
Abstract
Background and Purpose:
The aim of our study was to assess the oncologic outcomes of robot-assisted radical cystectomy (RARC) in patients with bladder cancer (BCa) treated in a high-volume robotic center.
Materials and Methods:
We retrospectively collected data of 155 consecutive patients who received RARC for urothelial BCa from January 2004 to May 2014. Kaplan–Meier analyses were used to assess time to recurrence, cancer-specific mortality (CSM) rate, and overall mortality rate. Uni- and multivariable Cox regression models addressed the predictors of recurrence and CSM.
Results:
Median follow-up for survivors was 42 months. Overall, 43%, 34%, 55%, and 18% of the patients had pT ≤1, pT2, pT3/4, and pN1–3 disease, respectively. Overall, 76% of the patients had high-grade disease at final pathology. The positive surgical margin rate was 9%. The 5-year recurrence-free, CSM-free, and overall survival estimates were 53.7%, 73.5%, and 65.2%, respectively. Among patients who experienced recurrence, 12.0%, 4.0%, and 84.0% had local, peritoneal, and distant recurrence, respectively. In multivariable Cox regression analyses, pathologic stage and nodal status represented independent predictors of recurrence and CSM (all p ≤ 0.04).
Conclusions:
In a high-volume robotic center, RARC provides acceptable oncologic outcomes in patients with urothelial BCa. Tumor stage and nodal status represent independent predictors of recurrence and CSM in this setting.
Introduction
B
Previous studies evaluating the oncologic efficacy of RARC in patients with BCa reported acceptable results. However, others hypothesized that this approach might be associated with an increased risk of pelvic recurrence compared with open surgery. 5 –9 The relatively short-term follow-up and the evaluation of small highly selected cohorts often limit the generalizability of available studies.
Additionally, the inclusion of patients with heterogeneous characteristics coming from several centers across the world might, in part, preclude the applicability of results reported by multi-institutional investigations. 10 Therefore, further studies are needed to comprehensively evaluate the oncologic safety of RARC in patients with BCa. Under this light, we aimed at assessing the recurrence and cancer-specific survival rates in a contemporary cohort of BCa patients treated with RARC at a single referral center by two high-volume surgeons. Moreover, we sought to describe the patterns of recurrence after surgery. Finally, we aimed at determining predictors of recurrence and disease-specific mortality rate in BCa patients treated with the robotic approach.
Materials and Methods
Patient population
We retrospectively extracted from our Institutional database all the 155 consecutive patients who underwent RC for nonmetastatic urothelial BCa at Onze-Lieve-Vrouw Hospital, Aalst, Belgium, from January 2004 to May 2014. Indications for RC were tumor invasion of the muscularis propria, high-grade invasive BCa associated with carcinoma in situ or refractory to intravesical immunotherapy, or recurrent multifocal nonmuscle-invasive BCa refractory to transurethral resection and intravesical therapy.
The surgical technique performed in our center has been previously described 11,12 and consists of ureteral isolation and ligation, retrovesical dissection, development of the rectovesical space, lateral dissection, division of the ovarian pedicles and dissection of the uterine support (in female), identification and isolation of the bladder pedicles, vaginal dissection (in female), anterior dissection, incision of the endopelvic fascia, incision of the dorsal venous complex and apical dissection (in male), transection of the urethra, and reconstruction of the vagina (in female). An anatomically defined extended pelvic lymph node dissection that included common, external, and internal iliac, presacral, and obturator nodes was performed according to the clinical judgment of the treating physician on the bases of disease characteristics and comorbidity status. 2,11 RARC was performed by two high-volume surgeons. One surgeon performed all the diversions extracorporeally. The second surgeon started performing intracorporeal diversion in selected cases in 2005 and performed exclusively intracorporeal diversion since 2007, adopting the surgical technique described by the Karolinska Institutet. 13 Neoadjuvant chemotherapy was selectively adopted, according to the treating physicians' preference.
Covariates
Clinical stage was based on the histological report of the transurethral resection specimen, chest X-rays, and abdominal CT. Concomitant upper urinary tract urothelial carcinoma was evaluated by excretory urography or abdominal CT. Bone scans and brain CT were performed when suggested by signs and symptoms. Patient comorbidity was assessed by the Charlson comorbidity index (CCI). 14 Clinical and pathological staging was reported according to the 2002 TNM system. The WHO 1998 classification was used to assign histological tumor grade. 15
Follow-up and outcome parameters
Patients were evaluated 2 months after discharge and then at least every 4 months for the first year, semiannually for the second year, and annually thereafter. Follow-up visits consisted of a physical examination, serum chemistry evaluation, and diagnostic imaging. Abdominal and chest imaging was performed at least annually or when clinically indicated. Additional radiographic evaluations were performed at the discretion of the treating physician. Primary outcome measures consisted of recurrence-free survival, cancer-specific mortality (CSM)-free survival, and overall survival. Recurrence-free survival was defined as time from surgery to local and/or metastatic recurrence based on histologic and/or radiologic evidence. Local recurrence was defined as evidence of disease in the true pelvis. Systemic recurrence was defined as evidence of metastatic disease outside the pelvis. CSM was defined as death from BCa. Overall mortality (OM) rate was defined as death due to any causes.
Statistical analyses
Medians and interquartile ranges (IQRs) were reported for non-normally distributed continuous variables. Frequencies and proportions were reported for categorical variables. The chi-square test was used to compare proportions between groups. Kaplan–Meier analyses were used to assess time to recurrence and CSM in the overall population and after stratifying patients according to pathological stage, nodal stage, and surgical margins. Separate Kaplan–Meier analyses were performed to assess time to CSM and OM after stratifying patients according to the site of recurrence (no recurrence vs local vs peritoneal vs distant recurrence). Uni- and multivariable Cox regression analyses addressed the predictors of recurrence, CSM, and OM. Covariates consisted of age, CCI, pathologic stage (pT ≤1 vs pT2 vs pT3/4), nodal stage (pNx vs pN0 vs pN1–3), number of nodes removed, pathologic grade, lymphovascular invasion, surgical margins, and the administration of neoadjuvant/adjuvant treatments.
All statistical tests were performed using the R statistical package v.3.0.2 (R Project for Statistical Computing,
Results
Baseline and perioperative characteristics
Table 1 depicts the demographic, preoperative, perioperative, and pathologic characteristics of patients included in the study. Median (IQR) age at surgery was 70 (61–77) years. Overall, 101 (65%) patients underwent cystectomy for muscle-invasive BCa. Overall, 32 (21%) patients received neoadjuvant chemotherapy. The majority of the patients included in our cohort received an ileal conduit (n = 132; 85.2%). The type of diversion was intracorporeal and extracorporeal in 105 (67.7%) and 50 (32.3%) patients, respectively.
BCa = bladder cancer; CCI = Charlson comorbidity index; IQR = interquartile range; PLND = pelvic lymph node dissection; RARC = robot-assisted radical cystectomy; ASA = American Society of Anesthesiologists; BMI = body mass index; TUR = transurethral resection.
Pathologic characteristics
Overall, 66 (43%), 32 (22%), 55 (35%), and 28 (18%) patients had pT ≤1, pT2, pT3/4, and pN1–3 disease, respectively. When a lymph node dissection was performed, the median (IQR) number of nodes removed was 11 (6–17). The majority of the patients included in the study had high-grade disease (n = 118; 76%). Overall, the positive surgical margin rate was 9%. When patients were stratified according to the pathologic stage, men with pT3/4 disease had significantly higher positive margin rates compared with their counterparts with pT ≤1 and pT2 disease (20.0% vs 3.0% vs 2.9%, respectively; p < 0.001).
Survival analyses
The median (IQR) follow-up for survivors was 42 (33.2–50.7) months. Overall, 59, 28, and 51 patients experienced recurrence, CSM, and OM, respectively. The 5-year recurrence-, CSM-free, and overall survival rates were 53.7%, 73.5%, and 59.2%, respectively (Figs. 1a, 2a, and 3). Among patients who experienced recurrence, 12.0%, 4.0%, and 84.0% had local, peritoneal, and distant recurrence, respectively. When patients were stratified according to the pathologic stage, significant differences were observed in 5-year recurrence- and CSM-free survival rates (73.2% and 87.4% vs 48.8% and 70.8% vs 33.6% and 58.6% for pT ≤1 vs pT2 vs pT3/4 disease, respectively; p < 0.001; Figs. 1b and 2b). When patients were stratified according to the nodal stage, those with pN1–3 disease had lower 5-year recurrence- and CSM-free survival rates compared with their counterparts with pNx/0 (15.7% and 42.2% vs 60.4% and 79.3%, respectively; p < 0.001; Figs. 1c and 2c). No significant differences were observed in 5-year recurrence- and CSM-free survival rates when patients were stratified according to the margin status (all p ≥ 0.3; Figs. 1d and 2d). Supplementary Figures S1 and S2 (Supplementary Data are available online at
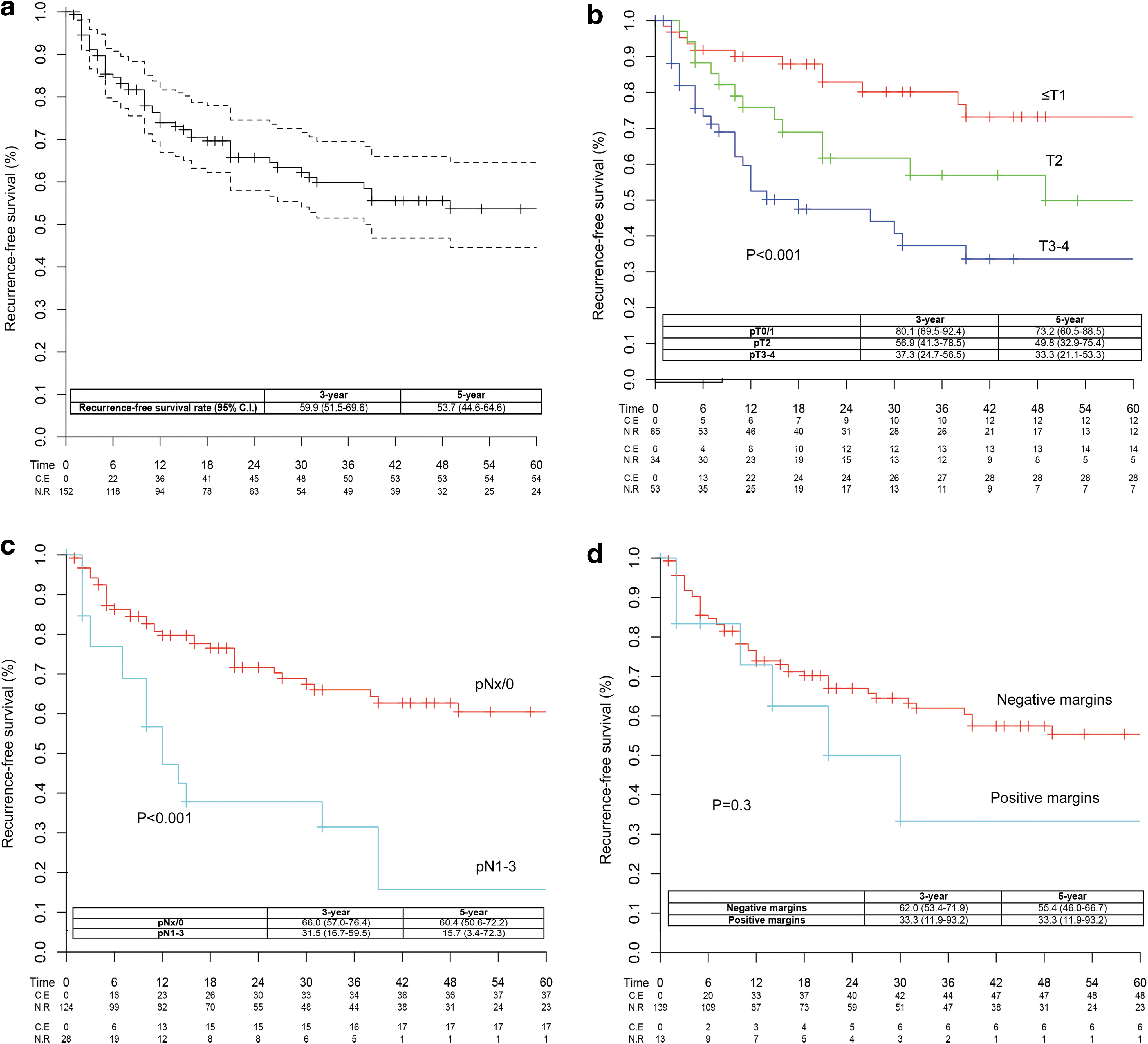
Kaplan–Meier curves depicting recurrence-free survival in the overall population
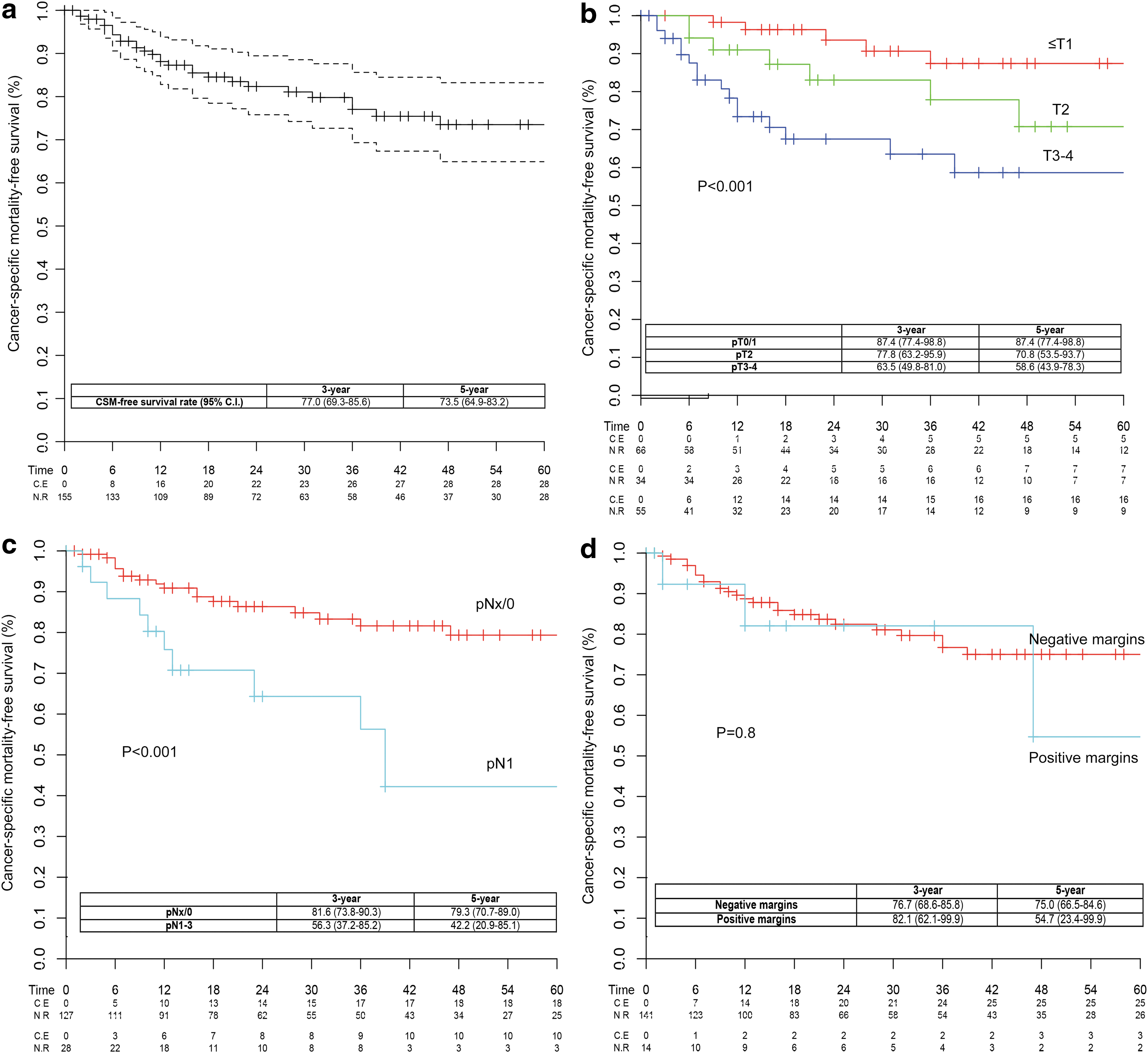
Kaplan–Meier curves depicting cancer-specific mortality (CSM)-free survival in the overall population
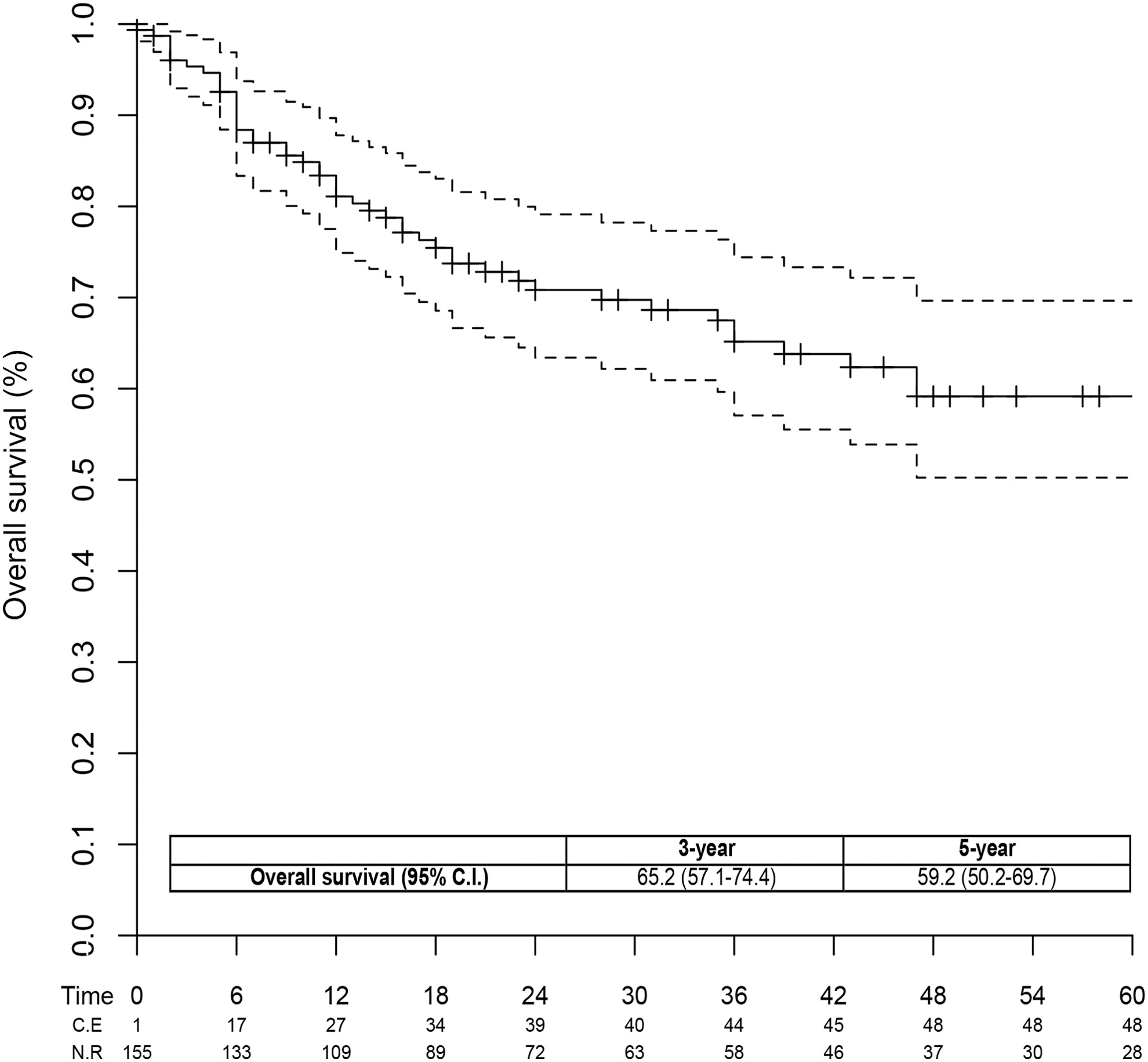
Kaplan–Meier curves depicting overall survival in the overall population.
Table 2 depicts uni- and multivariable Cox regression analyses assessing predictors of recurrence. In multivariable analyses, pathologic stage and nodal stage were confirmed as independent predictors of recurrence after accounting for potential confounders (all p ≤ 0.04).
CI = confidence interval; HR = hazard ratio.
Table 3 depicts uni- and multivariable Cox regression analyses assessing predictors of CSM. Pathologic and nodal stages represented the only independent predictors of CSM (all p ≤ 0.04). Particularly, patients with pT3/4 disease had 3.5-fold higher risk of CSM compared with their counterparts with pT ≤1 disease (p = 0.03). Moreover, patients with pN1–3 disease had 1.8-fold higher risk of CSM compared with those with pNx BCa (p = 0.04).
CSM = cancer-specific mortality.
Table 4 depicts uni- and multivariable Cox regression analyses assessing the predictors of CSM. In univariable analyses, age at surgery, CCI, pathologic and nodal stages, and lymphovascular invasion represented predictors of OM (all p ≤ 0.04). The pathologic stage represented the only independent predictor of OM after adjusting for potential confounders (p = 0.005).
Discussion
Over the last few years, RARC emerged as a novel treatment option for patients with muscle-invasive or high-risk nonmuscle-invasive BCa. Previous studies showed that this approach is safe in terms of perioperative outcomes, where patients treated with minimally invasive surgery might be at lower risk of blood loss, transfusions, and complications. 3,4 Nonetheless, solid data on the oncologic safety and efficacy of this technique are still lacking. 5 Under this light, we aimed at assessing the risk of recurrence, CSM, and OM in a large cohort of patients with urothelial BCa treated at a high-volume robotic center by two experienced surgeons. Moreover, we sought to describe the recurrence patterns and to identify the predictors of recurrence and mortality rate after RARC.
Several results of our study are noteworthy. First, the positive surgical margin rate observed in our cohort was lower than 10%. Moreover, when patients were stratified according to the pathologic stage, the proportion of individuals with positive margins did not exceed 3% among those with organ-confined disease. Conversely, approximately one of five patients with pT3/4 BCa had positive margins after RARC. These findings are in line with previous reports focusing on patients treated with the robotic approach. 5 –9,16 In their systematic review, Yuh and associates 5 recently showed that the positive surgical margin rate ranges between 0% and 25% in patients treated with RARC and it is strongly dependent on disease characteristics. Moreover, the results of our study are comparable with that reported by Novara and associates 17 in a large multi-institutional cohort of patients treated with open RC. Particularly, the authors showed that while a positive margin is a relatively uncommon event in organ-confined disease, more than 20% of individuals with pT4 BCa harbor a positive margin at final pathology. Taken together, these observations demonstrate that the robotic approach might achieve acceptable positive margin rates in patients with urothelial BCa.
Second, given the relatively long-term follow-up of patients included in our cohort, we were able to focus our analyses on strong oncologic outcomes such as recurrence and mortality rate. At 5-year follow-up, more than 50% of the patients included in our cohort were free from recurrence. Additionally, ∼90% of the patients who experienced recurrence had distant metastases and less than 5% of them had peritoneal recurrence. In this context, previous investigations suggested that robotic surgery might result into an increased risk of peritoneal seeding. 6,18 For example, Nguyen and associates 6 recently reported that peritoneal carcinomatosis was more common among patients treated with RARC compared with their counterparts receiving open surgery. Particularly, ∼20% of the patients experiencing recurrence after robotic surgery had peritoneal carcinomatosis. On the other hand, the low rate of peritoneal metastases observed in our series, together with currently available studies showing that the majority of recurrences after RARC occur in distant sites, 5,7,8,10,16 supports the ability of this approach to provide local control and should be reassuring regarding its safety. Of note, this translated into a 5-year CSM-free survival rate of 70%, which is comparable with what was shown by other series evaluating the intermediate- and long-term outcomes of RARC in patients with BCa. 7 –10,16 Additionally, a large multi-institutional study, including more than 700 patients treated with robotic surgery at 11 institutions with a minimum follow-up of 5 years, reported similar results. 10 Although an indirect comparison between open and minimally invasive surgery is difficult, these findings are similar to those observed in patients treated with open RC. Indeed, historical series evaluating the long-term follow-up of patients treated with the open approach in tertiary referral centers reported 5-year CSM-free survival rates ranging between 55% and 70%. 19 –21 Nonetheless, results from prospective, randomized controlled trials are still needed to assess the superiority of one technique over the other.
Finally, our study was able to demonstrate that pathologic stage and nodal status represent independent predictors of recurrence and CSM in patients with urothelial BCa treated with RARC. This is analogous to what was observed in open surgery and confirms that disease characteristics at final pathology represent the main determinant of long-term oncologic outcomes even in patients treated with minimally invasive approaches. 5,10,19,20 On the other hand, we failed to demonstrate an association between surgical margin status and disease-specific mortality rate. Positive soft tissue surgical margins represent well-known predictors of recurrence and mortality rate in patients treated with open surgery. 22 The conflicting results observed in our series might be related to the relatively small number of patients with positive margins and organ-confined disease included. Nonetheless, it should be highlighted that a meticulous resection with a negative margin should represent one of the main goals when performing RARC. 23
From a clinical standpoint, our study supports the long-term oncologic safety of the robotic approach in patients with urothelial BCa. Additionally, we were able to establish the predictors of recurrence and disease-specific mortality rate in our large contemporary cohort of BCa patients treated in a high-volume center. These observations might help clinicians in the identification of individuals who might benefit from a multimodal treatment approach. For example, patients with locally advanced disease and nodal invasion might benefit from systemic therapies, such as neoadjuvant and adjuvant chemotherapy, regardless of the surgical technique. 24 Conversely, their counterparts with organ-confined node-negative disease might be reassured regarding their relatively good long-term prognosis.
Despite several strengths, our study is not devoid of limitations. First, our investigation is limited by its retrospective nature. Second, the population evaluated in this study includes the learning curve of both surgeons with RARC. Additionally, our results were obtained in a high-volume setting. Therefore, they might not be applicable to low caseload centers. Third, the decision of performing a nodal dissection was left to the judgment of the treating physician based on disease characteristics and baseline comorbidities. 25 As a consequence, although nodal status represented an independent predictor of CSM, some patients might have been incorrectly classified in the pNx group. Fourth, the lack of data on intraoperative blood transfusion prevented us from adjusting our multivariable analyses for this potential confounder. 26 –28 Fifth, only well-designed, prospective, multicenter randomized studies with an adequate follow-up can comprehensively address the outcomes of RARC compared with the standard of care, which is currently represented by open surgery. Moreover, the relatively small number of patients with local and peritoneal recurrence prevented us from comprehensively addressing the impact of the site of recurrence on mortality rate. Finally, we included both patients receiving intra- and extracorporeal diversions. Although this might introduce an element of heterogeneity in the surgical technique, none of the available investigations showed an impact of the type of reconstruction on oncologic outcomes.
Conclusions
RARC provides acceptable oncologic outcomes in patients with urothelial BCa treated in a high-volume robotic center. The majority of patients experiencing recurrence had involvement of distant metastatic sites. Tumor stage and nodal status represent independent predictors of recurrence and CSM in patients treated with RARC. These findings might help clinicians in the identification of patients who might benefit from a multimodal treatment approach.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.