
Abstract
Introduction:
One third of men undergoing radical prostatectomy have a comorbid inguinal hernia (IH). Previous studies have shown that adding total extraperitoneal (TEP) IH repair to extraperitoneal laparoscopic radical prostatectomy (LRP) lacks adverse effects. However, outcomes of extraperitoneal robot-assisted laparoscopic radical prostatectomy (RALP) and TEP are unknown. We compared RALP+TEP with LRP+TEP and also with RALP alone.
Methods:
Eleven RALP+TEP cases were retrospectively compared with 26 LRP+TEP cases and 22 control RALP without TEP. Outcomes compared between groups included operative time, estimated blood loss (EBL), discharge hematocrit (hct), time to diet advancement, length of hospital stay (LOS), postoperative complications, and hernia recurrence.
Results:
Unilateral TEP added 32 minutes to RALP and 31 minutes to LRP, whereas bilateral TEP added 80 minutes to RALP and 36 minutes to LRP. There were no differences between RALP+TEP and LRP+TEP or RALP without TEP controls in regard to EBL, discharge hct, time to diet advancement, LOS, or postoperative complications. One patient developed an anterior mesh seroma, which resolved without intervention. No IH recurrences were noted on the mean follow-up of 33 months in the RALP group and 50 months in the LRP cohort.
Conclusions:
Unilateral and bilateral TEP added operative time to RALP but had equivalent outcomes to both LRP+TEP and RALP alone. This is likely due to the similar surgical space used for RALP and TEP, which obviates the need for substantial further dissection. For men with prostate cancer and comorbid IH, combined RALP+TEP appears to be an appropriate surgical combination.
Introduction
P
Previously reported series have investigated outcomes of extraperitoneal laparoscopic radical prostatectomy (LRP) with concurrent total extraperitoneal inguinal hernia repair with mesh (TEP-IHR or simply TEP) and found that there is no increase in complications, operative time is 15–30 minutes longer, and postoperative pain levels are similar. 8 –11 TEP performed during transperitoneal extraperitoneal robot-assisted laparoscopic radical prostatectomy (RALP) has also been reported and shown to add an additional 10 to 20 minutes of operative time, without additional postoperative narcotic requirements, length of hospital stay (LOS), estimated blood loss (EBL), or short-term postoperative complications. 12,13 There are no reports, to our knowledge, on outcomes of RALP with TEP or how this modality is compared with LRP+TEP. An extraperitoneal RALP approach may have several advantages, including preservation of an intact peritoneal cavity, and has been associated with decreased operative time and LOS compared with a transperitoneal approach. 14,15 Similarly, in the setting of TEP, a total extraperitoneal approach has been shown to decrease LOS compared with the transperitoneal (TAPP) hernia repair approach and precludes the mesh contact with the bowel and decreases the potential of mesh erosion into the bowel. 16 Combining TEP with RALP avoids staged procedure(s) for the patient and allows for IHR in a space already predissected for the RP, particularly when associated with pelvic lymph node dissection (PLND).
We retrospectively compared our experience of RALP±TEP with LRP+TEP and with a control group of RALP without hernia repair. We sought to identify the amount of time required for TEP during RALP (performed with and without concomitant PLND) and to determine if there were differences in EBL, LOS, diet advancement, discharge hematocrit (hct), and postoperative complications compared with patients who had RALP without TEP or who underwent extraperitoneal LRP and TEP.
Materials and Methods
A prospectively maintained institutional review board-approved database of LRP and RALP, performed by a single surgeon between September 2005 and September 2014, was queried for simultaneous performance of TEP. LRP was used preferentially from 2005 to 2010, and RALP was utilized preferentially beginning in 2010. TEP was performed immediately following urethral reanastomosis during RALP or LRP in a robot-assisted or laparoscopic manner, consistent with the modality utilized for prostatectomy by the urology team. The same port placement and robot location were used.
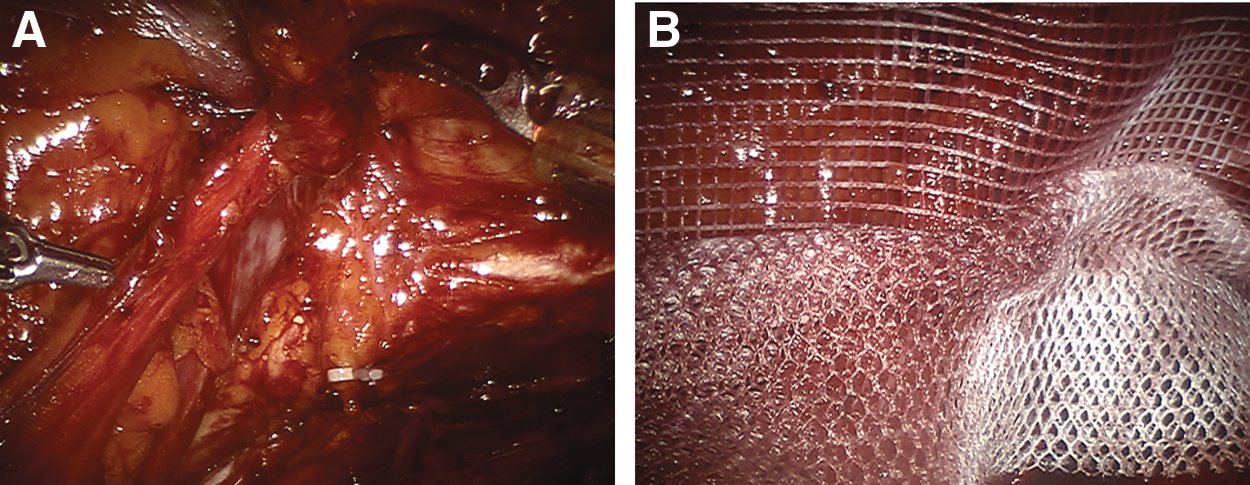
During LRP cases, hernia repair was performed by either the primary urologic surgeon or a consultant general surgeon, while in RALP cases, all hernia repairs were performed by a consultant general surgeon after the prostatectomy. The extraperitoneal space was first created with an insufflation balloon and was then insufflated to 15 mmHg. After four to five angled ports were placed into the space of Retzius in a fan-shaped configuration across the lower abdomen, the RP was performed in the standard extraperitoneal robotic manner. PLND was also performed in the majority of cases (based on PC risk stratification) and involved dissection of the obturator and external iliac lymph nodes up to the bifurcation of the common iliac artery. No extra ports were placed for the subsequent hernia repair, and the same port placement was used in both robotic and laparoscopic cases. On the side of the hernia, its contents were reduced, and the space was cleared for placement of prosthetic mesh. The hernia sac was completely reduced, and the synthetic mesh was inserted through the 12-mm port and used to reinforce the myopectineal orifice (Fig. 1). 3D Max mesh (Bard™) was used in LRP cases, and Parietex anatomic mesh (Covidien™), a multifilament polyester mesh, was used in RALP cases. Nonabsorbable tacks were used in LRP+TEP cases, and when absorbable tacks became available, they were used in RALP+TEP cases to secure the mesh as per surgeon's preference.
Between September 2005 and September 2014, 1020 RPs were performed laparoscopically or with robotic assistance. The majority utilized an extraperitoneal approach. Men who underwent extraperitoneal RALP+TEP were compared with age- and era-matched patients, who had extraperitoneal RALP without TEP as well as a cohort of patients who underwent LRP+TEP. Patient age, body–mass index (BMI), prostate-specific antigen (PSA), Gleason grade, and prostate size were recorded preoperatively. Operative times for TEP alone were available for RALP cases and were reported. Operative times for TEP alone in LRP cases were available for half of the cases performed. Performance of PLND (±), EBL, LOS, postoperative day (POD), on which diet was advanced, discharge hct, and operative and 90-day postoperative complications were noted. Student's t-test and Pearson's χ2 test were used to determine statistical significance. All analyses were performed using R, version 3.1.2. A p-value of <0.05 was considered significant.
Results
Eleven RALP+TEP were performed with 3 concomitant bilateral and 8 unilateral hernia repairs. Bilateral repairs added a mean of 80 ± 38 minutes to operative time, and the unilateral repairs added a mean of 32 ± 6 minutes. For the RALP/+PLND+unilateral TEP cohort, there was a mean of 34 ± 7 minutes of additional operative time (n = 7). In cases in which PLND was not performed (RALP/−PLND+unilateral TEP), the hernia repair added a mean of 30 minutes (n = 1). Twenty-six LRP+TEP cases were performed with 5 concomitant bilateral and 21 unilateral hernia repairs. Bilateral and unilateral repairs added a mean of 36 ± 0 and 31 ± 12 minutes, respectively. LRP/+PLND+unilateral TEP took 33 ± 13 minutes (n = 8), and LRP/-PLND+unilateral TEP took 26 ± 8 minutes (n = 4).
As shown in Table 1, the groups were well matched, without significant differences in age, BMI, PSA, Gleason grade, or prostate size (Table 1). When RALP+TEP was compared with RALP alone, there were no significant differences in the mean EBL (209.1 ± 76.9 mL vs 202.4 ± 55.8 mL, p = 0.80), discharge hct (35.6% ±2.7% vs 36.5% ±3.5%, p = 0.41), POD diet advancement (1 day vs 1 day, p = 1.0), and LOS (1.4 ± 0.5 days vs 1.4 ± 0.5 days, p = 0.64). Similarly, when RALP+TEP was compared with LRP+TEP, there were no significant differences in the mean EBL (209.1 ± 76.9 mL vs 223.7 ± 144.7 mL, p = 0.72), discharge hct (35.6% ±2.7% vs 36.1% ±3.9%, p = 0.62), POD diet advancement (1 day vs 1 day, p = 1.0), or LOS (1.4 ± 0.5 days vs 1.5 ± 0.5 days p = 0.46) (Table 2).
p-Values derived from comparison of RALP+TEP with RALP and with LRP+TEP.
BMI = body mass index; PLND = pelvic lymph node dissection; PSA = prostate-specific antigen; RALP = extraperitoneal robot-assisted laparoscopic radical prostatectomy; SD = standard deviation; TEP = total extraperitoneal; LRP = extraperitoneal laparoscopic radical prostatectomy.
p-Values derived from comparison of RALP+TEP with RALP and with LRP+TEP.
EBL = estimated blood loss; hct = hematocrit; LOS = length of hospital stay.
There were no postoperative complications in the RALP+TEP group; however, one patient developed a Clavien grade 1 complication (seroma anterior to the mesh, which resolved without intervention). One of the 20 patients in the RALP control group had a Clavien grade IIIa complication (lymphocele development requiring percutaneous drainage). All 11 RALP+TEP patients were hernia recurrence free at a mean follow-up of 28 months (range 3–51 months). Similarly, there were no complications in the LRP with TEP group. Twenty-four of the 26 patients in the LRP+IHR group returned for follow-up and had a mean follow-up of 50 months (range 1–110 months) without hernia recurrence.
Discussion
PC and IH are frequently comorbid and may be treated during a single operation. To our knowledge, there are no series reporting concurrent robotic prostatectomy and hernia repair using an extraperitoneal approach, and it is unknown how this is compared with a laparoscopic approach. We found in RALP cases that bilateral TEP added a mean of 80 minutes and unilateral TEP added a mean of 32 minutes. We thought that the performance of PLND with the RP might reduce the time needed for TEP, since the spaces dissected overlap, but found that not to be the case. Time requirements were similar in the LRP cohort: unilateral TEP added a mean of 31 minutes; however, bilateral repairs added only a mean of 36 minutes. Performance of concomitant PLND again did not substantially affect TEP times. RALP+TEP was equivalent to RALP alone and LRP+TEP-IH in regard to EBL, discharge hct, LOS, time to diet advancement, or postoperative complications. Finally, no hernia recurrences were noted in either cohort at a mean follow-up of 33 months for RALP TEP and 50 months for LRP TEP cases.
The similar dissection and structure identification required for extraperitoneal prostatectomy and hernia repair nevertheless likely underlie our lack of finding any significant differences in perioperative parameters when performed concurrently. The fact that no additional ports were required for performance of concomitant RALP and TEP also likely played a role in the lack of appreciable extra morbidity from the simultaneous performance of these procedures. Our findings are similar to series looking at combined transperitoneal RALP with hernia repair that found an increase in operative time of 10 to 20 minutes without significant changes in operative or postoperative factors, including LOS, EBL, and complications. 12,13 In these studies, hernia repair was performed by the urologic surgeon performing the prostatectomy. Hernia repair in our cohorts took slightly longer, particularly robotic bilateral TEP, but with additional experience the times are decreasing. Our longer TEP times are likely related, in part, to the use of a second (general surgical) team to perform the mesh hernia repairs, which, although experienced in laparoscopy, did not at series-start have the same breadth of experience with robotics as robotic assistance is not commonly used by general surgeons for TEP. Before the robotic era, our hospital recruited several general surgeons with expertise in laparoscopic and eventually robot-assisted laparoscopic IHR. Due to our tertiary care center's goal of providing excellence in patient care, these surgeons were invited to perform the hernia repairs at the conclusion of the RP. The general surgeon involved in the robotic TEP in this study was more expert at laparoscopy than robot-assisted laparoscopy and did not have the experience of using robotic assistance for TEP until the cases reported in this series. Nevertheless, the ultimate outcomes were excellent, and time was likely saved by avoiding undocking of the robot and adding laparoscopic ports for TEP. The longer times may also, in part, be attributable to unquantified patient variables given the small size of our series, particularly in terms of bilateral TEPs.
Our study does have limitations. As noted, the series is relatively small, particularly the RALP subsets, which may obscure currently undetected operative disadvantages and may be responsible, in part, for the wide range of operative times attributable to TEP. EBL in the LRP and RALP with TEP tended to be higher, and greater power could reveal this to be statistically significant. In addition, different surgeons performed the hernia repairs, while the urologic surgeon was the same throughout the series, which may add variability to our results. Finally, extraperitoneal RP is less commonly performed than transperitoneal RP, and our results may not be generalizable across approaches. However, and most importantly, there were no hernia recurrences noted in either of our LRP or RALP cohorts over intermediate-term follow-up and no differences in complications between these patients and matched controls.
Given the high incidence of IH among older men and increased risk of IH following RP, our results suggest that men with PC undergoing extraperitoneal robot-assisted RP may benefit from thorough preoperative and intraoperative examinations to detect IH, as these can safely and effectively be repaired during RP, thus avoiding additional operations and expenses.
Conclusions
Our study shows that extraperitoneal robot-assisted RP and concomitant TEP repair are safe, effective, and comparable to a laparoscopic approach. Approximately 30 minutes of additional operative time is required for concomitant TEP, but there do not appear to be additional drawbacks or specific urologic or infectious complications, and patients were able to avoid a staged procedure for their IHs. For men who are undergoing extraperitoneal RP for PC who have comorbid IH(s), a combined procedure should be considered.
Footnotes
Author Disclosure Statement
No competing financial interests exist.