
Abstract
Introduction and Objective:
Studies in patients and experimental animals have shown that percutaneous nephrolithotomy (PCNL) can acutely impair glomerular filtration and renal perfusion, but the factors contributing to this decline in renal function are unknown. The present study assessed the contribution of needle puncture of the kidney vs dilation of the needle tract to the acute decline in renal hemodynamic and tubular transport function associated with PCNL surgery.
Materials and Methods:
Acute experiments were performed in three groups of anesthetized adult farm pigs: sham-percutaneous access (PERC), that is, no surgical procedure (n = 7); a single-needle stick to access the renal collecting system (n = 8); expansion of the single-needle access tract with a 30F NephroMax balloon dilator and insertion of a nephrostomy sheath (n = 10). The glomerular filtration rate (GFR), effective renal plasma flow (ERPF), and renal extraction of para-amino hippurate (EPAH, estimates tubular organic anion transporter [OAT] activity) were assessed before and 1 to 4.5 hours after sham-PERC or PERC surgical procedures.
Results:
Overall, GFR responses were similar in all three groups. Sham-treated PERC pigs showed no significant change in ERPF over the experimental observation period, whereas a single-needle stick to access the renal collecting system resulted in renal vasoconstriction (∼30% reduction in ERPF, p < 0.05). Dilation of the single-needle access tract to create the nephrostomy did not lead to a further decline in ERPF. PERC surgical procedure-mediated renal vasoconstriction was most evident at the 1-hour posttreatment time point. A reduction in EPAH was only observed in pig kidneys with a nephrostomy.
Conclusions:
Needle puncture of the kidney for percutaneous access to the renal collecting system is the major driving force for the renal vasoconstriction observed after PCNL surgery, whereas creation of the nephrostomy appears to be largely responsible for decreasing tubular OAT activity.
Introduction
P
PCNL surgery involves gaining access to the renal collecting system by advancing an 18-gauge diamond-tipped needle through the skin and into the kidney. The needle access tract is subsequently expanded with sequential dilators or balloon inflation and stabilized with an Amplatz sheath so that a sufficiently large channel (nephrostomy tract) is created for the introduction of endoscopic instrumentation to view and remove stone(s). The focus of the present study was to identify the contribution of needle puncture vs dilation of the needle tract to the acute decline in renal hemodynamic and tubular transport function associated with PCNL surgery.
Materials and Methods
Animal studies were conducted in accordance with the National Institutes of Health Guide for the Care and Use of Laboratory Animals and were approved by the Institutional Animal Care and Use Committees of Indiana University School of Medicine and Methodist Hospital. The methods of anesthesia, general surgery, percutaneous access of the renal collecting system, and renal function measurements have been extensively described in a previous publication. 2 In brief, anesthesia was induced and maintained with ketamine/xylazine plus isoflurane. Catheters were inserted into the ear vein for infusion of fluids, inulin, and para-amino hippurate (PAH); femoral artery for blood pressure monitoring; renal veins to collect samples for the plasma renin activity (PRA) and to measure the renal extraction of PAH (EPAH); and ureters for retrograde injection of X-ray contrast agent to define renal collecting system and collection of urine. Acute experiments were performed in three groups of anesthetized, adult female farm pigs (∼70 kg body weight). Group 1 consisted of seven sham-PERC (time control) pigs that underwent a skin incision that was later sutured to mimic the period of time required for the PERC procedure. Group 2 consisted of eight pigs that underwent a single-needle stick with an 18-guage diamond-tipped needle to access the renal collecting system. Group 3 consisted of 10 pigs that underwent single-needle access of the urinary space; expansion of the access tract with a NephroMax balloon dilator; insertion of a 30F working nephrostomy sheath; brief visualization of the collecting system with a rigid nephroscope using minimal torque; and 8F Cope loop nephrostomy tube placed in renal collecting system and working sheath removed. The glomerular filtration rate (GFR) and effective renal plasma flow (ERPF) were assessed by the renal clearance of inulin and PAH, respectively. EPAH provided an estimate of the efficiency of tubular organic anion transport. Renal venous PRA was measured by radioimmunoassay of Angiotensin I. All measurements were taken before and 1 to 4.5 hours after sham-PERC or the PERC access procedures.
Statistics
Variables were summarized by means and standard errors of the means. Baseline cardiovascular function measures were compared using one-way analysis of variance. Linear mixed effects models analyzed longitudinal measures. Time was included as a categorical variable to account for potentially nonlinear trends. Random intercepts were used to account for within-subject correlations. Two-sided p-values <0.05 were considered statistically significant. All analyses were performed using SAS 9.4 (SAS Institute, Cary, NC).
Results
Cardiovascular
Baseline blood pressure, heart rate, and renal hemodynamic function were comparable among all three groups (Table 1).
ERPF = effective renal plasma flow; GFR = glomerular filtration rate; HR = heart rate; MAP = mean arterial blood pressure; PERC = percutaneous access.
Mean arterial blood pressure and heart rate
Mean arterial blood pressure (MAP) fell ∼20% during the course of the experiment in the sham-PERC group, with a somewhat similar decline in MAP recorded in the one-needle stick PERC group and a smaller decline (p < 0.05) in MAP recorded in the one-needle+nephrostomy group (Fig. 1A). However, baseline and ending MAPs were similar in all three groups. The heart rate rose to a similar degree in all groups during the course of the experiment (Fig. 1B).

Glomerular filtration rate
Although there was either a trend or significant posttreatment decline in GFR in the two PERC-treated groups compared to their respective baseline values, the responses were not significantly different from those recorded in the sham-PERC group. Overall, GFR responses in both kidneys were similar for all three groups at both the 1 and 4.5 hours posttreatment time points (Fig. 2).
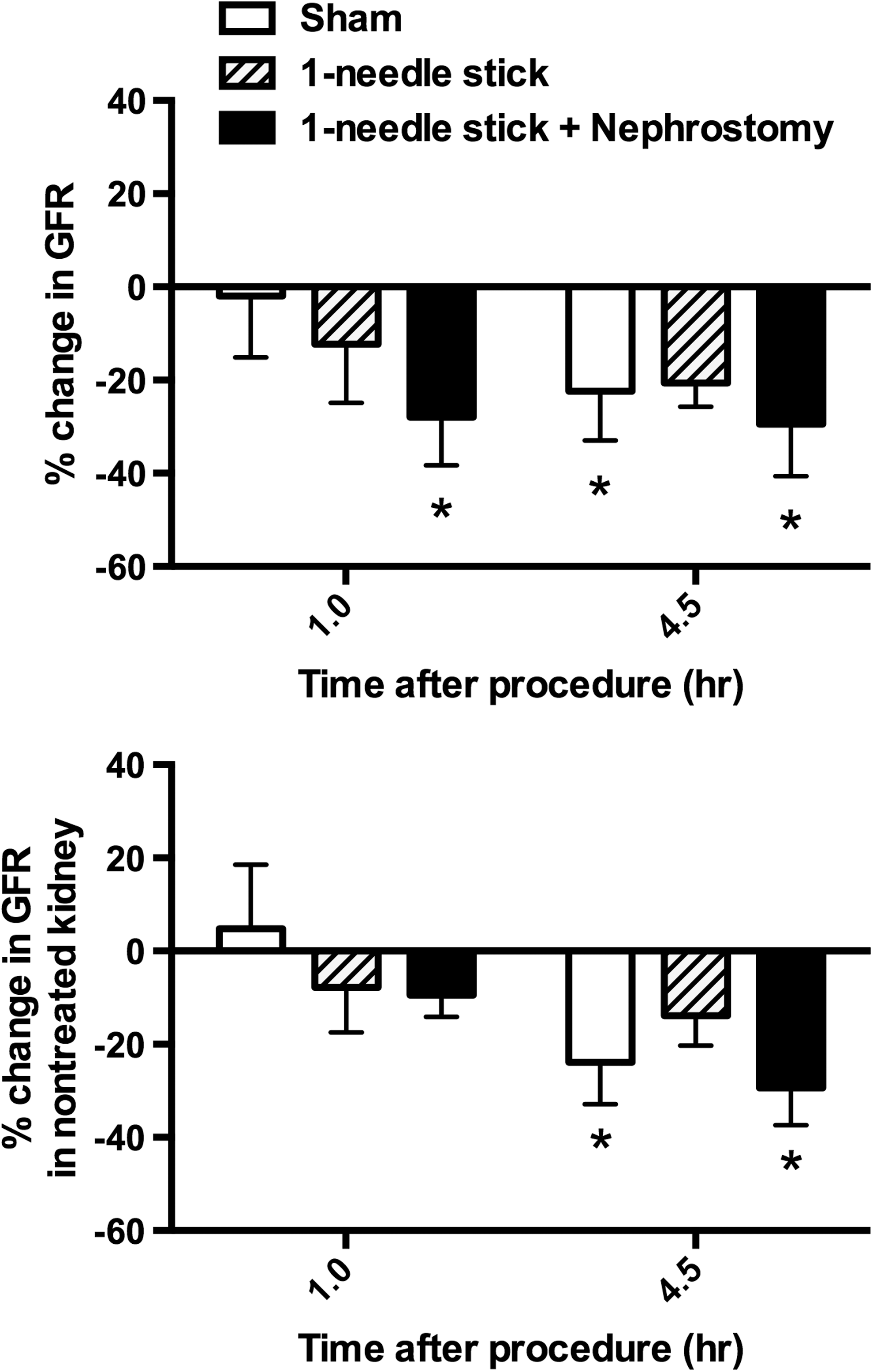
Glomerular filtration rate (GFR) responses in both treated and nontreated kidneys after PERC surgical procedures. *p < 0.05 from corresponding baseline value.
Effective renal plasma flow
Blood perfusion in the sham-PERC-treated kidney was not significantly different from baseline values at both 1 and 4.5 hours after sham treatment. In contrast, the one-needle stick PERC and one-needle stick+nephrostomy PERC-treated pigs had significant decreases in ERPF at both 1 and 4.5 hours posttreatment. These decreases in ERPF were similar in the PERC-treated groups and averaged 30% at 1 hour posttreatment and 35% at 4.5 hours posttreatment. The PERC-treated group responses at 1 hour posttreatment were significantly different from the sham-PERC group. Despite somewhat similar responses observed in all three groups at the 4.5 hours posttreatment time point, statistical significance between the PERC groups and the sham-PERC group was not achieved. ERPF responses in the contralateral kidney were generally similar to the treated kidney for all three groups (Fig. 3). That is, PERC of one renal unit resulted in bilateral renal vasoconstriction.
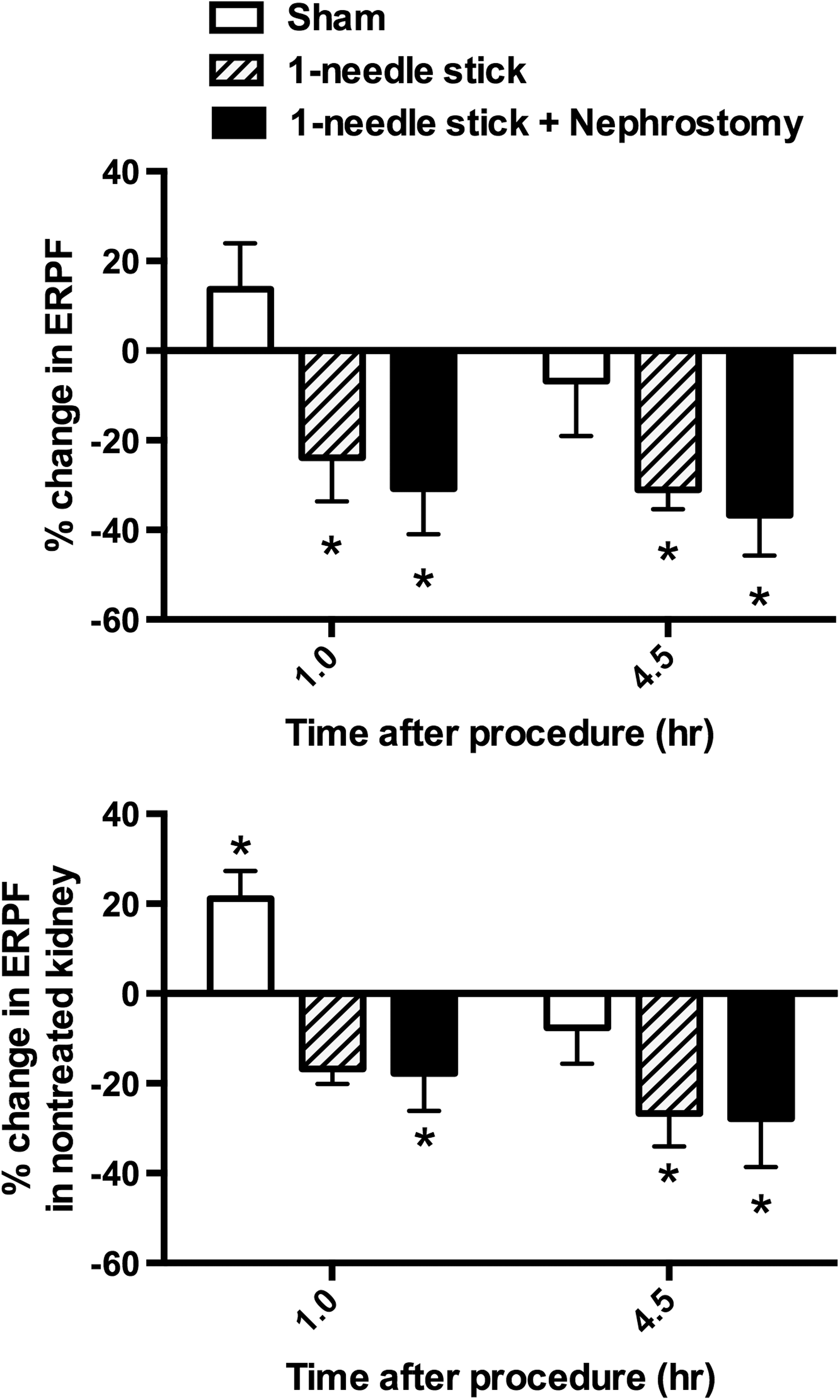
Renal perfusion in treated and nontreated kidneys after PERC surgical procedures. *p < 0.05 from corresponding baseline value.
Renal PAH extraction
EPAH averaged 88% in both kidneys before treatment in all groups (Fig. 4). In the sham-PERC-treated pigs, EPAH remained constant throughout the experiment with no difference between kidneys except for a small 2% difference at 1 hour posttreatment (p = 0.0328). In the one-needle stick PERC group, there was the appearance of a reduced EPAH in the treated kidney at 4.5 hours posttreatment compared to the opposite nontreated kidney. This was largely due to one pig having a 23% decline in EPAH in the treated kidney. In the other four pigs, EPAH was similar in both kidneys at 4.5 hours posttreatment. In contrast, all eight pigs of the one-needle+nephrostomy PERC group had on an average 12% reductions in EPAH at 1 and 4.5 hours posttreatment, which were significant compared to pretreatment values (p ≤ 0.0048) and compared to EPAH in the opposite nontreated kidney (p ≤ 0.0155).

Renal extraction of para-amino hippurate (EPAH) in both treated and nontreated kidneys after PERC surgical procedures. *p < 0.05 from corresponding baseline value.
Renal venous PRA
Figure 5 shows the renal venous PRA from the treated kidney in all three groups over the first 90 minutes of posttreatment. There was a small but significant increase in PRA in the sham-PERC group at 90 minutes. In contrast, renal venous PRA increased threefold to sevenfold in both PERC-treated groups at 30 and 90 minutes posttreatment, which were PRA responses significantly greater (p ≤ 0.0377) than those measured in the sham-PERC group.
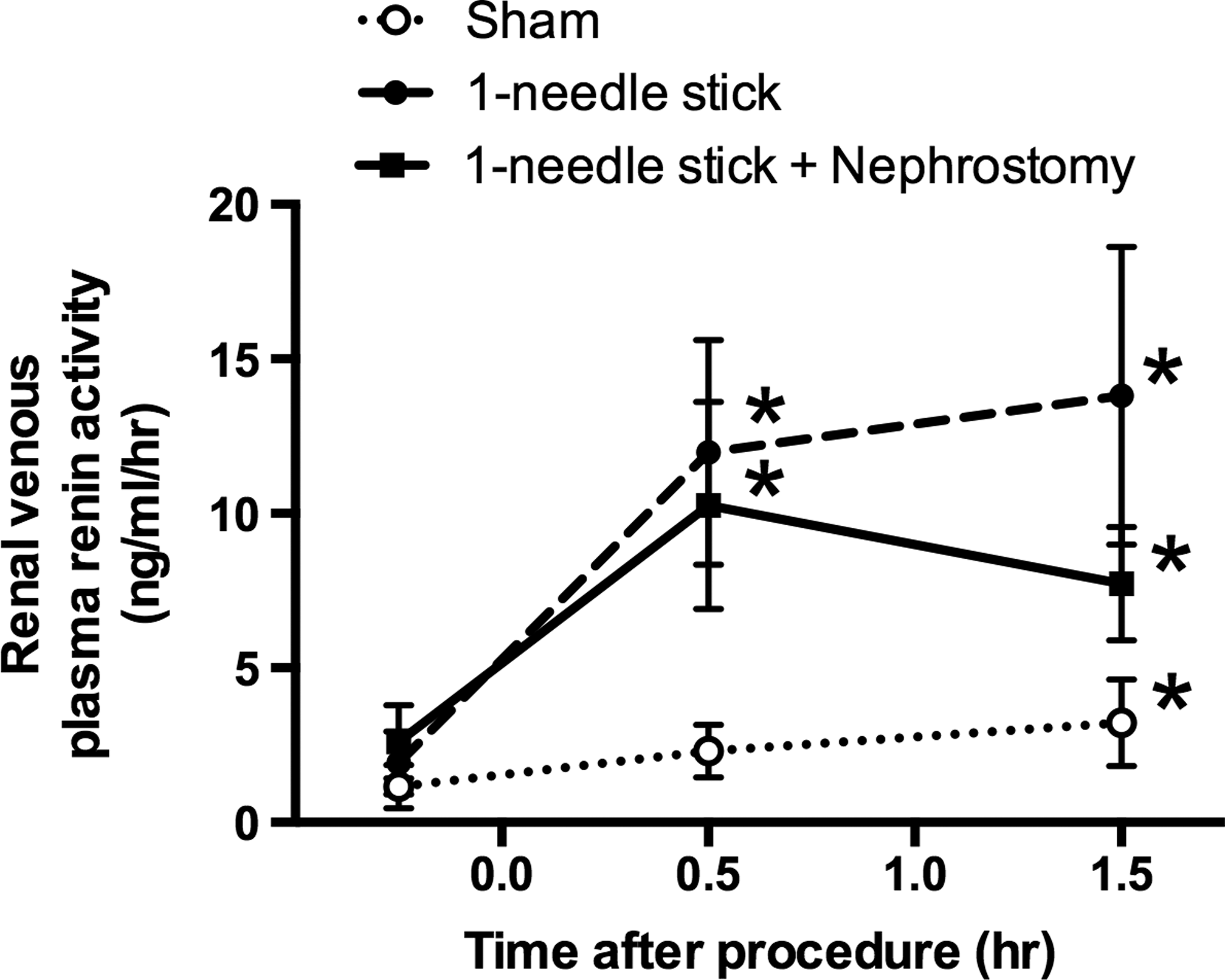
Effect of PERC surgical procedures on renal venous plasma renin activity (PRA). *p < 0.05 from corresponding baseline value.
Discussion
Our results demonstrate that accessing the renal collecting system by simply inserting an 18-gauge diamond-tipped needle through the skin and into the kidney initiated renal vasoconstriction within 1 hour and lasts at least 4.5 hours. Balloon dilation of the needle access site to form a 30F nephrostomy tract did not significantly add to the initial renal vasoconstrictor response. Therefore, gaining percutaneous needle-stick access to the renal collecting system is the major driving force in PCNL surgery for initiating renal vasoconstriction. This highlights that even a single-stick needle puncture of the kidney should be considered a traumatic event leading to renal functional consequences. PCNL surgery often requires multiple-needle sticks to effectively access the renal collecting system and this could potentially result in even greater renal effects. In this regard, we have previously reported much greater declines in GFR and renal perfusion after a conventional PERC surgical procedure that involved an average of three needle sticks to access the pig's renal collecting system. 2 However, a controlled study examining single- vs multiple-needle-stick puncture of the kidney would be needed to validate this suspicion. Our finding would also suggest that dilating the needle access site up to 30F has similar adverse effects on renal hemodynamics as needle-stick access alone. Therefore, the functional impairment associated with PERC surgical procedures employing smaller nephrostomy tract sizes (as in mini-PCNL) will likely be similar to that of conventional PCNL, at least with respect to the acute declines in renal hemodynamics. Although the decrease in renal hemodynamic function after PERC access is most likely short-lived at the whole kidney level, 10 our results provide no information regarding regional changes in renal perfusion and filtration in the damaged pole of the kidney that may potentially be more severe and longer lasting. The clinical significance of such functional impairment and structural trauma to the renal parenchyma 2 is presently unclear, but could potentially adversely impact renal function and postoperative outcomes after PCNL procedures in patients with renal insufficiency, diabetes, or hypertension. 11
Vasoconstriction is not restricted to the PERC-treated kidney as similar effects were measured in the contralateral nontreated kidney. This is in agreement with our previous animal work, in which we demonstrated that single-tract PERC or multiple-tract PERC to a single kidney results in bilateral renal vasoconstriction. 2,12 Such bilateral renal effects have also been reported in patients undergoing unilateral PCNL. 3,6 The mechanism(s) involved in initiating vasoconstriction in the treated and nontreated kidney and the method of communication between both kidneys are unknown, but could involve the sympathetic nervous system (i.e., reno–renal reflexes) and/or humoral systems. Another modality of stone treatment is shockwave lithotripsy (SWL), and we have shown that treatment of one kidney resulted in bilateral renal vasoconstriction and that communication between the two kidneys to initiate vasoconstriction in the nontreated kidney was largely due to the sympathetic nerves. 13 Yet, nonneural factors appeared to be prominent in the vasoconstrictor response in the SWL-treated kidney. 13 The similarity between PERC and SWL effects on bilateral renal function is striking and leads to the suspicion that they may share common effector pathways.
The needle puncture step of PERC surgery appears to be a major stimulus for increasing renal venous PRA. That is, the kidney responded to needle puncture by secreting renin into the blood stream, which will ultimately lead to an increase in blood Angiotensin II—a potent constrictor of blood vessels. Others have also shown that PCNL is a stimulus for increasing plasma PRA in the general circulation of stone patients. 14,15 Therefore, Angiotensin II could be a potential candidate contributing to the vasoconstriction observed in the PERC-treated kidney. Angiotensin II may also potentially be involved in the vasoconstriction recorded in the opposite nontreated kidney as single-needle puncture of one kidney resulted in an increase in renal venous PRA in both the treated and contralateral nontreated kidney (unpublished results). In fact, the stimulus to increase PRA may be multifactorial and include tissue injury-related factors (e.g., oxidative stress 16 ) and/or increased renal nerve activity—the sympathetic nervous system having direct and indirect actions on the kidney to increase renin release. 17
We have consistently shown that the EPAH is decreased after PERC procedures 2,9 (present study) and can last at least 3 days postsurgery. 10 PAH is transported from the blood into the renal tubules through selective organic anion transporters (OATs) located on proximal tubule membranes. 18,19 Hence, EPAH provides an estimate of OAT efficiency. The decline in EPAH after PERC is localized to the treated kidney and may reflect some type of trauma to the renal tubules. Our results would suggest that tissue trauma induced by needle access is not a major stimulus to reduce EPAH, but rather dilation of the needle access site to create a 30F working nephrostomy tract is the key factor for the decline in EPAH—perhaps as a result of impacting additional tissue mass by compressing surrounding tissue. It remains to be determined whether the decline in the renal elimination of PAH would also apply to other drugs eliminated by OATs and whether this elimination defect is restricted to OATs or may encompass other tubular transport systems. Also, whether a smaller size nephrostomy tract (as in mini-PCNL) may have less of an impact on tubular drug elimination.
The cellular mechanism(s) responsible for the reduced EPAH are unknown and could potentially reflect direct trauma to tubules and/or indirect through a redistribution of intrarenal blood flow. 20,21 Others and we have shown that SWL treatment of the kidney may also be associated with a reduction in EPAH. 22,23 Therefore, both PCNL and SWL can acutely reduce the renal elimination of drugs dependent on OAT activity, and it seems reasonable to consider such a potential complication in postoperative medical therapy.
Conclusions
Needle puncture of the kidney initiate the acute vasoconstrictor response of PERC surgery. Balloon dilation of the needle access tract did not significantly add to the renal vasoconstriction, but did appear to initiate the decline in the EPAH—that is, a decrease in the renal elimination of drugs by OAT activity. PERC surgery was also associated with an activation of the Renal Renin–Angiotensin System, which could potentially contribute to the decline in renal perfusion observed after PERC.
Footnotes
Acknowledgments
This study was supported, in part, by funds from the Boston Scientific Co. and U.S. Public Health Service grant P01-DK43881. The authors thank Drs. Jessica A. Mandeville, Ehud Gnessin, Amy E. Krambeck, Naeem Bhojani, Nicole L. Miller, and Marawan El Tayeb for their expertise in PERC access; and to Dr. Robert V. Considine and Anthony Acton Jr. for performing the plasma renin assay.
Author Disclosure Statement
Dr. James E. Lingeman has financial interests in Midwest Mobile Lithotripsy and Midstate Mobile Lithotripsy.