
Abstract
Objective:
To evaluate the impact of rectal balloon (RB) inflation on post-transurethral resection of the prostate (TURP) bleeding in patients with symptomatic benign prostatic hyperplasia.
Methods:
After institutional review board approval, patients who were eligible for TURP were randomized into two equal groups, depending on whether they received postoperative endorectal balloon (RB) (GII) or not (GI). The tip of three-way Foley catheter was fixed to a balloon by a blaster strip to prepare air-tight RB. Postoperatively, the RB was inflated for 15 minutes by a pressure-controlled sphygmomanometer. Perioperative data were compared between both groups, including hemoglobin (Hb) deficit 24-hour postoperatively and at time of discharge. Functional outcomes, anorectal complaints, and adverse events were assessed perioperatively and after 1 and 3 months.
Results:
Fifty patients were enrolled, including 13 (26%) patients who presented with indwelling urethral catheters. Baseline data and mean resected tissue weight were comparable between both groups, including preoperative Hb (p = 0.17). Immediate postoperative Hb deficit was, comparable between GI and GII patients (0.58 ± 0.18 vs 0.60 ± 0.2, p = 0.56) before RB inflation, respectively. However, compared to GI patients, mean Hb deficit significantly decreased in GII patients 24-hour postoperatively (0.2 ± 0.2 vs 0.7 ± 0.3 g, p = 0.002) and at time of discharge (0.8 ± 0.2 vs 1.3 ± 0.4 g, p = 0.003). GII patients needed significantly less postoperative irrigation (2.1 ± 1.6 vs 8.3 ± 1.8 L, p < 0.001), shorter catheterization time (2.3 ± 0.8 vs 3.8 ± 1.3 days, p < 0.001), and shorter hospital stay (2.6 ± 0.5 vs 4.3 ± 1.0 days, p < 0.001). Both groups were comparable in all functional outcomes at the most recent follow-up. Blood transfusion was needed in only one patient (4%) in GI. No patient needed recystoscopy for hematuria or clot retention in either group, while there were no anorectal complaints reported by GII patients.
Conclusions:
Post-TURP endorectal balloon inflation seems to be simple, safe, and an efficient procedure to reduce postoperative bleeding and irrigation volume. It is significantly associated with shorter catheterization time and hospital stay.
Introduction
T
Furthermore, post-TURP complications decreased from 18% to as low as 5.8% in multicenter studies, 8 including transfusion rate, post-TURP syndrome, clot retention, urinary-tract infection, and failure to void. 2,3 However, bleeding that necessitates blood transfusion is still one of the most distressing complications of TURP, especially with larger glands, prolonged resection time, or presence of infection or retention. 2,4 Therefore, many techniques were described to decrease blood loss during and after TURP, depending on the pressure provided by the catheter balloon on the prostatic fossa or within the urinary bladder, associated with catheter-applied traction. 2,6,9 Moreover, suprapubic catheters have been used during TURP to decrease the irrigation flow pressure and consequently, decreasing blood loss. 10 In addition, 5α-reductase inhibitors were recommended for 4 to 6 weeks before surgery to decrease bleeding. 11,12 Rectal digital compression for 5 to 10 minutes was also used to control postoperative bleeding. 2,4,13 Pre- and post-TURP injection of cyproterone acetate was recently used to reduce perioperative blood loss. 14 In patients with uncontrolled post-TURP bleeding, open prostate temporary packing has been advised to control bleeding. 15
We previously reported our experience in using a new technique to control postoperative blood loss; the rectal balloon (RB) during open simple prostatectomy with convenient promising results in decreasing postoperative blood loss. 16 Therefore, the aim of the present study was to assess the feasibility, effectiveness, and safety of RB inflation on post-TURP blood loss. We hypothesize that RB would similarly decrease postoperative bleeding through compression of the blood vessels of the prostatic capsule from within the rectum.
Materials and Methods
Patients' enrollment
This study was approved by the institutional ethics committee and all patients provided written informed consents. Patients presented with lower urinary tract symptoms (LUTS) secondary to BPH eligible for TURP and with prostate volume of ≤80 cc by transrectal ultrasound (TRUS) were invited to participate in this pilot study. Exclusion criteria were the use of 5α-reductase inhibitor within the previous 6 months, bladder stones, proven prostate cancer, abnormal bleeding profile from concomitant coagulopathy or blood thinners, which could not withhold prior and during surgery, and/or presence or history of anorectal pathology or surgery.
Patients were prospectively enrolled and randomized between October 2012 and September 2013 into two equal groups, depending on whether they would have postoperative RB (GII) or not (GI). Randomization was performed in the operative room and immediately after finishing the TURP completely to blind the surgeon about the possibility of RB insertion in any patient. The stratified block randomization method was used to distribute prostate size equally between both groups. Baseline data included clinical evaluation, prostate volume determined by TRUS, international prostate symptom score (IPSS), peak flow rate (Qmax), measurement of postvoiding residual urine volume (PVR) by ultrasound, and prostatic-specific antigen (PSA). Complete blood counts, including hemoglobin (Hb) and hematocrit levels, were performed immediately preoperatively (samples were taken in the operating room), immediately after surgery (to assess intraoperative blood loss), 24-hour postoperatively, and at the time of discharge.
Procedure
All patients were operated by well-trained attending urologists, who used the same Mauermayer technique, using a 26F continuous flow resectoscope and monopolar high-frequency current under spinal anesthesia. 2,4,17 At the end of the procedure, all patients underwent three-way 22F urethral Foley catheters where the balloons were inflated with 20 cc more than the resected tissue volume. Catheter traction was applied and continuous bladder irrigation was followed for GI patients, who were transferred to the ward, while GII patients had RB inflation after urethral catheter insertion followed by traction on the urethral catheter thereafter. The RB has been assembled by positioning the tip of a three-way Foley catheter in a medium sized balloon (5 × 7 cm) and fixed by a blaster strip to make it airtight (Fig. 1). RB is inserted in the rectum opposing the prostate, above the anal sphincter (Fig. 2 and 3). The catheter was inflated with a connected sphygmomanometer pump through its small channel, while the sphygmomanometer mercury storage was connected to the catheter large channel to measure the pressure during balloon inflation in the rectum. 16
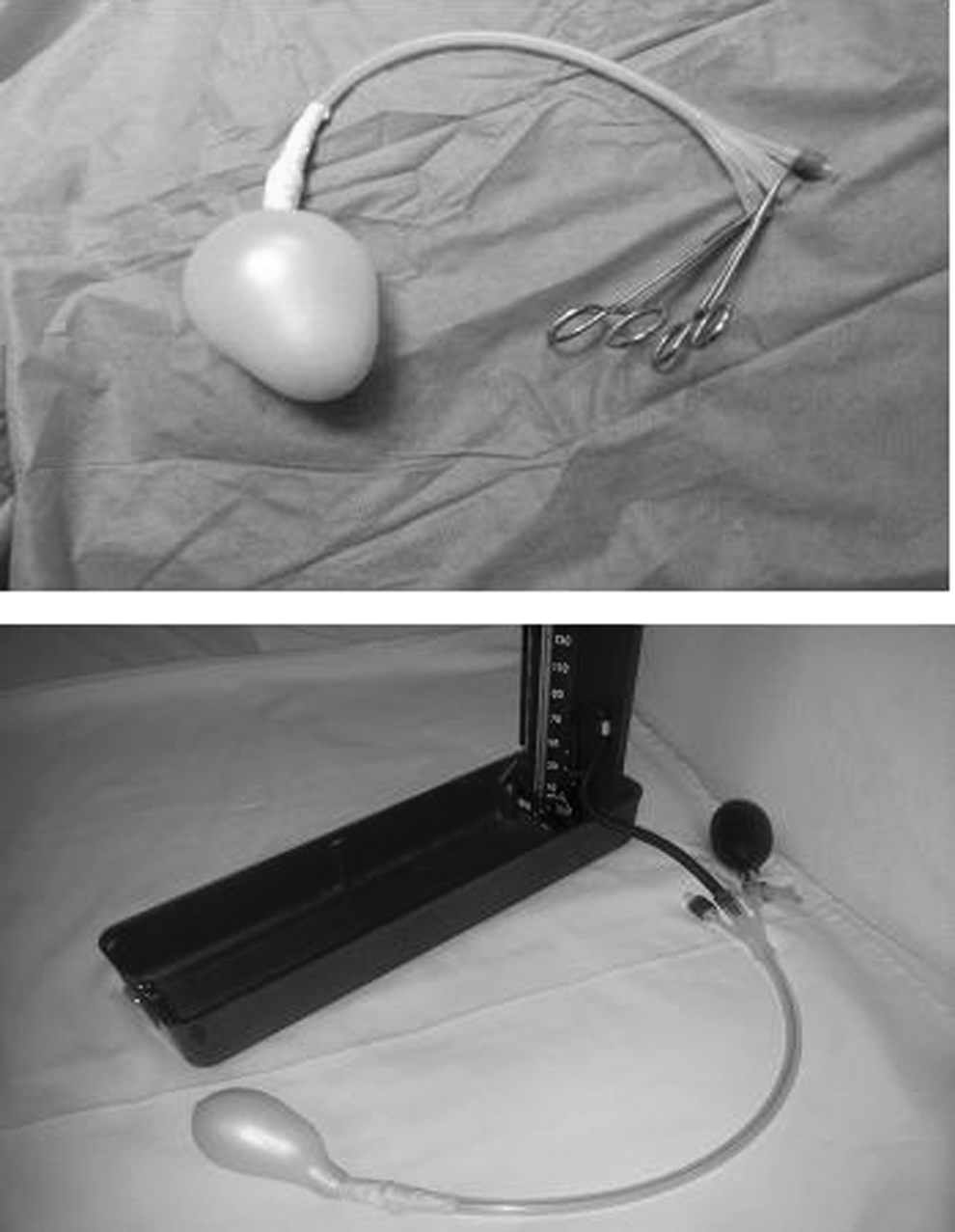
Illustration of the rectal balloon (RB) and its attachment to the sphygmomanometer.
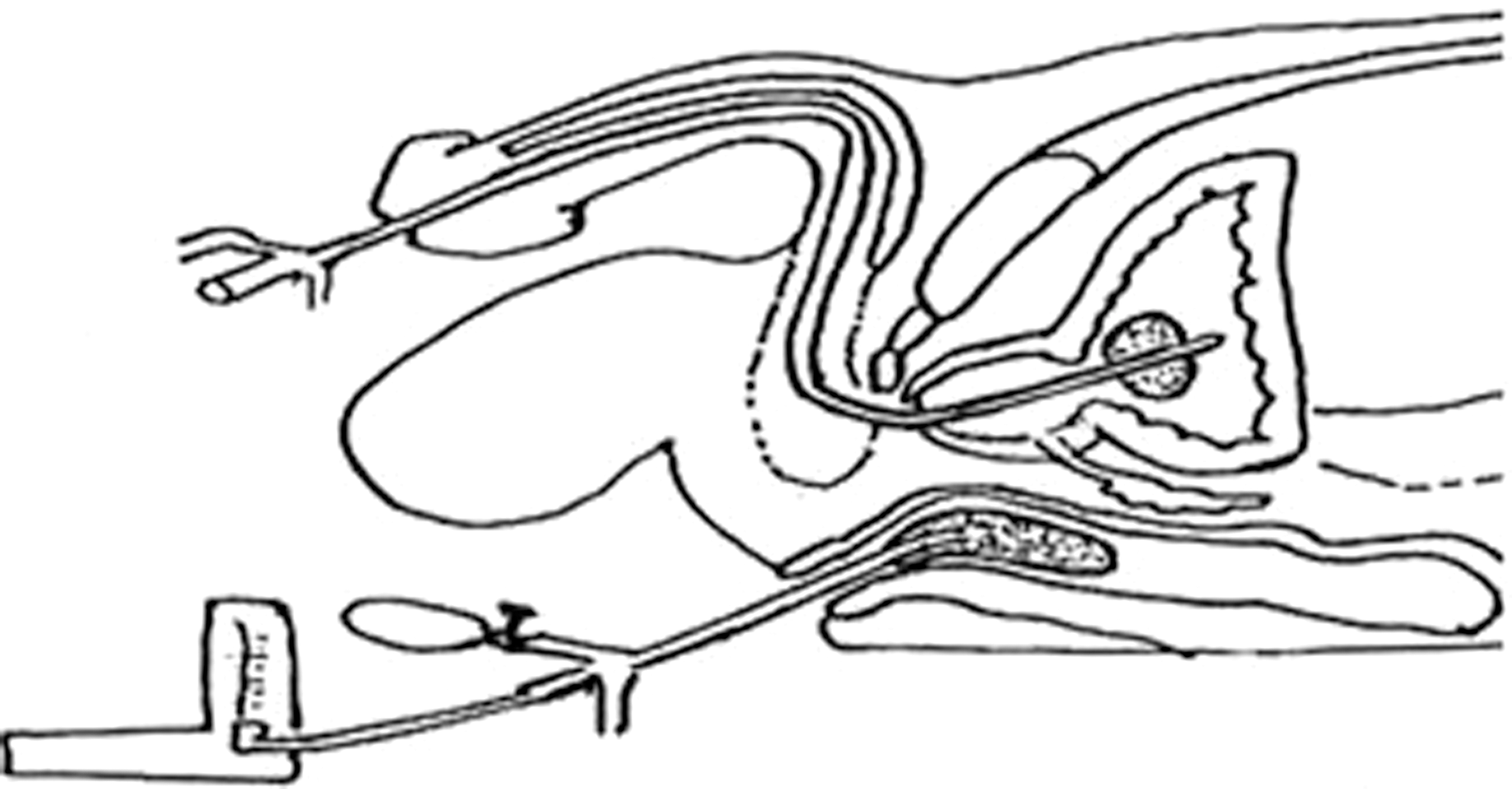
Diagram represents the positioning of the RB in the rectum.
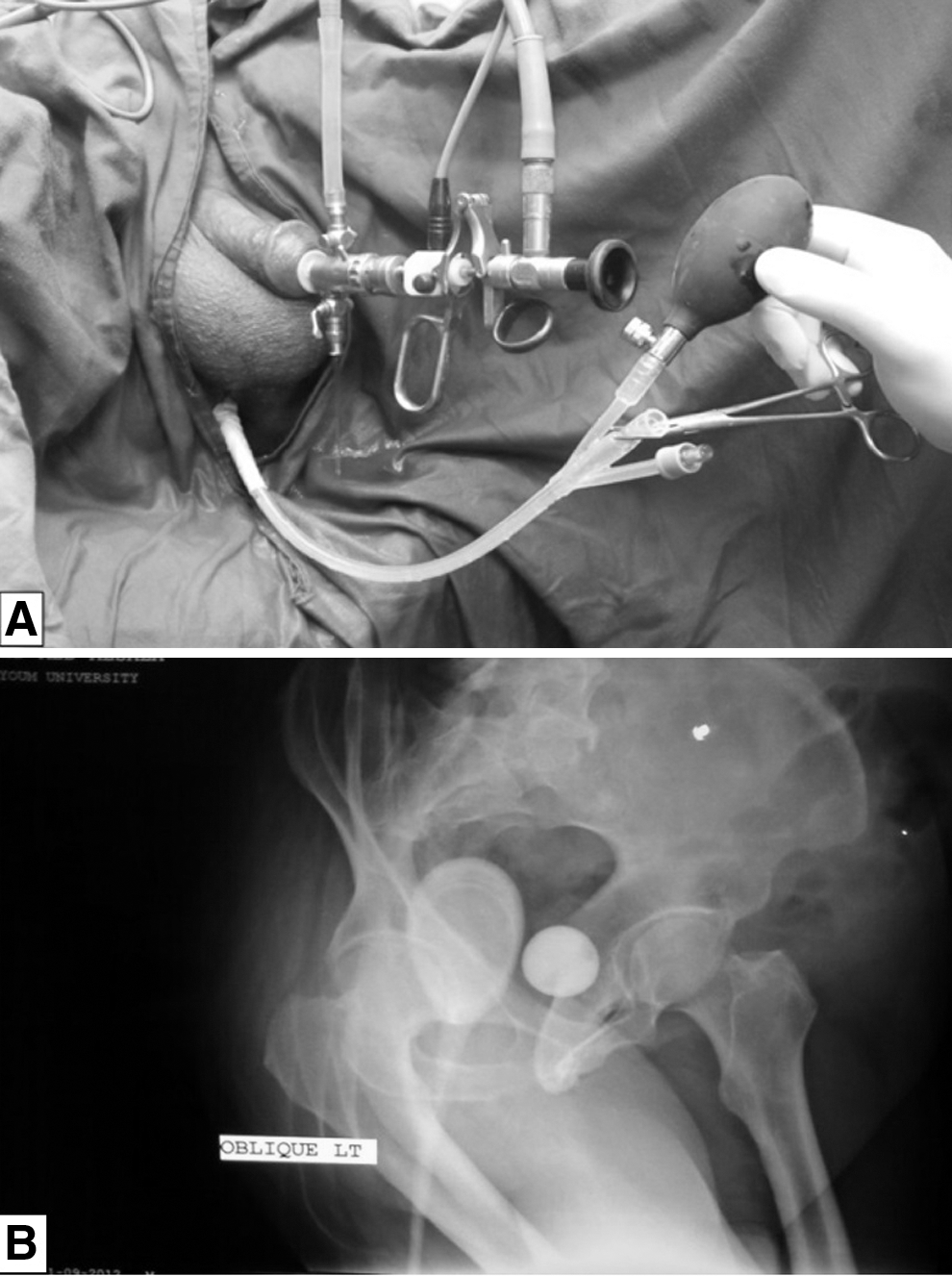
Positioning of the RB in the rectum and its inflation at the end of transurethral resection of the prostate
RB was inflated to pressure less than the systolic pressure and above the diastolic of the patient for 15 minutes to avoid pressure necrosis on the rectal wall, after which it was deflated and removed from the rectum. The anal sphincter was then inspected for any obvious injuries. The urethral catheter was removed when the urine became clear, and the patient was discharged home without catheter when he was able to void satisfactorily. Operative time, resected tissue weight, and amount of saline used for irrigation were calculated for each patient. Catheter duration and the length of hospital stay were documented. One and 3 months postoperatively, patients were followed up with clinical evaluation, IPSS, Qmax, and PVR, whereas PSA was performed at the 3-month visit. GII patients were asked at the first follow-up visit about postoperative adverse events, including rectal complaints, bleeding per rectum, tenesmus, or pain, at the anal verge.
Study outcomes
The primary outcome of the study was to compare the amount of Hb deficit in both groups, in comparison to the baseline values. The secondary outcomes included the assessment of the safety of the post-TURP inflation of RB and to compare the functional outcomes between both groups at different follow-up times.
Statistical analyses
Data analyses were performed using the commercially available Statistical Package for the Social Sciences (SPSS), where continuous variables were tested for normality and equality of variances using the Shapiro–Wilk W-test and Levene F-test, respectively. Descriptive data were presented in terms of numbers and percentages or mean (SD)/median (range), whichever is appropriate. Student's t-test and Fisher's exact test were used to compare continuous and categorical variables, respectively, with accepted critical p-value of ≤ 0.05 for statistically significant differences. Sample size was calculated to detect a Hb deficit of 0.8 ± 02 g between both groups 16 with type I error (alpha) set at 0.05 (two-tailed) and type II error (beta) set at 0.2 (power of 80%). This yielded a projected overall sample size of 50 patients (25 per each group).
Results
Fifty patients were included in the final statistical analysis, including 13 (26%) patients who presented with indwelling urethral catheter secondary to acute urine retention, 7 patients (28%) in GI and 6 patients (24%) in GII (p = 0.327). The demographic and baseline criteria were comparable between both groups (Table 1).
Data are presented in terms of mean ± SD (range).
IPSS=international prostate symptom score; PSA=prostatic-specific antigen; PVR=postvoiding residual urine; Qmax=maximum flow rate.
GII patients had significantly longer operative time (42 vs 58 minutes, p = 0.007) and significantly shorter catheter duration (2.3 ± 0.8 vs 3.8 ± 1.3 days, p < 0.001) and hospital stay (2.6 ± 0.5 vs 4.3 ± 1.0 days, p < 0.001) than GI patients (Table 2). However, GI patients needed significantly more postoperative saline irrigation (8.3 ± 1.8 vs 2.1 ± 1.6 L, p < 0.001) than GII patients.
Data are presented in terms of mean ± SD (range).
Both groups were comparable in baseline Hb (p = 0.17) and intraoperative Hb loss (p = 0.56). However, GII had significantly lower postoperative Hb deficit 24-hour postoperatively (0.2 ± 0.2 vs 0.7 ± 0.3 g, p = 0.002) and at the time of discharge (0.8 ± 0.2 vs 1.3 ± 0.4 g, p = 0.003) in comparison to GI patients (Table 3). The mean resected prostate tissue was comparable, respectively, in GI and GII patients (33 ± 10 vs 34 ± 11 g, p = 0.58).
Data are presented in terms of mean ± SD (range).
Baseline minus immediate postoperative level (g/dL).
Hb=hemoglobin.
All functional outcomes, including IPSS, Qmax, and PVR significantly improved in both groups in comparison to their baseline values. However, they were comparable in both groups at the 3-month follow-up visit in terms of IPSS (5.6 ± 1.2 vs 5.8 ± 1.6, p = 0.62), Qmax (21 ± 2.7 vs 20 ± 2.0, p = 0.14), and PVR (9.4 ± 3.6 vs 11 ± 4.6 mL, p = 0.18) for GI and GII patients, respectively. This yielded respective comparable percent improvement from the baseline of 76.1% vs 74.4% in IPSS, 275% vs 228% in Qmax, and 95.3% vs 93.9% in PVR.
No patient in either group developed post-TUR syndrome, clot retention, or needed recystoscopy for hematuria. Blood transfusion (Clavien Grade II) was only needed in one patient (4%) of GI for excessive intraoperative bleeding, while no patient in GII needed transfusion (p = 1.00). No anorectal adverse events were reported by GII patients resulting from the insertion and/or inflation of the RB. Transient immediate postoperative urinary incontinence (Clavien grade I) was detected in 5 (20%) and 6 (24%) patients of GI and GII, respectively (p = 1.00). However, no patient had urinary incontinence at the 3-month follow-up visit. The histopathology reports for all patients reveal no incidental adenocarcinoma.
Discussion
Continued refinement of instruments and technology resulted in decline in post-TURP adverse events. However, bleeding still remains one of its serious complications, 15 with consequent blood transfusion rates of up to 7.1%. 2,4,15 The impact of balloon compression on the bleeding area has been described in the pressure-controlled Sengstaken–Blakemore tube. The endorectal Foley catheter balloon has been used after TRUS-guided biopsy to control bleeding, but it was not pressure controlled. 17 –19
In the present cohort, all baseline demographic data were comparable between both groups, including the number of patients presented with indwelling urethral catheters. This would not impact postoperative blood loss due to prostate congestion. 2,3 Moreover, the resected tissue weight was consistent with that previously reported after TURP. 1,3,10,20 –23 It would seem intuitive that the operative time was significantly longer in GII patients due to adding the time needed for RB insertion and inflation for hemostasis.
Baseline Hb was also comparable between both groups and the intraoperative bleeding as well, determined by immediate postoperative Hb deficit in both groups. However, patients who underwent postoperative RB insertion had significantly lowered Hb deficit within the first 24 hours and at the time of discharge. This would highlight the hemostatic effect of post-TURP endorectal balloon in compressing the blood vessels of prostatic capsule from within the rectum. Considering post-TURP Hb deficit of up to 3.2 g in some studies, 20,21 this Hb deficit in GII patients seems to be lower than what has been previously reported, even with preoperative use of 5α-reductase inhibitors, 11,20 –23 or when the suprapubic catheter was preoperatively fixed. 10
Furthermore, Hb deficit in the current study was comparable or even lower than that reported with bipolar TURP. 22,24,25 This further supports the compressive effect of the inflated endorectal balloon on the prostatic blood supply. The transfusion rate was 4% in GI patients, which was consistent with that previously reported, 3,20,21 vs 0% in GII. However, this difference was not statistically significant.
It would also seem intuitive that the significantly less blood loss in GII patients was associated with significantly less time and amount of irrigation fluid postoperatively with consequent significant earlier catheter removal by a mean of 1.5 days, shorter hospital stay, and earlier discharge home. Therefore, a significant decrease in the overall cost would be expected for GII patients, including the lower irrigation time and hospital stay costs. The catheterization time of GII patients was lower than previously reported, 1,5,20 and the hospital stay as well. 3,20,21
The objective and subjective functional parameters were significantly improved from the baseline in all patients, while they were comparable between both groups at the most recent follow-up visit, including comparable percent improvement of IPSS (76.1% vs 74.4%), Qmax (275% vs 228%), and PVR (95.3% vs 93.9%) for GI and GII patients, respectively. This was consistent with that previously reported. 3,4,20
The safety of RB insertion and inflation was confirmed by the absence of any anorectal complaints immediately after surgery, at discharge, or even 1-month postoperatively. Moreover, anorectal examination after deflation of the RB at the operative room did not show any local signs of injury or adverse events, which might result from insertion and pressure-controlled inflation of the endorectal balloon. These data support the use of this simple maneuver for decreasing blood loss after TURP, as it is seems to be safe, efficient, and cost-effective. Transient urinary incontinence was comparable between both groups, which usually takes the form of urge incontinence. Fortunately, it improves significantly and progressively postoperatively to be similar to the baseline rates. Adaptation of the bladder and sphincter to the relief of urinary obstruction plays a significant role in such improvement.
Despite being a prospective controlled study, the present cohort represents preliminary data, which does not preclude further multicenter studies to document and improve this technique. Another limitation of the current cohort is the inclusion of prostate glands <80 cc with exclusion of the larger glands, which may have the higher risk of bleeding. However, as a preliminary study to evaluate a new technique, we aimed first to assess its impact on prostate glands <80 cc, which we guess is the standard of care of daily urologic practice in developing countries, where an open simple prostatectomy is still recommended for larger glands. Nevertheless, these promising results encouraged us to use this simple technique currently for a larger gland.
Conclusions
Post-TURP endorectal balloon inflation is a simple, safe, and efficient procedure for patients with small prostate and does not need special operative technique. It seems to reduce the postoperative blood loss, frequency of blood transfusion, postoperative irrigation, and shortens the catheterization time and length of hospital stay. However, this technique is still not universally accepted as the standard of care for a majority of such patients around the world.
Footnotes
Author Disclosure Statement
No competing financial interests exist.