
Abstract
Background:
Upper urinary-tract urothelial carcinomas (UTUC) constitute 5% of urothelial malignancies. Prognostic biomarkers would allow lower risk surgical approaches for less aggressive UTUCs. One biomarker—Ki-67/mindbomb E3 ubiquitin protein ligase 1 (Ki-67/MIB-1)—shows promise in UTUC, but there have been conflicting findings regarding its prognostic role. The systematic review and meta-analysis aim to determine the prognostic value of Ki-67/MIB-1 in UTUC in terms of UTUC-specific mortality rate, 5-year disease-free survival, and 5-year overall survival (including disease-specific survival).
Methods:
A systematic review of the current literature produced 654 records. A total of 13 studies consisting of 1030 patients were finally included in the meta-analysis. Hazard ratios (HRs) with 95% confidence intervals (CI) were extracted or estimated. The individual HR estimates were combined into a pooled HR using a fixed-effects model that summed homogeneity of the individual true HRs.
Results:
Patients with Ki-67/MIB-1 overexpression displayed significantly higher UTUC-specific mortality rate (pooled HR: 2.14, 95% CI: 1.73–2.64; p<0.00001), significantly reduced 5-year disease-free survival (pooled HR: 2.27, 95% CI: 1.79–2.92; p<0.00001), and significantly reduced 5-year overall survival (pooled HR=1.77; 95% CI: 1.39–2.23 p<0.00001). There was significant heterogeneity detected in the UTUC-specific mortality rate meta-analysis (I 2=63%) and the 5-year disease-free survival meta-analysis (I 2=65%), but there was no significant heterogeneity detected in the 5-year overall survival meta-analysis (I 2=0%). Egger's testing showed that none of the outcomes were influenced by publication bias (p>0.05).
Conclusions:
Ki-67/MIB-1 overexpression shows promise as a prognostic biomarker for UTUC patients and requires further investigation.
Introduction
U
However, an accurate risk stratification of UTUC cases remains problematic due to the difficulties inherent in clinical staging. 4 Several potential prognostic factors for UTUC have been previously identified, including the patient's clinical characteristics, pathological parameters, and molecular biomarkers. 4 Specifically, a comprehensive 2012 review of the UTUC literature revealed that changes in several urothelial tissue biomarkers—including p53, Ki-67/MIB-1, Snail, Bcl-2, survivin, and CD24—are associated with both advanced staging and tumor grading. 5 Clinical application of these biomarkers could identify patient candidates for more conservative surgical approaches without significantly compromising their clinical outcomes.
One biomarker in particular–Kiel-67/mindbomb E3 ubiquitin protein ligase 1 (Ki-67/MIB-1)–shows promise in terms of UTUC tumor staging and grading, but there have been conflicting findings regarding its prognostic role. 6 One previous systematic review in 2004 by Moreno et al. sought to investigate the prognostic role of Ki-67/MIB-1 in UTUC patients, but a meta-analysis could not be performed at that time due to the heterogeneity of the studies found. 7 Therefore, the aim of this systematic review and meta-analysis was to determine the prognostic role of Ki-67/MIB-1 in UTUC in terms of UTUC-specific mortality rate, 5-year disease-free survival, and 5-year overall survival (including disease-specific survival).
Methods
Search strategy
We performed a systematic review according to the PRISMA guidelines (
Selection criteria
To limit heterogeneity across studies, 8 strict inclusion and exclusion criteria were applied here. If the same data were reported in more than one article, the article providing the most information was selected to avoid data duplication. Studies were considered for inclusion if they met the following criteria: (i) Ki-67/MIB-1 protein expression was evaluated in human upper urinary tract tissue (including the ureter and renal pelvis); (ii) in situ Ki-67/MIB-1 protein expression was evaluated by immunohistochemistry, fluorescence in situ hybridization (FISH), immunofluorescence, enzyme immunoassay, or Western blotting; (iii) the tumor's histologic type was conclusively determined to be urothelial cell carcinoma (UC, UCC) or transitional-cell carcinoma; and (iv) the association between in situ Ki-67/MIB-1 protein expression levels and survival outcome(s) was measured.
The following exclusion criteria were used: (i) reviews, letters to editorial staff, commentaries, or case reports; (ii) studies on cell lines or animal models; (iii) survival outcome(s) not reported; or (iv) if the hazard ratio (HR) and its standard error could not be calculated based on the reported information (please see “Statistical analysis” section below).
Data extraction
One coauthor extracted data from the included studies, and another coauthor checked the extracted data for accuracy. The following data were extracted from each included study: (i) basic article information (first author's name, publication year, country of study, and study design); (ii) patient characteristics (number of patients per study arm, age, gender proportion [male%, female%]); (iii) treatment modality (e.g., chemotherapy, surgery, radiation); (iv) method of measuring the Ki-67/MIB-1 protein expression (e.g., immunohistochemistry, FISH, immunofluorescence, enzyme immunoassay, or Western blot); and (v) HRs of Ki-67/MIB-1 overexpression for UTUC-specific mortality rate, 5-year disease-free survival, or 5-year overall survival (as well as their 95% confidence intervals (CI) and p-values). For data that could not be extracted, good faith efforts were applied to obtain the data by contacting the author(s) and researching other studies citing the study in question.
Quality assessment
The methodological quality of the included studies was scored according to a previously described eight-point quality scale. 9 Studies with a total score of eight were deemed to be of the highest quality, while studies with a total score of zero were considered to be of the lowest quality. This methodological quality assessment was independently performed by two coauthors, and any disagreement with regard to scoring was resolved by consensus. Studies were also scored as phase I–III according to Simon and Altman's well-established criteria for prognostic marker studies. 10
Statistical analysis
All meta-analyses were performed with Review Manager version 5.0 (RevMan; the Cochrane Collaboration, Copenhagen, Denmark). When provided, HR and 95% CIs for Ki-67/MIB-1 expression were extracted; however, for studies solely reporting the total number of events and the number of at-risk patients in each study arm, previously reported indirect methods were used for extracting the log(HR) and variance. If only Kaplan-Meier curves were available, then data were extracted from the graphic survival plots using Engauge Digitizer version 2.11 (
Heterogeneity testing of combined HRs was performed using I2 with a p-value of less than 0.05 deemed significant. An I2 value above 50% indicated significant heterogeneity. Publication bias was assessed by inspecting the funnel plot–where an asymmetric plot suggests possible publication bias—followed by Egger's testing if needed.
Results
A total of 654 records were initially identified through the literature search (Fig. 1). After removal of duplicate records and strict application of the inclusion and exclusion criteria, 13 studies consisting of 1030 patients were finally included in this meta-analysis. 11 –23 Data extraction was conducted successfully with a mean intraclass correlation between the two independent reviewers of 0.87±0.08.
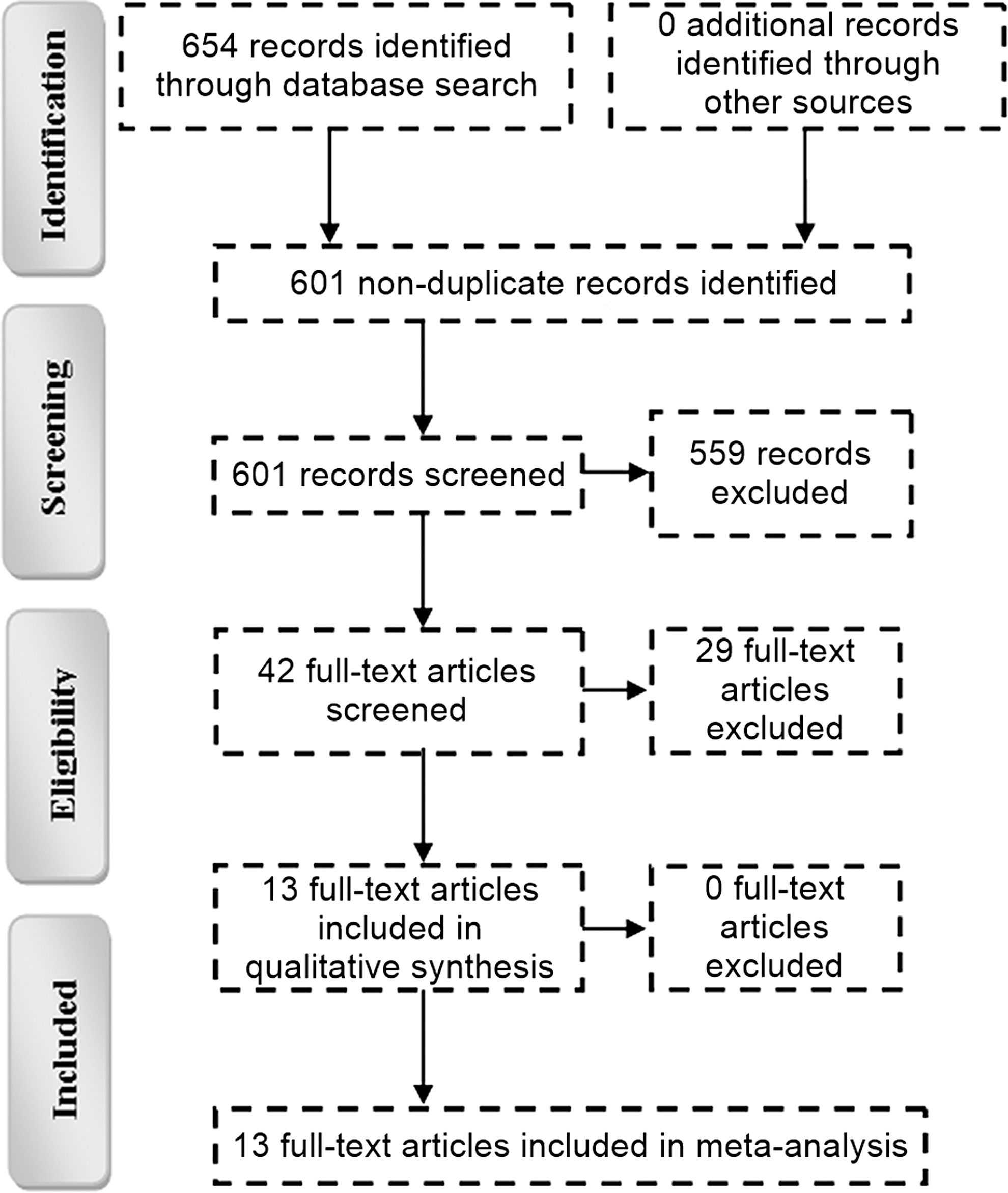
Flow Diagram of Study Selection. Four-phase PRISMA flow-diagram for study collection, showing the number of studies identified, screened, eligible, and included in the review and meta-analysis.
The demographic and clinical characteristics of these 13 studies are detailed in Table 1. The constituent studies were performed on adult patient populations from Western Europe, East Asia, and the United States that had undergone surgery, radiation therapy, or chemotherapy for UTUC. All 13 studies were either phase II or phase III studies and used immunohistochemistry as the means of detecting the Ki-67/MIB-1 expression. Methodological quality assessment on an eight-point quality scale revealed that all 13 studies had a score of five or greater (Table 2). Using data from these 13 studies, three meta-analyses were conducted here: UTUC-specific mortality rate, 5-year disease-free survival, and 5-year overall survival, which are detailed below.
See Table 2.
M = male; F = female; NR = not reported.
Meta-analysis of UTUC-specific mortality rate
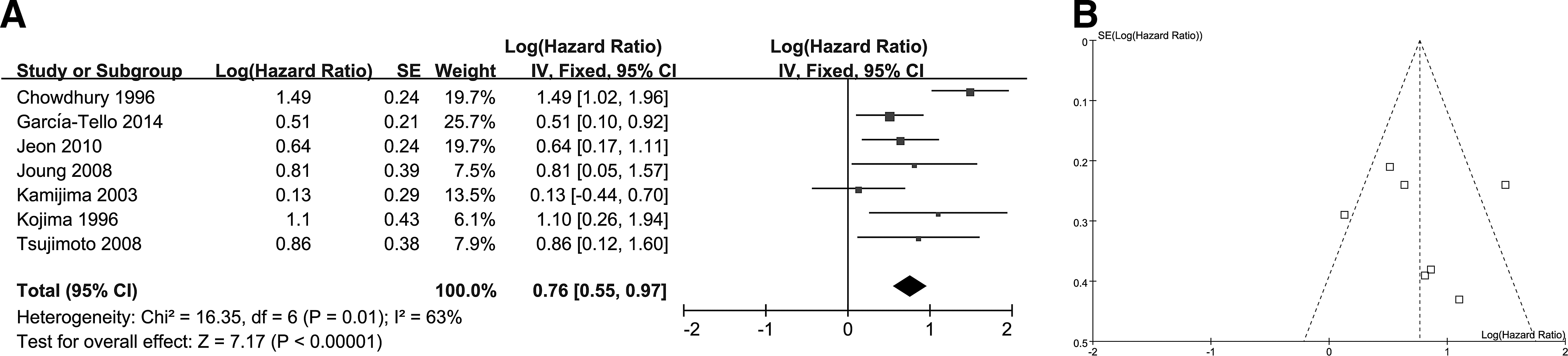
HRs of Ki-67/MIB-1 overexpression for UTUC-specific mortality rate were available for seven studies (Fig. 2A). The pooled log(HR) was 0.76 (95% CI: 0.55–0.97, z=7.17, p<0.00001), which equaled the pooled HR of 2.14 (95% CI: 1.73–2.64). The results indicate that patients with a Ki-67/MIB-1 overexpression display significantly higher UTUC-specific mortality rate.

Meta-Analysis of UTUC-Specific Mortality Rate.
There was significant heterogeneity in the effect size (p=0.01, I 2 =63%). There was no significant asymmetry in the inverted funnel plots of the selected studies (Fig. 2B). Considering the number of selected studies may not have provided sufficient power to show a clear asymmetry, Egger's test was performed. This test showed that the primary outcome (p=0.34) was not influenced by publication bias.
Meta-analysis of 5-year disease-free survival
HRs of Ki-67/MIB-1 overexpression for 5-year disease-free survival were available in four studies (Fig. 3A). The pooled log(HR) was 0.82 (95% CI: 0.58–1.07, z=6.66, p<0.00001), which equaled the pooled HR of 2.27 (95% CI: 1.79–2.92). These results indicate that patients with a Ki-67/MIB-1 overexpression display a significantly reduced 5-year disease-free survival.
Meta-Analysis of 5-Year Disease-Free Survival.
There was significant heterogeneity in the effect size (p=0.04, I 2 =65%). There was no significant asymmetry in the inverted funnel plots of the selected studies (Fig. 3B). Considering the number of selected studies may not have provided sufficient power to show a clear asymmetry, Egger's test was performed. This test showed that the primary outcome (p=0.21) was not influenced by publication bias.
Meta-analysis of 5-year overall survival
HRs of Ki-67/MIB-1 overexpression for overall 5-year survival (including disease-specific survival) were available for seven studies (Fig. 4A). The pooled log(HR) was 0.57 (95% CI: 0.33–0.80, z=4.75, p<0.00001), which equaled the pooled HR of 1.77 (95% CI: 1.39–2.23). The results indicate that patients with a Ki-67/MIB-1 overexpression display a significantly reduced 5-year overall survival.
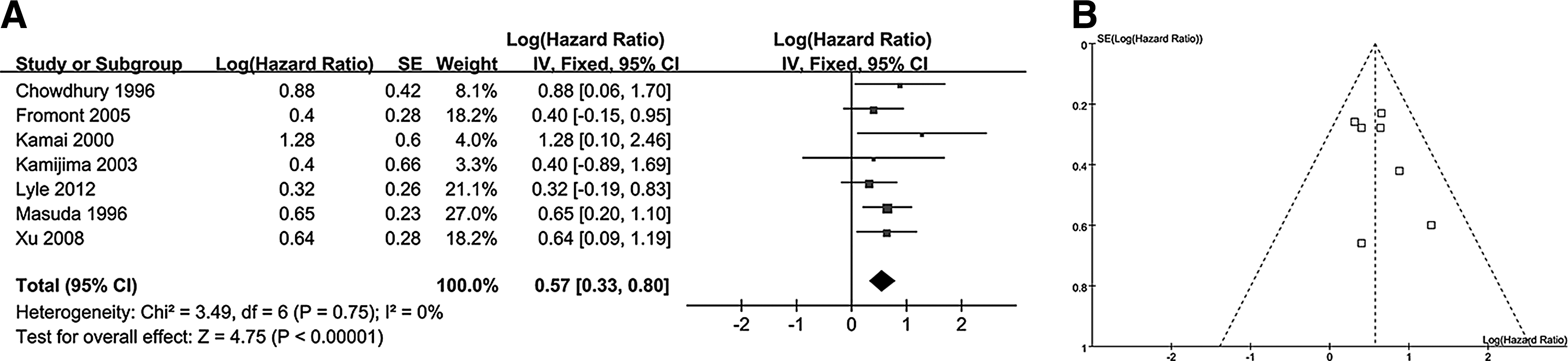
Meta-Analysis of 5-Year Overall Survival.
There was no significant heterogeneity in the effect size (p=0.75, I 2 =0%). There was no significant asymmetry in the inverted funnel plots of the selected studies (Fig. 4B). Considering the number of selected studies may not have provided sufficient power to show a clear asymmetry, Egger's test was performed. This test showed that the primary outcome (p=0.54) was not influenced by publication bias.
Discussion
In this systematic review and meta-analysis, we aimed to determine the prognostic role of Ki-67/MIB-1 in UTUC in terms of UTUC-specific mortality rate, 5-year disease-free survival, and 5-year overall survival. We found that patients with a Ki-67/MIB-1 overexpression displayed significantly higher UTUC-specific mortality rate (pooled HR: 2.14, 95% CI: 1.73–2.64; p<0.00001), significantly reduced 5-year disease-free survival (pooled HR: 2.27, 95% CI: 1.79–2.92; p<0.00001), and significantly reduced 5-year overall survival (pooled HR=1.77; 95% CI: 1.39–2.23 p<0.00001). There was significant heterogeneity detected for the UTUC-specific mortality rate meta-analysis (I 2 =63%) and the 5-year disease-free survival meta-analysis (I 2 =65%), but there was no significant heterogeneity detected for the 5-year overall survival meta-analysis (I 2 =0%). Egger's testing showed that no outcomes were influenced by publication bias (p>0.05).
Ki-67/MIB-1 was initially identified in 1991 as a nuclear nonhistone protein. 24,25 The widespread expression of Ki-67/MIB-1 in proliferating cells and absence in quiescent ones have developed this protein's role as a key cell proliferation marker in laboratory studies. 25 Accordingly, Ki-67/MIB-1 blockage by antibody treatment or inhibiting the protein's dephosphorylation results in arrest of cell proliferation. 25 –28 Not surprisingly, previous evidence has supported the use of Ki-67/MIB-1 as a prognostic marker across a wide variety of human cancers aside from UTUC, including transitional-cell bladder carcinoma, 29 renal-cell carcinoma, 30 breast carcinoma, 31 prostate cancer, 32 cervical cancer, 33 pancreatic adenocarcinoma, 34 nonsmall-cell lung carcinoma, 35 head and neck squamous-cell carcinoma, 36 and soft tissue sarcoma. 37
While Ki-67/MIB-1 is a well-established indicator of cell proliferation and cancer prognosis, its precise mechanism(s) of action remains unknown. That being said, Ki-67/MIB-1 is recognized to play a role in the cell cycle based on its cell cycle-dependent cyclical expression profile—Ki-67/MIB-1 expression levels undulate throughout the cell cycle with a low baseline level during G1 and early S that climaxes at M, followed by a return to baseline. 25,38 Moreover, the cellular localization of Ki-67/MIB-1 varies throughout the cell cycle. 26 The protein is disbursed within the nuclear karyoplasm during early G1 and then accumulates into perinucleolar granules during late G1. 12,25,28,39 Then, during S and G2, the protein localizes to nucleolar and heterochromatin areas, and in early M, Ki-67/MIB-1 localizes to chromosomal surfaces. 12,25,28,39 Although this evidence suggests that Ki-67/MIB-1 plays a role in promoting cell proliferation through its cell cycle-dependent expression profile, nuclear localization, and association with chromatin, further research is needed to elucidate its precise role in cell cycle regulation.
There are several limitations to the current meta-analysis. First, the included studies applied different immunohistochemical cutoff values for Ki-67/MIB-1 overexpression. These differences may be responsible for the difficulty in establishing a universal standard threshold in clinical practice. However, Spyratos et al. have recommended that the immunohistochemical cutoff point should depend on the clinical scenario. For example, a lower cutoff of 10% would avoid overtreatment if Ki-67/MIB-1 is used to exclude patients with slow-growing tumors from chemotherapy. However, if Ki-67/MIB-1 is used to identify chemotherapy-sensitive patients, a higher cutoff of 25% would be advisable. 40 Even though the relative increase in Ki-67/MIB-1 expression is estimated by a baseline risk (the risk in the group considered Ki-67 negative or underexpression), it is not precisely the same in all the included studies, our current findings still reveal that Ki-67/MIB-1 overexpression signals higher UTUC-specific mortality rate as well as reduced 5-year disease-free and overall survival in UTUC patients. Second, this meta-analysis only assesses the univariate prognostic value of Ki-67/MIB-1 in UTUC patients. Therefore, it cannot be inferred from these findings that Ki-67/MIB-1 is an independent prognostic factor for the assessed outcomes; a prospective study is required to make such a determination. Third, there was significant heterogeneity detected for the UTUC-specific mortality rate meta-analysis (I 2 =63%) and the 5-year disease-free survival meta-analysis (I 2 =65%). The use of different Ki-67/MIB-1 cutoff values across the included studies, ethnogenetic and environmental differences across the various geographic regions under study, and regional differences in UTUC treatment protocols and healthcare delivery could explain some of the observed heterogeneity. Moreover, this meta-analysis pooled studies employing a variety of treatment options, including chemotherapy, radiation, and surgery; this may have also contributed to the observed heterogeneity.
Conclusions
Patients with Ki-67/MIB-1 overexpression display significantly higher UTUC-specific mortality rate, significantly reduced 5-year disease-free survival, and significantly reduced 5-year overall survival. Thus, Ki-67/MIB-1 overexpression shows promise as a prognostic biomarker for UTUC patients and requires further clinical investigation.
Author Contributions
Conceived and designed the study: Y.L., Z.L., and M.C. Performed the study: Y.L. Z.L., S.T., and B.L. Analyzed the data: B.L. and W.H. Wrote the artcle: Y.L., L.Q., and M.C.
Footnotes
Acknowledgments
This study was funded by the National Nature Science Foundation for the Youth of China (grant no. 81202005), the Technology Plan Fund of Hunan Science (grant no. 2013FJ4109), and the Central South University Innovation Fund for Independent Graduate Exploration (grant no. 72150050587).
Author Disclosure Statement
The authors declare that they have no conflicts of interest.