
Abstract
Background and Purpose:
Bipolar energy has recently been used as a common alternative to conventional monopolar transurethral resection of the bladder (TURB) while managing nonmuscle-invasive bladder cancer (NMIBC). We established a meta-analysis comparing the safety and efficacy of plasmakinetic bipolar and monopolar TURB for NMIBC.
Methods:
A systematic search of PubMed, MEDLINE, Web of Science, and China National Knowledge Infrastructure was performed up to March 1, 2015. Outcomes of interest assessing the two techniques included demographic and clinical baseline characteristics, perioperative variables, and complications.
Results:
Eight eligible trials evaluating bipolar TURB (bTURB) versus monopolar TURB (mTURB) for NMIBC were identified including six randomized controlled trials (RCTs), one prospective study, and one retrospective study. The bTURB was associated with shorter operative time (P = 0.002), shorter hospital stay (P < 0.001), less established blood loss (P < 0.001), and shorter catheterization time (P = 0.004). There were fewer complications such as obturator nerve reflex (P < 0.001) and bladder perforation (P = 0.003) in the bTURB group. The postoperative recurrence rate in 2 years also showed advantages of bTURB over mTURB.
Conclusion:
Our data showed that bTURB appeared to be a safe and efficient method and had presented several advantages when compared with conventional mTURB in the management of NMIBC. As a promising technique, bTURB may be used as a preferable choice instead of mTURB for superficial bladder tumor.
Introduction
B
Currently, transurethral resection of the bladder (TURB) has become the gold standard of the treatment of patients with nonmuscle-invasive bladder cancer (NMIBC); it is also used for the pathologic evaluation of bladder cancer of all stages or grades. 2,3 Conventionally, TUR is performed by monopolar electrocautery. Recently, plasmakinetic bipolar energy has also been used widely in the transurethral resection of the prostate (TURP) for benign prostatic hyperplasia.
Meta-analyses comparing monopolar and bipolar TURP showed that bipolar energy was associated with favorable outcomes with lower short-term complications, especially less hemorrhage and fewer cases of TUR syndrome. 4,5 In addition, bipolar TURB (bTURB) was also expected to present some advantages compared with monopolar TURB (mTURB) for the management of NMIBC. 6,7
In recent years, a number of studies have begun to compare the safety and efficacy between bTURB and mTURB, 8 –17 but it is difficult to detect low incidence events based on a single trial. Thus, we conducted a meta-analysis of the literature on the feasibilities and advantages of bTURB versus mTURB in terms of demographic and clinical baseline characteristics, and perioperative and postoperative variables.
Methods
Study selection
A systematic search of PubMed, MEDLINE, Web of Science, and China National Knowledge Infrastructure was performed to identify all studies published up to March 1, 2015 that compared bTURB with mTURB with following MESH search headings: “comparative studies,” “bipolar transurethral resection of bladder,” “monopolar transurethral resection of bladder,” and “nonmuscle-invasive bladder cancer.” The “related articles” function was used to broaden the search, and all abstracts, studies, and citations were reviewed.
Inclusion criteria and exclusion criteria
To be included in the analysis, studies were required to be: (1) randomized controlled trails (RCTs) or nonrandomized controlled trials (non-RCTs), (2) the comparison of bTURB with mTURB, (3) patients with NMIBC in the clinical stage of Ta, Tis or T1, (4) reports on at least one outcome of interest mentioned below, and the relative data were reported or could be calculated.
Studies were excluded in the meta-analysis if: (1) patients had muscle-invasive tumor or with metastasis, (2) no outcomes of interest (specified later) were reported or impossible to calculate or extrapolate the necessary data for either bTURB or mTURB from the published results, (3) children were included in the studies.
Data extraction and outcomes of interest
Two reviewers (ZCM and TK) independently extracted the following data including: first author, year of publication, country, study interval, study design, number of patients who underwent bTURB or mTURB, characteristics of the study population, and outcomes of interest. All disagreements about eligibility were resolved by a third reviewer (XH) by discussion until a consensus was reached. In all cases of missing or incomplete data, the corresponding authors were contacted, but no additional information was provided.
The following outcomes were extracted to compare bTURB and mTURB. Demographic variables were a series of patients' baseline characteristics including: age, proportion of males, tumor size, tumor stage, proportion of multiple tumors and proportion of who underwent previous surgery. Perioperative and postoperative variables included operative time, estimated blood loss, length of hospital stay, blood transfusion rate, drop in hemoglobin level, catheterization time, terminal damage causing histopathologic artifacts, complications including obturator nerve reflex and bladder perforation, and postoperative recurrence rate in 2 years.
Study quality and level of evidence
The level of evidence of included studies was rated according to criteria by the Centre for Evidence-Based Medicine in Oxford, United Kingdom. 18 Two reviewers (ZCM and TK) independently assessed the quality of the studies, and disagreement was resolved by consensus.
Statistical analysis
Our meta-analysis was performed according to the recommendations of the Cochrane Collaboration and the Quality of Reporting of Meta-analyses guidelines. 19 The weighted mean difference (WMD) was used for continuous variables, and the odds ratio (OR) was used for dichotomous parameters both with 95% confidence interval (CI). For studies presenting continuous data as means and range, we made an approximate transformation using the technique described by Hozo and associates. 20
All the pooled effects were determined by the z test, and P < 0.05 was considered statistically significant. The quantity of heterogeneity among included studies was assessed by chi-square–based Q test and I 2 test. When I 2 <50%, P > 0.05, the evidences showed no heterogeneity, we used the fixed-effects model; otherwise, we used a random-effects model. Sensitivity analyses were performed by omitting a certain study each time. We used funnel plots to assess publication bias. All the statistical analyses were performed using RevMan 5.3 (Cochrane Library Software, Oxford, UK).
Results
Characteristics of selected studies
A total of 221 records were retrieved through database searching; after screening, eight trials 8 –15 were selected in our meta-analysis (Fig. 1), including 490 patients undergoing bTURB and 500 patients undergoing mTURB, respectively. Six studies were RCTs, one study was a prospective case-control study, and the other one was a retrospective case-control study. The characteristics of these studies are shown in Table 1.
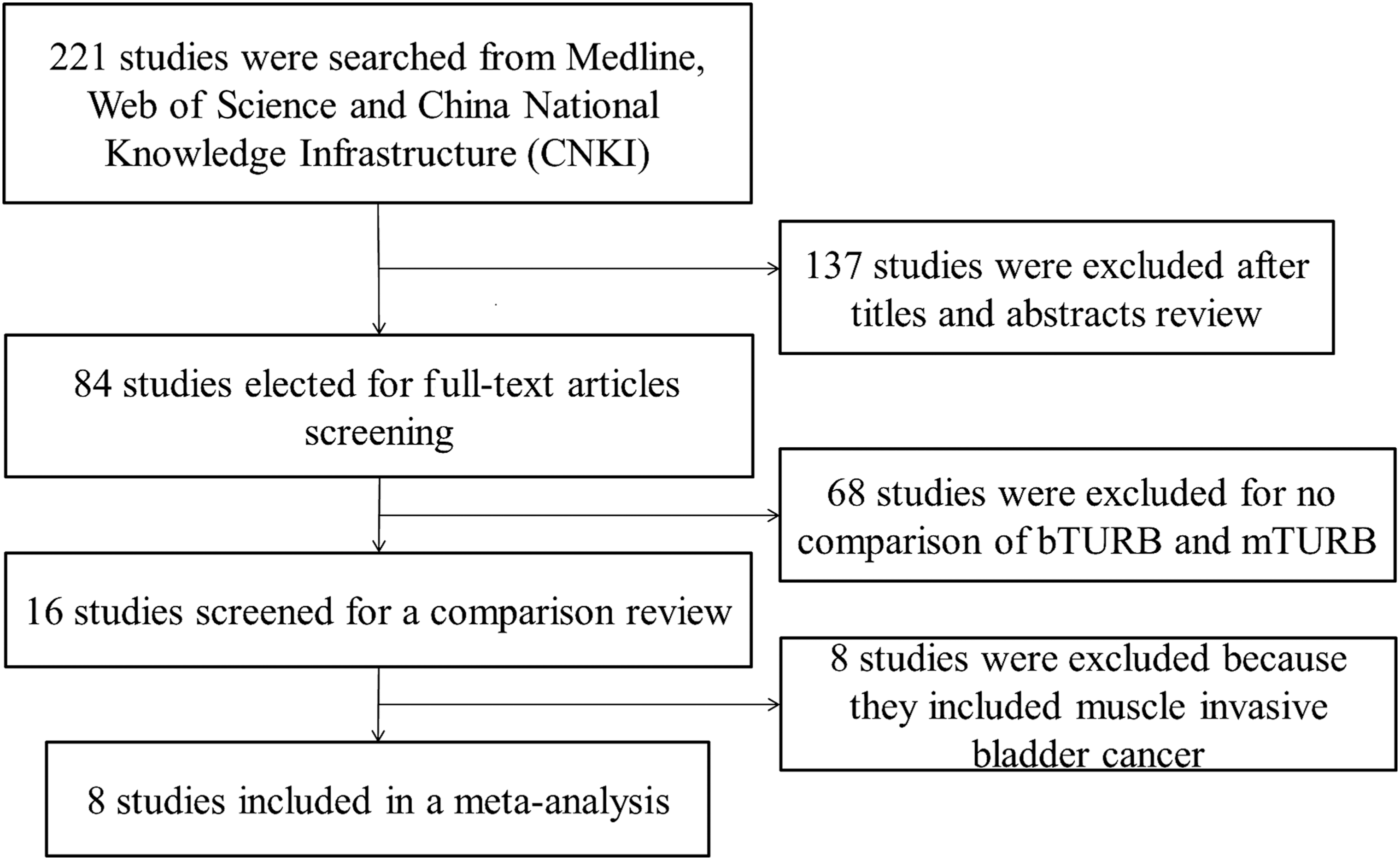
Flowchart showing the selection of studies for meta-analysis.
Based on US Preventive Services Task Force grading system.
Matching/comparable variables: 1 = age, 2 = gender, 3 = tumor size, 4 = tumor stage, 5 = tumor number, 6 = previous surgical procedure.
LOE = level of evidence; TURB = transurethral resection of the bladder; mTURB = monopolar TURB; bTURB = bipolar TURB; RCT = randomized control trial; NA = data not available.
Outcomes of demographic and clinical characteristics
There was no significant difference with respect to age, proportion of males, tumor size, tumor stage, previous surgery, and proportion of multiple tumors between the bTURB and mTURB groups; the results are shown in Table 2.
Values of WMD.
OR = odds ratio; WMD = weighted mean difference; CI = confidence interval.
Outcomes of perioperative variables
The bTURB was associated with shorter operative time (WMD: −2.19; 95% CI: −3.56 to −0.28; P = 0.002) (Fig. 2), shorter hospital stay (WMD: −1.38; 95% CI: −1.60 to −1.15; P < 0.001) (Fig. 3), and shorter catheterization time (WMD: −0.76; 95% CI: −1.27 to −0.25; P = 0.004) (Fig. 4). There was less established blood loss (WMD: −17.56; 95% CI: −24.85 to −10.28; P < 0.001) (Fig. 5) and less drop in hemoglobin level (WMD: −0.55; 95% CI: −0.84 to −0.26; P < 0.001) in the bTURB group. The cases of terminal damage causing histopathologic artifacts were fewer in the bTURB group (OR: 0.32; 95% CI: 0.11–0.88; P = 0.03). There was no significant difference in transfusion rate between the two groups (OR: 0.26; 95% CI: 0.04–1.60; P = 0.15). These results are shown in Table 3.

Forest plot and meta-analysis of operative time (minutes). bTURB = bipolar transurethral resection of the bladder; mTURB = monopolar transurethral resection of the bladder; SD = standard deviation; CI = confidence interval.

Forest plot and meta-analysis of postoperative hospital stay (days).

Forest plot and meta-analysis of catheterization time (days).

Forest plot and meta-analysis of estimated blood loss (mL).
Values of WMD.
Statistically significant values are shown in bold.
Outcomes of complications and postoperative 2-year recurrence rate
We pooled data on complications from the included studies. The most common complications were obturator nerve reflex reported in seven studies 8,10 –15 and bladder perforation reported in five studies 8 –10,12,14 ; other complications such as bleeding 10 and TUR syndrome 12 were only reported in one study, respectively. The bTURB was associated with fewer cases of obturator nerve reflex (OR: 0.22; 95% CI: 0.12–0.40; P < 0.001) (Fig. 6) and bladder perforation (OR: 0.16; 95% CI:0.05–0.55; P = 0.003) (Fig. 7). The 2-year postoperative recurrence rate was also lower in the bTURB group (OR: 0.63; 95% CI:0.41–0.99; P = 0.04) (Fig. 8). These results are shown in Table 4.

Forest plot and meta-analysis of obturator nerve reflex rate.
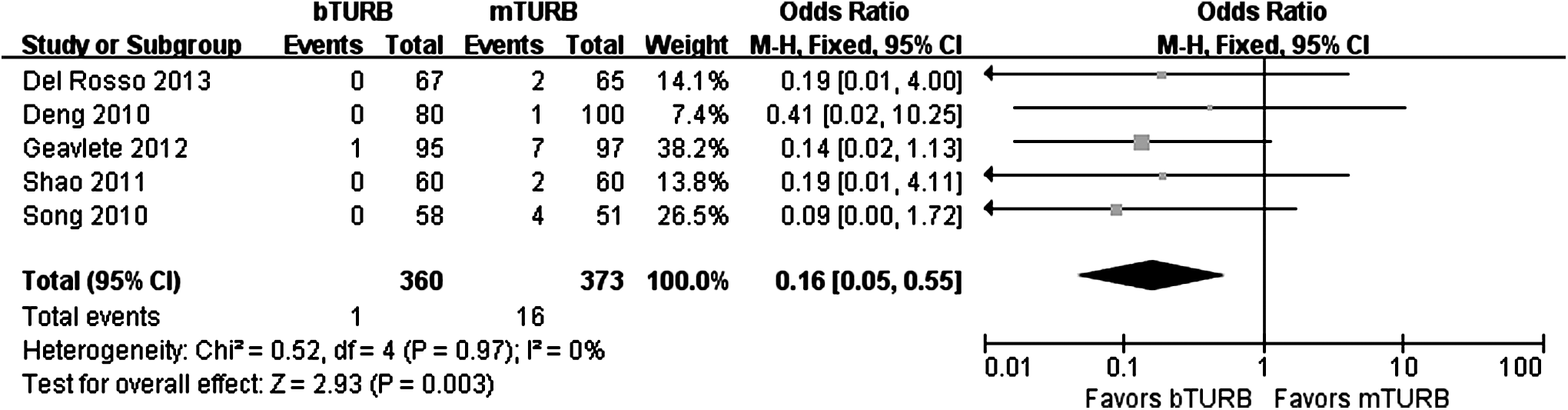
Forest plot and meta-analysis of bladder perforation rate.

Forest plot and meta-analysis of bladder cancer postoperative 2-year recurrence rate.
Statistically significant values are shown in bold.
Sensitivity analysis and publication bias
Sensitivity analysis was performed by removing one certain study each time. The results showed when the study of Del Rosso and colleagues 8 was omitted, the result of operative time demonstrated no significant statistical difference between the two groups (OR: −1.26, 95% CI: −2.95 to 0.43, P = 0.14), and when the study of Li 11 was omitted, there was no significant difference in the 2-year recurrence rate between the two groups (OR: 0.77, 95% CI: 0.48–1.23, P = 0.27). No other significance of the pooled comparison between the two groups was influenced by removing any single study, indicating that the results of our meta-analysis were stable.
Funnel plots were used to assess the publication bias of included studies. Significant publication bias only existed in the comparisons of hospital stay and catheterization time in this presented analysis.
Discussion
Since Beer 21 first reported, TURB remains the standard of diagnosis and initial management of bladder tumor. With the development of bipolar and laser resection techniques, new methods were introduced in the management of TURB as alternatives to conventional mTURB. Different from the monopolar electrocautery resecting loop, plasmakinetic bipolar resection is performed with isotonic saline for irrigation instead of the hypotonic glycine, sorbitol, or mannitol, which helps to avoid TUR syndrome. 22,23 Furthermore, in mTURB, electrical energy is directed into the tissues, where its electrical resistance creates a temperature higher than 300°C.
In bipolar systems, however, the radiofrequency energy converts the conductive medium into a plasma field of highly ionized particles disrupting the organic molecular bonds between the tissues at a much lower temperature as 40°C to 70°C, which may reduce the thermal damage to the surrounding tissues. 7,8,15,22,24,25 In addition, bTURB is much safer for high-risk patients with bladder tumor, such as those with implanted pacemakers or pregnant women. 26
Based on these advantages, bTURB is theoretically safer, and in our meta-analysis and some other studies 16,17 it showed favorable results compared with mTURB for the management of bladder tumor.
Our meta-analysis pooled the data of eight trials from four countries. Compared with other single studies, we revealed more significant differences between bTURB and mTURB in terms of safety and efficacy. The results showed very good baseline characteristics with no significant difference regarding age, sex, the size, number and stage of tumor between the mTURB group and the bTURB group, which would influence the perioperative and postoperative parameters. The bTURB seemed to have a more precise cutting and more reliable hemostasis ability, resulting in shorter operative time, shorter hospital stay, less bleeding, less terminal damage, short catheterization period, and fewer complications such as obturator nerve reflex and bladder perforation.
The most common complication during TURB is bleeding 27 ; bTURB was associated with less established blood loss and a smaller drop in hemoglobin level, indicating that bTURB possesses a better property of hemostasis. There was no significant difference in transfusion rate between mTURB and bTURB. A population-based comparison study in Japan also showed that there was a similar incidence of postoperative hemostasis procedures and transfusion in both groups. 17 Bleeding is not a severe risk factor during TURB to the clinician of the day, and the difference of established blood loss between the two groups seems to be clinically irrelevant. The bTURB, however, provides a bloodless operation field, which can lead to the improvement of tumor clearance and decrease in occurrence of complications.
Our meta-analysis concluded that the incidence rate of bladder perforation was significantly lower in bTURB, which none of the other single studies pointed out. Bladder perforation is a severe complication in TURB, which not only increases the risk of bleeding, but also carries the potential risk for tumor seeding outside the bladder into the extra- or intraperitoneal cavities. Aggressive, deep resection or obturator nerve reflex that results in violent adduction of the leg during the resection may cause the injury or even perforation of the bladder wall. 28 Although the success rate of the obturator nerve block to prevent adductor muscle contractions during TURB is more than 90%, 29 it is still unavailable to avoid the occurrence of obturator nerve reflex completely, especially when the tumor is located on the lateral bladder wall.
The energy of plasmakinetic bipolar resection is confined within smaller depth of the contact surface, and when saline irrigation is used during the bTURB procedure, no current can pass through the body 7 ; hence, the risk of obturator nerve stimulation is significantly reduced. Consequently, the incidence of bladder perforation is also decreased in bTURB.
In our meta-analysis, however, only the trials for the treatment of NMIBC were pooled. In the study of Venkatramani and coworkers, 16 which included patients with invasive bladder cancer, the cutting energy and depth must be increased for satisfactory resection, and without any muscle relaxation or obturator block during the resection procedures, the occurrence rate of bladder perforation and obturator nerve reflex were 16.7% versus 16% and 60% versus 46.2% in the bTURB and mTURB groups, respectively. 16 Therefore, although bipolar energy is associated with a more precise and safer cutting property, standard precautions are necessary to prevent obturator jerk and bladder perforation, especially when the cancer is invasive.
Only one case of TUR syndrome was reported in the trials included in our meta-analysis in mTURB group 12 ; no patients who underwent bTURB had TUR syndrome, and the serum sodium was decreased more in the mTURB group according to the study of Del Rosso and colleagues. 8 Because of the low incidence of this complication in TURB, studies with a large sample size will be necessary to prove statistical significance. In cases of larger, invasive or multiple bladder cancer, which requires higher ablative energy and longer procedures that have been proposed as risk factors of TUR syndrome, bipolar energy is much safer than monopolar. 5,16
The lower occurrence rate of complications in bTURB can help to shorten the perioperative and postoperative recovery period such as hospital stay and catheterization time. The procedures of TURB were not performed in the same way in different countries. For example, in some countries, such as the United States, most TURBs are performed as outpatient procedures, 13 so the problem of hospital stay does not exist. Postoperative rehabilitations in hospital are needed, however, in many places with underdeveloped domestic medicine, and the shorter hospital stay in the bTURB group would be significant.
On the other hand, we found that bipolar loop caused minor terminal damage that altered the histologic architecture. Better preserved resected specimens with fewer cases of severe cautery artifacts were provided by bTURB for pathologic diagnosis. The bTURB can be used not only for the treatment of patients NMIBC, but it also manifested a favorable property to obtain tissues for pathologic confirmation of histologic diagnosis for bladder cancer of all grades and stages. 16,24
The 2-year recurrence rate of bladder cancer was higher in the mTURB group in our meta-analysis. Because bTURB possesses a more accurate cutting ability with lower occurrence of perioperative complications, the blind operation field and the residual lesions may be reduced using bTURB for the management of NMIBC. This result remains questionable, however; our sensitivity analysis of the recurrence rate indicated that this result was not stable, and there was lack of other evidence that supported this conclusion.
There were several limitations in our study. First, only studies published in English and Chinese were pooled in our meta-analysis; some related studies published in other languages might be missed. Second, although the funnel plots only showed publication bias in the comparison of hospital stay and catheterization time, the influence of bias in our study could not be completely excluded. Third, the sample size of some studies included in the analysis is small, so that the statistical power to detect the difference in the outcomes is limited. Fourth, some of our results comparing mTURB and bTURB were only significantly different by statistical analysis, but revealed limited clinical significance, such as differences in operative time of a few minutes and catheterization time of about 1 day.
Last, we only included studies comparing bTURB and mTURB for the treatment of patients with NMIBC; some studies including patients with bladder cancer in a stage more than T2 were excluded. 16,17,24 In fact, TURB is also widely used for bladder cancer in all grades and stages, not only for treatment but also for diagnosis. A more precise study could be performed if more detailed data such as tumor location, tumor size, pathologic stage and grade were available.
Conclusion
Our meta-analysis demonstrated the efficiency and safety of bTURB in the treatment of patients with NMIBC. We compared bTURB and mTURB on the perioperative and postoperative outcomes based on eight trials; the results indicated that bTURB advanced over mTURB in operative time, hospital stay, catheterization period, terminal artifacts, bleeding, complications, and recurrence rate. Our meta-analysis strongly confirmed that bTURB possesses various advantages over mTURB. As a beneficial surgical method for patients with NMIBC, bTURB may be used as a preferable substitute for conventional mTURB.
Footnotes
Author Disclosure Statement
No competing financial interests exist.