
Abstract
Background and Purpose:
Flexible ureterorenoscopy (F-URS) plays a major role in the management of kidney stones. Ureteral access sheaths (UAS) are important tools for F-URS. In this study, we aimed to evaluate the difference in intrarenal pressures between different flexible ureteroscopes while using the same UAS and to calculate the irrigation flow variance.
Materials and Methods:
Eight different flexible ureteroscopes were tested with five different UAS on an artificial kidney model to measure intrarenal pressures and irrigation flow. Irrigation at 60 cmH2O pressure was performed; the pressure and the irrigation flow amount were recorded with different states of the operator channel: Free, with the laser fiber (272 μm), and with the nitinol basket (1.9F) inside.
Results:
The highest pressure recorded was 46.68 cmH2O with Wolf Boa and 9.5/11.5F Cook Medical UAS. All the ureteroscopes that fit inside the 10/12F Coloplast ReTrace provided pressures below 40 cmH2O. The inner diameter of the 10/12F Rocamed Bi-Flex is actually 11F, so intrarenal pressures were lower and irrigation flow was higher. With the 11/13F Boston Scientific Navigator HD and 12/14F Coloplast ReTrace, the pressures were very low. The irrigation flow measurements were in concordance with pressure measurements.
Conclusion:
The ureteroscope sizes diminished with advancements in technology. Small-sized ureteroscopes can provide low intrarenal pressures with good irrigation flow when used with convenient small-sized access sheaths. The compatibility between the ureteroscopes and UASs should be anticipated by all endourologists and considered during F-URS. The advantages of 10/12 UASs in terms of intrarenal pressure and irrigational flow should make these access sheaths an interesting first-line choice.
Introduction
O
Different ureteroscopes have different thicknesses and tip configurations, however, and the inner width of the UASs may vary. The intrarenal pressures and irrigation flow may differ not only according to these properties but also with the instruments occupying the operator channel of the ureteroscope. Therefore, to find a compatible relationship of ureteroscopes with UASs, we aimed to test different devices with different UASs. The aim of the study was to evaluate on a bench model the intrarenal pressure and irrigation flow variance for different flexible ureteroscopes while using the same UAS.
Materials and Methods
This study was conducted in a single institution laboratory setting with objective evalution. A bladder evacuator (Boston Scientific) was used as an artifical kidney because of its flexible nature, and the cap was reinforced with a nephroscope operator channel insertion cap (Karl Storz) and a rubber cap (Cook Medical) to provide a closed system and to prevent any leakage around the UAS. The artificial kidney model is shown in Figure 1. The pressure inside the bench model was measured in mmHg with a pressure fiber (St. Jude Medical) passing outside the UAS and was converted to cmH2O. The system was completely closed; the only back flow was on the side of the ureteroscope inside the UAS. The study setting is shown in Figure 2.

Boston Scientific bladder evacuation device enforced by two rubber caps to create a closed-system artificial kidney model. Color image available online at

Study setting.
We tested eight flexible ureteroscopes with five different UAS. The digital ureteroscopes were Karl Storz Flex-XC, Olympus URF-V2, Olympus URF-V, Richard Wolf Cobra Vision, and Richard Wolf Boa, and the fiberoptic ureteroscopes were Olympus URF-P6, Karl Storz Flex-X2, and Olympus URF-P5; the access sheaths were 9.5/11.5F Cook Medical, 10/12F Coloplast ReTrace, 10/12F Rocamed Bi-Flex, 11/13F Boston Scientific Navigator HD, and 12/14F Coloplast ReTrace UAS.
Among these ureteroscopes, Olympus URF-P6 was the thinnest ureteroscope and the Storz Flex-XC was the thinnest ureteroscope among the digital ones. Olympus URF-P6 and Olympus URF-V2 represent the newer and thinner versions of Olympus URF-P5 and Olympus URF-V, respectively. Wolf Cobra Vision is a digital ureteroscope with two operator channels that can provide the endourologist an advantage during endoscopic stone surgeries.
Using the endoflow pump, 4 minutes of irrigation was performed at 60 cmH2O pressure with the Rocamed TraxerFlow irrigation system to achieve a steady state for the artificial intrarenal pressure. Afterward, the pressure and the irrigation flow amount were recorded at the end of each minute with different states of the operator channel: Free, with the laser fiber (272 μm), and with the nitinol basket (1.9F) inside, respectively. This sequence of tests was repeated three times for each combination of ureteroscope and UAS, to evaluate any variation.
During this study, we created a microscopic imaging setting using a surgical microscope combined with the Storz endoscopic imaging system to record microscopic images of the access sheath tips. The UASs were placed perpendicular to the microscope, adjacent to a surgical ruler. Photos were taken with the highest zoom possible that did not influence the visual quality of the image with 12× magnification. The inner and outer diameters were measured using the adjacent ruler as a reference.
The pressure values were measured in mm Hg and multiplied by 1.3595 to calculate the values in cm H2O, because pressure values in cm H2O are frequently used in our department to determine irrigational pressures. The irrigation flow values are given in mL/min.
The data are presented as mean values and analyzed with GraphPad Prism5 and IBM SPSS Statistics Version 22. Descriptive statistics are given to demonstrate the differences between each combination.
Results
The statistical analyses were performed to compare the measured pressure values inside each UAS. For each ureteroscope, the Kruskal Wallis test was performed to see if there was a significant relationship, which showed that for each ureteroscope, there was a significant statistical difference (P < 0.05). Afterward, the Mann Whitney U test was performed to reveal individually the significant differences for each UAS.
Olympus URF-P6, Storz Flex-X2, and Wolf Boa were the only ureteroscopes that could fit inside the smallest access sheath, 9.5/11.5F Cook Medical. Olympus URF-V was the largest ureteroscope with a 10.9F diameter and could fit only inside the 11/13F Boston Navigator HD and 12/14F Coloplast ReTrace. The highest pressure recorded during the study was 46.68 cm H2O with the combination of Wolf Boa and 9.5/11.5F Cook Medical UAS. Although the Storz Flex-XC was smaller in diameter than the Wolf Boa, it did not fit inside the 9.5/11.5F Cook Medical because of its oval tip configuration. All the ureteroscopes that could fit inside the 10/12F Coloplast ReTrace provided pressures below the limit for intrarenal reflux, which is 40 cm H2O. The visual comparison is given as a table in Figure 3.
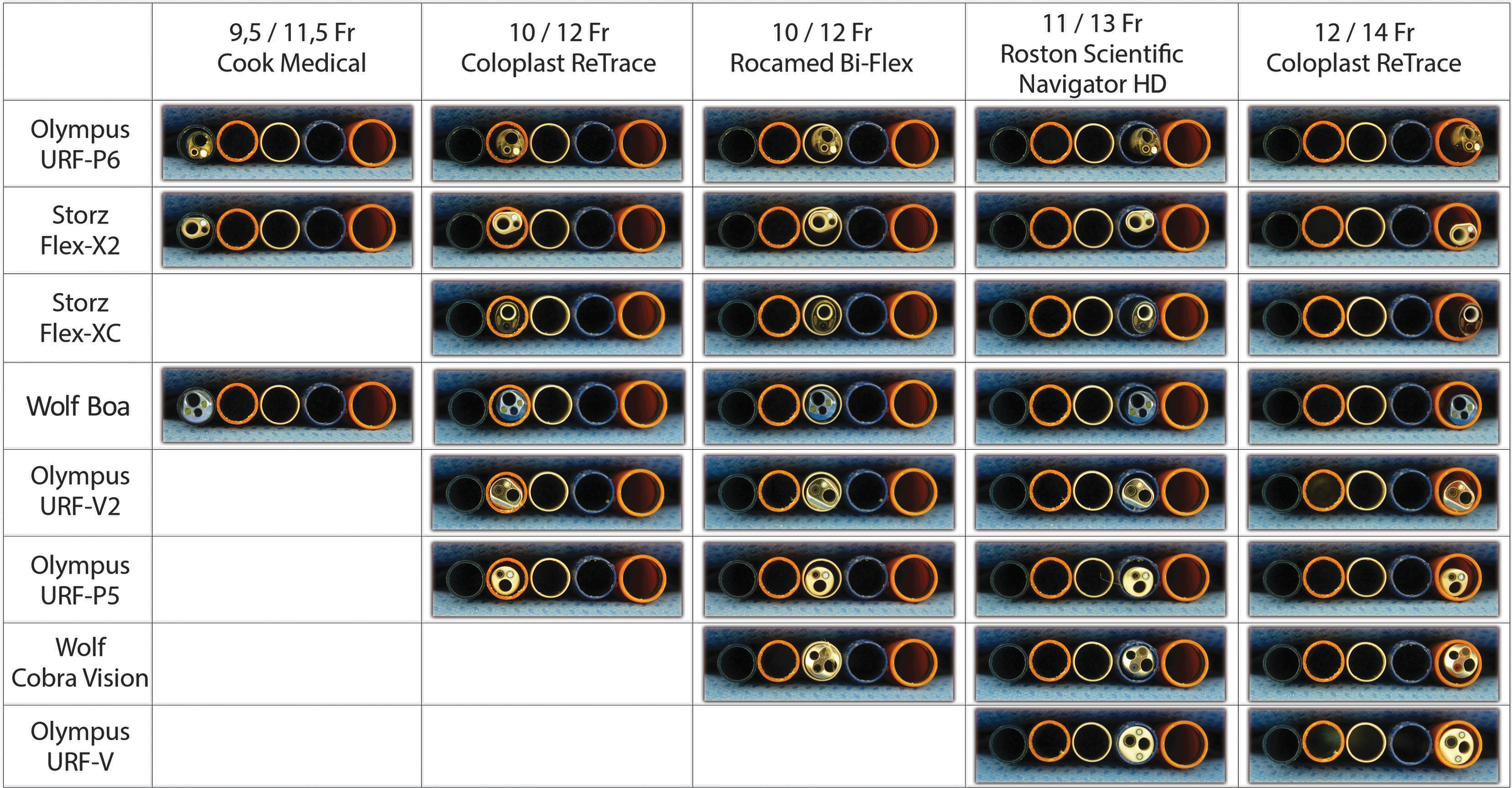
Flexible ureteroscopes inside the ureteral access sheaths. Color image available online at
The pressure values were highest when the operator channel was empty and lowest when the channel was occupied with the basket catheter. The irrigation flow values were inversely proportional to pressure values: Highest in the empty channel and lowest in basket-occupied channel.
The pressure values of Olympus URF-P6, Storx Flex-X2, and Wolf Boa were statistically significantly higher inside the 9.5/11.5F Cook UAS when compared with the values inside the 10/12F Coloplast ReTrace UAS (P < 0.005). The pressure values of Olympus URF-P5, Olympus URF-V2, and Wolf Boa were statistically significantly higher inside the 10/1F Coloplast ReTrace UAS when compared with the values inside the 10/12FrRocamed Bi-Flex UAS (P < 0.01, P < 0.005, P < 0.05, respectively).
Olympus URF-P5, URF-P6, URF-V2, Storz Flex-X2, Flex-XC, and Wolf Cobra Vision had statistically significantly higher pressure values inside 10/12F Rocamed Bi-Flex when compared with values inside 11/13F Boston Scientific Navigator HD (P < 0.05, P < 0.005, P < 0.05, P < 0.01, P < 0.01, P < 0.001 respectively). Olympus URF-V was the only ureteroscope to have significantly higher pressure values inside the 11/13F Boston Scientific Navigator HD when compared with the 12/14F Coloplast ReTrace (P < 0.01). All the pressure and irrigation flow measurements are given in Table 1, and these values are given individually for each ureteroscope as line graphs in Figure 4.
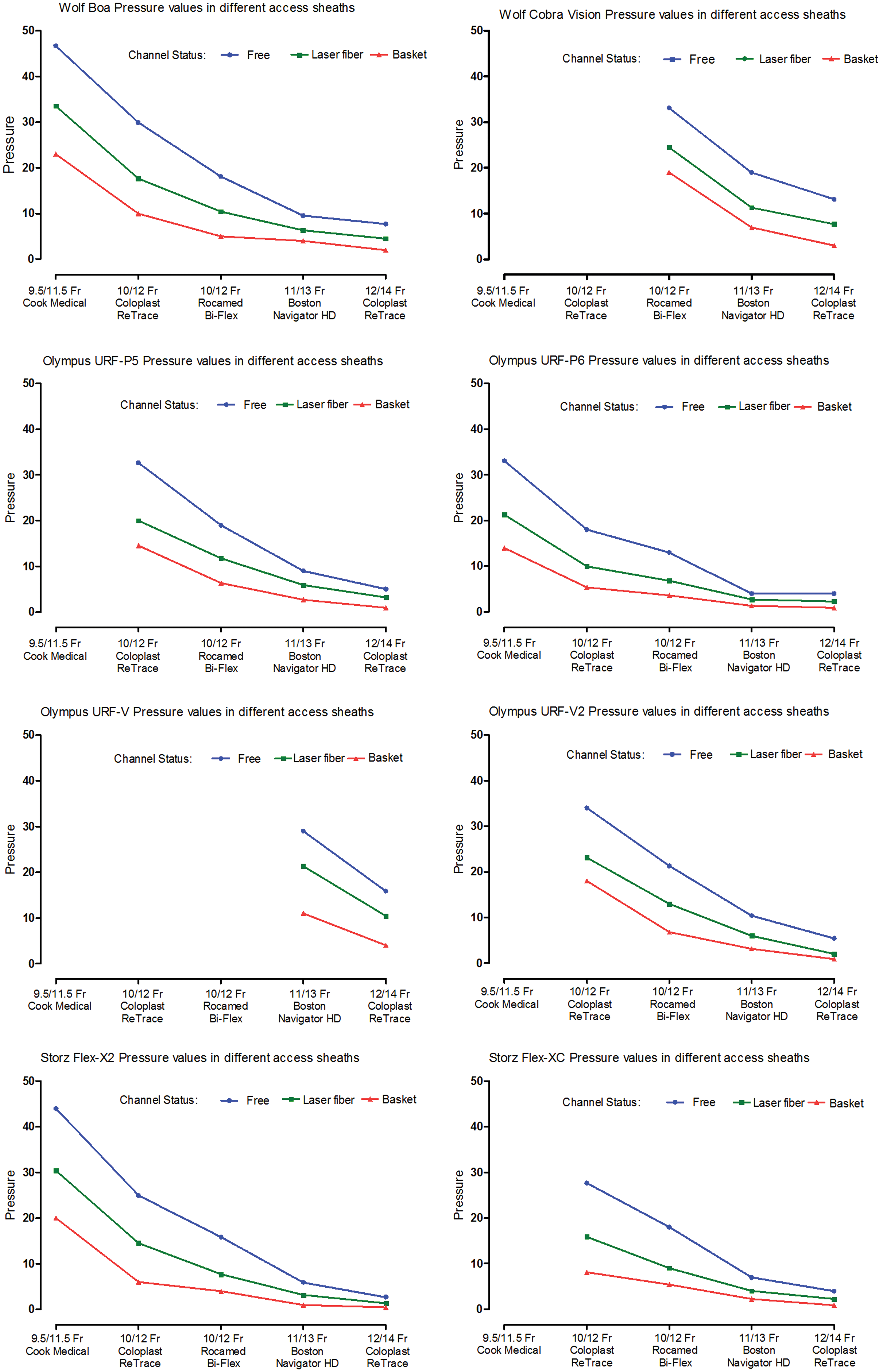
Line graphs of pressure measurements for each ureteroscope. Color images available online at
Pressure values are given in cm H2O, and irrigation flow values are given in mL/min.
Discussion
Since the introduction of flexible ureteroscopes to modern medicine in the late 1980s, the indications for flexible ureteroscopic surgeries have expanded to a wide spectrum in all locations of the collecting system. Lately, the wide use of UASs have reduced patient morbidity, improved stone-free rates, reduced costs, and provided surgeon comfort by allowing multiple passages into the collecting system. 6,7
During F-URS, because of the irrigation solution flow and irrigational pumping, pyelosinus, pyelovenous, and/or pyelolymphatic backflow of irrigant solution may occur and is hypothesized to start at pressures above 40 cmH2O. 2,8,9 It is common practice to pressurize the irrigant during F-URS to provide a clear view for the endourologists, and so this backflow is almost inevitable.
Keeping the intrarenal pressures below the limit for intrarenal and pyelosinous backflow, which is 40 cmH2O, may prevent complications such as infection and urosepsis. Schwalb and associates 10 showed that high-pressure irrigation during URS in pigs caused irreversible, deleterious effects in the kidney parenchyma, and it is proposed that infectious complications may result from bacterial translocation and renal extravasation.
Because of this pyelosinus, pyelovenous, and/or pyelolymphatic backflow and consequently morphologic and physiologic changes in the renal parenchyma, effort is now being spent on ways to decrease these elevated pressures. Apart from the UAS and miniaturized endoscopic equipment, pharmacologic agents are also studied. Jung and colleagues 11 demonstrated in a controlled study in pigs that irrigation with isoproterenol (ISO) can effectively reduce renal pressures during F-URS without side effects. They also showed in another study that ISO in very low concentrations added to the irrigating saline could reduce pressure significantly during F-URS in humans without side effects. 12
The intrarenal pressures and irrigation flow measurements may change proportionally according to different irrigation pressures. In the study of Rehman and coworkers, 2 when no UAS was in place, at 50, 100, and 200 cm H2O irrigation pressures through the ureteroscope, the pressures in the cadaveric kidneys were approximately 15, 30, and 55 cm H2O and irrigation flow measurements were 23, 47 and 80 mL, measured every 3 minutes. As also shown in the same study, the pressure inside the kidney and the irrigation flow measurements were the same with 14F and 16F UAS; the maximum flow rate was achieved with both of the UASs, and no change was recorded in pressure measurements. Despite this information, we should always keep in mind that these properties may vary with different ureteroscopes because they used a 7.5F ureteroscope. 2
The most commonly used UAS when dealing with renal calculi are the 12/14F access sheaths. With the miniaturization of the ureteroscopes, the 10/12F UASs are also becoming more widely used. In the study of Rehman and colleagues, 2 when a 12/14F UAS was used, the pressures inside the cadaveric kidneys were significantly lower and the irrigation flow rates were significantly higher than the situation when no UAS was used.
Auge and associates 3 also published in their study that the intrarenal pressures without an UAS were significantly greater when the ureteroscope was placed in the distal, middle, and upper ureter and the renal pelvis. They showed that the UASs may provide protection against elevated intrarenal pressures by a reduction of 57% to 75%. 3 The miniaturization of ureteroscopes and consequently the UASs provided an increase in F-URS success rates and a decrease in the need for stent preplacement. Our results show that with relatively bigger UASs, because of high irrigation flow, intrarenal pressures are very low, but there is a compromise in ureteral wall safety.
Traxer and coworkers 13 showed in their study of 359 patients that severe ureteral wall injury involving ureteral smooth muscle layers is not rare after insertion of a 12/14F UAS, and the incidence of postoperative pyelonephritis is higher with higher grade UAS-related injury. Therefore, it should be kept in mind that bigger UASs do not always mean safety.
With this information, effort is being spent on miniaturization of UASs with which the incidence of ureteral damage and subsequently infectious complications are expected to decrease. The question of which ureteroscope was compatible with which UAS seemed to be a mystery until in March 2014, Al-Qahtani and coworkers 14 established a correlation table with 21 different UAS and 12 different ureteroscopes and concluded that 10/12F UASs would become the new standard UAS that accept all endoscopes with low friction rates.
To improve procedure efficacy, ureteroscope durability and reduce costs, the right choice of endoscopes and materials must be made for different occasions. Therefore, when efficacy and safety are considered, endourologists must know which UAS to use with their ureteroscope. Although Al-Qahtani and associates 14 summarized very well in their study, the importance of intrarenal pressures must also be taken into account. With this point of view, we decided to see the intrarenal pressures and irrigation flow measurements in an artificial kidney model by using eight different ureteroscopes and five different UAS with different instruments inside the operator channel of the ureteroscope.
Despite the miniaturization, the digital ureteroscopes are generally slightly larger in diameter than the fiberoptic ureteroscopes. Although the choices may vary, with the excellent endoscopic vision provided by these scopes, they are becoming the first line of choice for many endourologists. In our study, when compared with the fiberoptic ureteroscopes, intrarenal pressures are higher and irrigation flow rates are lower with digital ureteroscopes.
When digital ureteroscopes were compared with small-sized UASs, lowest pressures were achieved with Storz Flex-XC, Wolf Boa, and Olympus URF-V2, respectively. Because of its oval tip configuration, however, Storz Flex-XC did not fit into the 9.5/11.5F Cook Medical UAS, and Wolf Boa was the only one that could fit. With the larger-sized 12/14F ReTrace Coloplast UAS, all the digital ureteroscopes provided very low intrarenal pressures; the highest pressures were provided by two ureteroscopes, the Olympus URF-V, the older version of the Olympus digital endoscope, and Wolf Cobra Vision, the only ureteroscope with two working channels used in our study.
As fiberoptic ureteroscopes were compared, Olympus URF-P6 was the thinnest one even among all the ureteroscopes in the study, which eventually provided the lowest pressures for all different sizes of UASs and highest irrigation flow rates. All the characteristics of different ureteroscopes were taken from the manufacturers' official websites and are summarized in Table 2.
In all the ureteroscope-UAS combinations, the pressure measurements were higher when the operator channel was empty and diminished when a 272 μm laser fiber was inserted and were even lower when a 1.9F nitinol basket was inside, because of the diminished irrigation. With 10/12F Rocamed Bi-Flex UAS, the pressures were lower and irrigation flow measurements were higher than the same sized 10/12F Coloplast ReTrace, because the former has actually an inner width of 10.9F instead of 10F, as claimed by the company, as demonstrated by Al-Qahtani and coworkers 14 in their study in which they confirmed with a laboratory measurement. 8 We measured the inner and outer diameters of all UASs used in the study. The values are given in Figure 5.
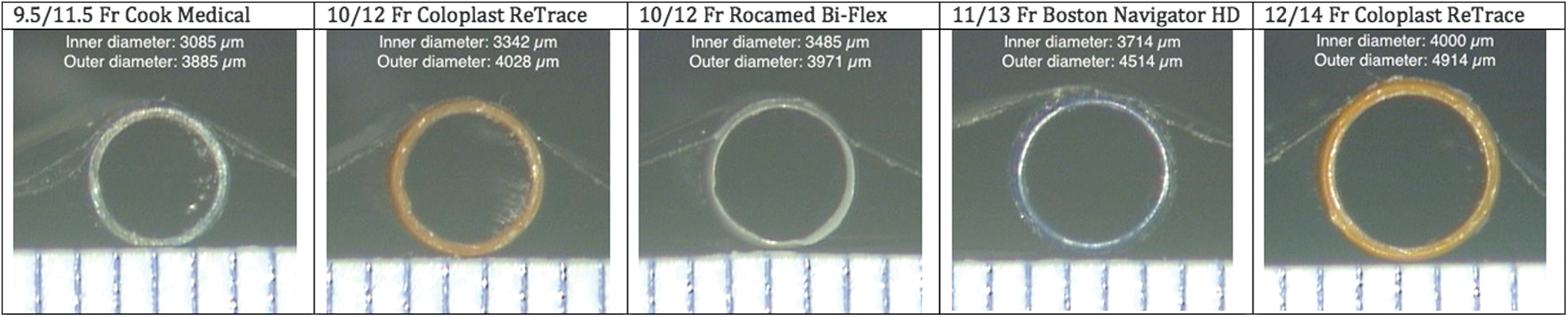
Microscopic images of the ureteral access sheaths. Color images available online at
During F-URS, the majority of the time is spent with the laser fiber inside the endoscope. The endoscope is used with a free channel to investigate and irrigate the collecting system, and a nitinol basket is generally used toward the end of the operation to collect stone fragments. Therefore, knowledge of the pressures when the laser fiber is inside the endoscope is essential to decide which UAS to use with each ureteroscope.
Because ureteral safety is one of the most important issues, it may seem that 9.5/11.5F Cook Medical UAS can be the first choice, but when it comes to intrarenal pressures, even for the smallest ureteroscopes, the pressures are above 25 cmH2O for Wolf Boa and Storz Flex-X2. It is also not practical to use this access sheath, because there are few endoscopes that can fit inside.
In our measurements, 10/12F Coloplast ReTrace provided pressures below 25 cmH2O for every ureteroscope that could fit inside. The 10/12F Rocamed Bi-Flex also provided lower pressures, and also it is actually a 11/12F, so with the same outer diameter as the 10/12F Coloplast ReTrace, ureteral damage risk is somewhat alike; because of its larger inner diameter, however, it has the advantage of lower intrarenal pressures.
With the larger UAS, 11/13F Boston Navigator HD and 12/14F Coloplast ReTrace, the pressures can be very low with the expense of safety. When using a larger ureteroscope such as Olympus URF-V or Wolf Cobra Vision, however, the access sheath options are limited to these larger UAS. Both of them provide pressures below 25 cm H2O and seem to be convenient for these two endoscopes. The conventional and globally frequently used 12/14F Coloplast ReTrace UAS was slightly better in terms of pressure-irrigation flow ratios.
With all this information, in terms of artificial intrarenal pressures and irrigational flow, 10/12F UASs, and also among the two, Rocamed Bi-Flex UAS seems to be a safer choice because of its larger inner diameter and lower pressures provided with it, as also stated by Nagele and colleagues 15 in their study. Even with the advantage of being the smallest UAS, the 9.5/11.5F Cook Medical access sheath seems to be a second-line choice if you do not have an Olympus URF-P6 because of the high intrarenal pressures that come along and also the fact that many of the flexible ureteroscopes do not fit inside.
Our study has limitations. The different characteristics of the UASs as to lubricity, tapering of the tip, and shaft stiffness, which can also affect their safety potential, were not taken into account in our study. The study was conducted in a laboratory setting, so what happens in vivo is one of the questions we must find out in the future. Moreover, this study was conducted with an irrigation of 60 cm H2O. The pressures inside the kidney during an ureteroscopic procedure vary with pumping and may differ according to the irrigation systems used. Also, during F-URS in vivo, there is a potential flow of irrigation solution between the ureter and the UAS, especially with dilated ureters, which was not included in our study. Different conditions must be created to see the variances with different systems and settings.
Conclusion
The ureteroscope sizes diminished with advancements in technology. Small-sized ureteroscopes can provide low intrarenal pressures with good irrigation flow when used with convenient small-sized access sheaths. The compatibility between the ureteroscopes and UASs should be anticipated by all endourologists and considered during F-URS. The advantages of 10/12 UASs in terms of intrarenal pressure and irrigational flow should make these access sheaths an interesting first-line choice.
Footnotes
Author Disclosure Statement
Professor Traxer is a consultant for Olympus, Rocamed, and Coloplast in research and development. For the remaining authors, no competing financial interests exist.