liver on anatomic change from supine to prone positioning (39.2 mm vs 35.3 mm [prone vs supine, left kidney] and 79.4 mm vs 75.3 mm [prone vs supine, right kidney]).
We documented that in the prone position, the colon moves significantly closer to the renal hilum: 1.02 cm vs 1.32 cm for the left side and 0.81 cm vs 1.45 cm for the right side (p = 0.04 and p = 0.33, respectively). In the prone position, the colon is also more posteriorly located: 1.21 cm vs 1.04 cm (left kidney) and 0.80 cm vs 0.70 cm (right kidney) (p = 0.005 and p = 0.005, respectively). Regarding the amount of perirenal fat, there was no significant difference between prone and supine images (1.04 cm vs 1.21 cm [L] and 0.8 cm vs 0.7 cm [R], p = 0.064 and p = 0.103, respectively).
Tumor characteristics of all 19 patients are shown in Table 2. We noted a total of 8 minor intraoperative and perioperative complications in 7/19 (36.8%) patients. Five patients experienced small, asymptomatic, intraoperative perirenal hematoma (26.3%), which was only noted by imaging during the procedures. One patient developed hematuria (5.2%), and one patient experienced a small asymptomatic pneumothorax and perirenal hematoma (5.2%). Only the hematuria patient required intervention, which included bladder irrigation and observation for 23 hours.
Discussion
To our knowledge, there are no published reports of anthropometric renal alterations between the supine and prone positions, which focus on the impact of percutaneous ablation for RCN. Although CT scans for diagnostic reasons are most typically performed in a supine position, percutaneous ablation procedures are commonly performed in the prone position. In this retrospective study, several clinically relevant anthropometric alterations were associated with the prone position. The purpose of this study was to describe the anatomic differences between prone and supine CT scans and the clinical impact of percutaneous ablation procedures.
In the current study, the percutaneous cryoablation tract length is statistically significantly shorter in the prone compared with the supine position on both sides (6.47 cm vs 7.84 cm [right side] and 6.04 cm vs 6.81 cm [left side]). One potential explanation for the difference in the tract length might be the difference in the body thickness between the prone and supine positions (22.6 cm vs 25.27 cm, p = 0.001). The posterior body wall is less deformable compared with the anterior body wall because of the vertebral column and the ribs. This may lead to an increase in body compression of organs in the prone position, with the kidney then forced posteriorly and consequently a shorter skin to tumor distance. Surprisingly, the kidneys on both sides are more anteriorly located in the prone position (4.72 cm vs 4.29 cm for the left side and 4.41 cm vs 4.06 cm for the right side). Similar findings were presented by Duty and coworkers in 20 patients with a CT scan in the prone and supine positions, in which both kidneys were farther away from the anterior border of the vertebral column. 4 A further study by Azhar and colleagues showed identical results in 16 percutaneous nephrolitholapaxy (PCNL) patients; again, the prone position was associated with a shorter skin to target (stone) distance. 5 Our findings may be clinically significant in obese patients in whom biopsy and ablation technologies sometimes may not be long enough to access the target pathology during supine measurements.
One of the most clinically significant findings was a bilateral cranial movement of the kidneys in the prone position. Honey and colleagues evaluated anatomic alterations between the supine, prone, and prone-flexed positions. The authors demonstrated significant (1.5 cm) superior movement of the kidney in the prone-flexed position compared with the standard prone position. 6 This finding could be helpful for upper pole tumors, and table position should be recognized as highly relevant.
One of the most salient findings of the current article is that the colon can be located significantly more posteriorly and in closer proximity to the kidney in the prone position. Changes in the position of the colon are clinically important during percutaneous ablation procedures as the colon may be at increased risk for ablative energy injury with shorter distances from the target pathology. These findings are consistent with those of Cormio and colleagues who reported a more anteromedially located colon in the supine position. 7 The prone position is also associated with an increasingly posterior location of the colon. Hopper and colleagues first reported this anatomic alteration when they compared images from prone and supine CT scans. The study group showed a higher incidence of a retrorenally located colon in the prone (10%) position compared with supine CT images (1.9%). 8 An additional study by Tuttle and colleagues showed that the risk of organ injury was increased for a lower pole kidney access in the prone position for PCNL patients (15.1% vs 6%). 9
One of the clinically significant findings of the current study is that in the prone position, the kidneys are located significantly more cranial compared with supine images: 80.4 mm vs 60.8 mm (left kidney) and 87.2 mm vs 57.4 mm (right kidney). In 1987, Preminger and coworkers already reported a cephalad kidney movement of 2 to 3 cm for PCNL patients in the prone position. 10 This 2-cm change can make access of upper pole RCN significantly more challenging, particularly for right-sided cases. The upward movement of the kidneys in the prone position may be responsible for the finding that the pleura covered more of the kidney on the right side in the prone position. For upper pole tumors, it may be prudent to get preprocedure imaging in the prone position. This may be particularly valid for right-sided lesions. With regard to the asymptomatic pneumothorax, Park and Kim evaluated prognostic factors influencing the development of an iatrogenic pneumothorax during image-guided procedures of upper pole tumors. 11 The authors demonstrated that preprocedure CT scans in the prone position are highly diagnostic in regard to intervening lung tissue and iatrogenic pneumothorax. This finding correlates well with our data; the patient with the asymptomatic pneumothorax was treated for an upper pole tumor on the left side.
The anatomic changes noted in this study have already altered our clinical technique as patients with right upper pole tumors undergo prone CT scan before the planned procedure to optimize treatment plans. In an effort to minimize radiation exposure, these prone CT scans are performed without contrast and are limited only to the upper abdomen.
Conclusion
There are specific clinically relevant and reproducible anatomic differences between the prone and supine positions during CT imaging of the kidney. Knowledge of the anatomic changes between the supine and prone positions can help the urologist and radiologist to establish an optimal treatment plan for CT-guided ablative therapy. In selected patients, a limited scope noncontrast upper abdominal CT scan may be helpful in small RCN ablative treatment planning.
Footnotes
Author Disclosure Statement
No competing financial interests exist.