
Abstract
Objective:
To report our experience with concomitant hernia repair during robot-assisted radical prostatectomy (RARP) with a nonprosthetic and tissue-based technique.
Methods:
We conducted a retrospective review on 1005 consecutive patients who underwent RARP between the years 2005 and 2015. Twenty-nine patients, who underwent 37, concurrent, direct, inguinal hernia repairs, were identified (group 1) and compared to a match control group of 29 patients who underwent RARP without hernia repair (group 2). Cases were matched 1:1 for age, body–mass index, and pathologic stage. The reinforcement of the floor was achieved with a modified posterior wall darn repair. The repair consisted of suturing the lateral edge of the rectus abdominis muscle sheath to the ileopectineal ligament (Cooper's ligament) with continuous prolene loose suture. This technique provided a tissue-based repair and the final reinforcement of the floor was expected to ensue by the secondary fibrotic tissue development and maturing between the sutures.
Results:
From a total of 1005 patients who underwent RARP, 29 (2.8%) were preoperatively identified with a primary, direct inguinal hernia and underwent concomitant inguinal herniorrhaphy. The operative time was 147 minutes for group 1 vs 143 minutes for group 2 (p = 0.8). Estimated blood loss was 175 mL for the group with the hernia repair vs 200 mL for the group without repair (p = 0.3). There were no Clavien–Dindo grade >1 complications observed in either of the groups. Mean follow-up period was 32.1 months for group 1 vs 33.3 for group 2 (p = 0.8). Importantly, no hernia recurrences were observed.
Conclusions:
Inguinal hernias represent an important surgical issue and may be repaired concurrently during radical prostatectomy to minimize the risks of postoperative complications. The concomitant repair of inguinal hernias during robotic radical prostatectomy utilizing a nonprosthetic is a safe and feasible alternative for primary direct hernia repair during prostatectomy.
Introduction
I
Methods
This is a retrospective analysis of 1005 consecutive patients who underwent RARP between the years 2005 and 2015. Institutional review board approval was obtained. From this large cohort, 29 patients who underwent 37 concurrent direct inguinal hernia repairs were analyzed. Hernia diagnosis was confirmed by physical examination before surgery performed by the surgeon himself. Patients with bowel in the hernia sac or recurrent hernias after a previous hernia repair (56 patients in the entire cohort) were excluded from analysis, since they were managed with the use of a mesh. Patients with a diagnosis of indirect hernias were likewise excluded, since the management was either by a prosthetic repair or purse-string suturing of the internal inguinal ring. Thus, patients included in the analysis had direct hernias and none underwent previous inguinal hernia repair.
Preoperative patient characteristics evaluated included age, serum prostate-specific antigen (PSA) value, body–mass index (BMI), and American Society of Anesthesiologists Score. The intra and postoperative data documented included operative time, estimated blood loss, use of nerve-sparing technique, pathologic stage, Gleason Score in the specimen, surgical margin status, length of hospital stay, day of catheter removal, complications, and hernia recurrence. The 29 patients who underwent hernia repair (group 1) were compared to another 29 matched controls, who underwent RARP without a hernia repair (group 2). Cases were matched 1:1 for age, BMI, and pathologic stage, and 29 were randomly chosen for comparison from the matching cohort. All procedures were performed by the same surgeon (A.R.K.) with a six-port configuration using the DaVinci® surgical system.
Hernia repair was performed upon completion of radical prostatectomy, lymph node dissection (when indicated), specimen extraction, and securing of a water-tight anastomosis. Port configuration was kept unchanged. The initial step was to reduce the contents of the hernia followed by reconstruction of the posterior abdominal wall. The reinforcement of the floor was achieved by a modified posterior wall darn repair. 5 The technique consists of suturing the lateral edge of the rectus abdominis muscle sheath to the ileopectineal ligament (Cooper's ligament) with 2/0 prolene using a continuous loose suture secured after every other knot (Fig. 1). The two edges of the continuous suture were secured with clips (Fig. 2). The suturing line started and ended at the same spot (Fig. 2). This technique provided a nonprosthetic and tissue-based repair and the final reinforcement of the floor was anticipated to ensue by the secondary fibrotic tissue, which would grow and mature between the sutures. The two groups were compared for operative time, blood loss, complications, and most importantly hernia recurrence. Recurrences were evaluated by physical examination and performed by the surgeon himself initially at 3 months after surgery and yearly thereafter. Radiological imaging was not performed for hernia recurrence follow-up. Statistical analysis used involved t-test for unpaired samples using SPSS v21 for Windows (IBM). The point of statistical significance was set at 0.05.

Direct hernia and involved anatomical structures.
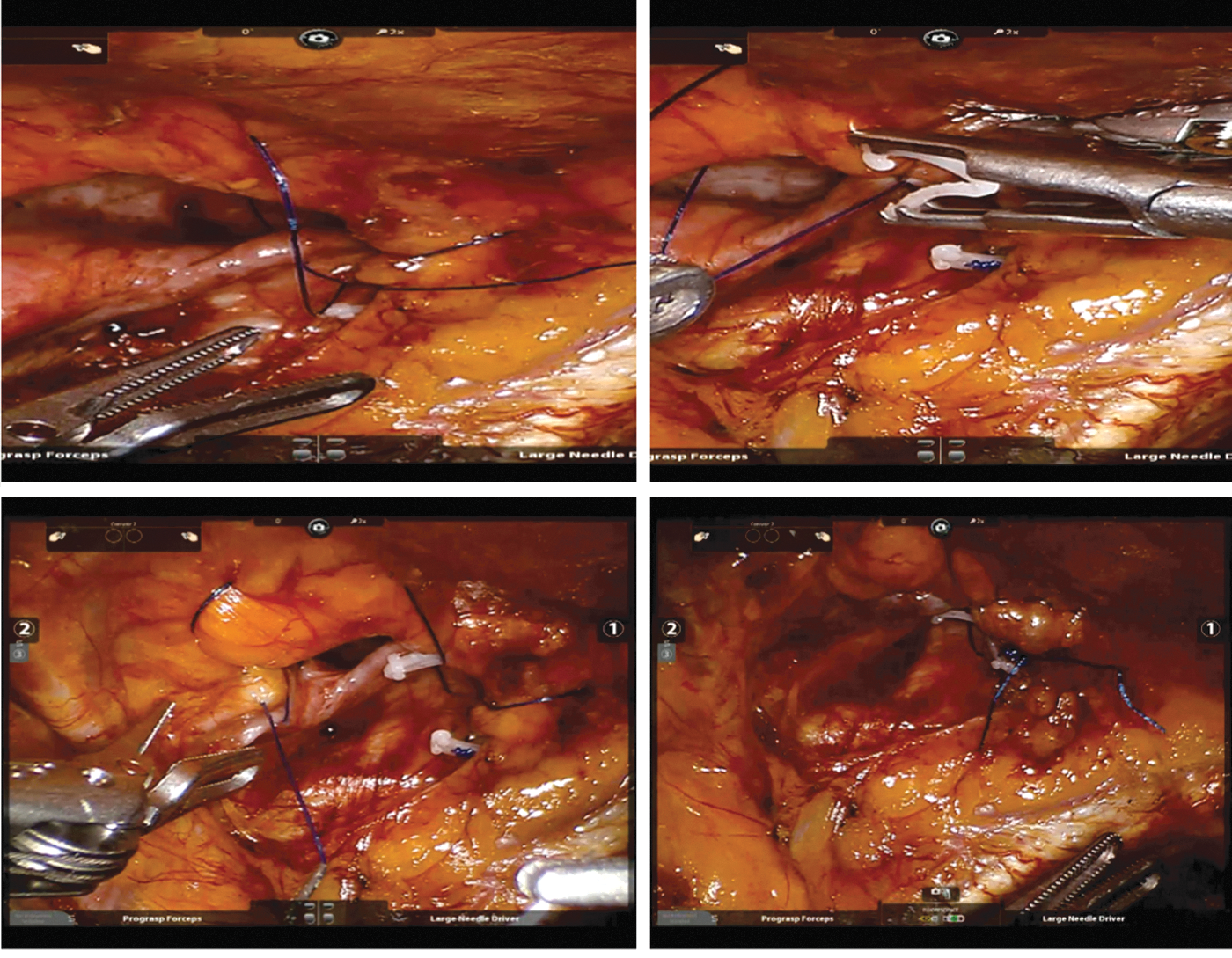
“Darning Technique” suturing the lateral edge of rectus abdominis muscle with ileopectineal (Coopers) ligament.
Results
RARP was performed on 1005 consecutive patients. Inguinal hernia was detected preoperatively by physical examination in 29 (2.8%) patients, who underwent a total of 37 inguinal herniorrhaphies during robotic prostatectomy; 7 (24%) left-sided, 14 (48%) right-sided, and 8 (28%) bilateral repair. The mean age was 62.8 vs 61.9 years (p = 0.518), the mean PSA value was 9.2 vs 6.4 ng/mL (p = 0.251) and the mean BMI 26.47 vs 26.44 kg/m2 (p = 0.947) for groups 1 and 2, respectively. Ten of 29 (34%) patients had a history of past abdominal surgery in group 1 and 15 (52%) in group 2 (p = 0.20). The prevalence of smoking and diabetes was similar in both groups; 18 (62%) and 22 (75%) smokers (p = 0.29) and 11 (38%) and 12 (41%) diabetics in groups 1 and 2, respectively. Patient characteristics are summarized in Table 1. None of the patients received radiation or hormonal treatment after surgery in either group.
Data are presented as mean ± standard deviation.
BMI = body–mass index; PSA = prostate-specific antigen; RARP = robot-assisted radical prostatectomy.
The comparison of the two groups for the intra and postoperative characteristics revealed no statistically significant differences. The operative time was 147 minutes for group 1 vs 143 minutes for group 2 (p = 0.785). The estimated blood loss was calculated as 175 mL for the group with the hernia repair vs 200 mL for the group without repair (p = 0.337). There were no Clavien–Dindo grade >1 complications observed in either of the groups. Likewise, postoperative characteristics revealed similar rates in the length of stay (4.3 vs 4.6 days) and day of catheter removal (6.5 vs 6.4 days), for groups 1 and 2, respectively. The pathology report revealed tumors with similar characteristics in both groups as depicted in Tables 2 and 3. The mean follow-up period for groups 1 and 2 was 32.1 and 33.3 months, respectively (p = 0.835). Hernia recurrence was not observed in any patient within this period.
Discussion
Inguinal hernia has a relatively high prevalence in the general population, which is reported at around 7.2%, but may reach up to 14% in the male population, even after excluding the subclinical ones. 6 This problem may concur with surgical conditions of the true pelvis, such as prostate surgery. The coincidence may be as high as 33%, based on open radical prostatectomy series. 7 High rates of inguinal hernia (21%) were also noted following open radical prostatectomy surgery, implying that the hernia was unrecognized preoperatively. 8 Thus, careful physical examination appears to be mandatory. Obtaining preoperative computed tomography scan would minimize unrecognized hernias; however, its routine use would probably not be recommended due to cost and radiation issues. 9
There are many reports in the literature concerning hernia repair during open radical prostatectomy. In a relatively large cohort of 108 patients, who underwent 141 inguinal hernia repairs during open radical prostatectomy, Savetsky et al. reported a low complication rate with a 2.8% recurrence at 16 months of follow-up. 10 Many different techniques for minimizing the incisions and shortening the surgical time have been established. 11 As laparoscopic hernia repair evolved and laparoscopic radical prostatectomy followed, the combination of these two minimally invasive techniques became inevitable. In a study reporting the experience with this laparoscopic combination, the mean operative time was significantly longer in the group who underwent simultaneous laparoscopic inguinal hernia mesh repair (221.9 vs 191.2 minutes, p = 0.011). Complication rates, however, were comparable (4% vs 2%). The authors concluded that this technique was feasible and safe. 12
Laparoscopy expanded with the inauguration of robotic technology. As the experience in RARP evolved, new data emerged regarding the effectiveness and safety of repairing inguinal hernias during RARP. Finley et al. performed 49 concurrent herniorrhaphies in 40 patients during RARP. They used mesh routinely except for two small hernia repairs. The investigators reported a slight increase in the operative time (<10 minutes in all cases), when hernia repair was performed; a statistically significant difference was not noted in the length of stay and in postoperative analgesics. Hernia recurrence rate was 2% at a median follow-up of 15.3 months. 12 Further data regarding incidentally detected inguinal hernias were published by Lee et al. They followed 91 patients who underwent 113 herniorrhaphies during robotic prostatectomy using a mesh. These investigators stated that this type of repair was effective and safe with only a slight increase in the operative time (185 vs 168 minutes, p < 0.01) without increasing morbidity. They reported one hernia recurrence requiring further repair. 3
All hernias in the present series were diagnosed preoperatively, whereas all in Lee et al. series were detected incidentally during surgery. 3 Interestingly, in the University of California-Irvine experience, 50% had an abnormal physical examination and another 50% were incidental. 13 It is not easy to explain the discrepancy among the three series. We might have missed some during surgery and Lee et al. might have missed some preoperatively. It is essential that urologists performing radical prostatectomies are cognizant of the significant incidence of coincidental inguinal hernias and trained for its management.
Importantly, the two above-mentioned studies used mesh for hernia repair. 3,13 Although the effectiveness of mesh repair is well documented, 14,15 it has a few inherent potential complications. The risk of infection is low, although not zero. 16 Once the bladder is dropped from the abdominal wall during transperitoneal surgery, there is always the risk of the mesh coming in contact with urine. Another concern with prosthetic mesh is the potential risk of bowel adhesions. The use of the tacking device for mesh fixation could create postoperative neuralgia. Utilizing mesh is also associated with increased expenditure. There are reports in the literature about successful repair results with suturing techniques. 17,18 We were able to demonstrate that direct hernia repair using a modified darn repair is both feasible and safe, when performed concomitantly with RARP. One of the advantages of suture-based repairs over permanent mesh repair would be the avoidance of foreign body material. Unlike the two above-mentioned studies, surgical time was not any longer with the addition of hernia repair to prostatectomy. This was probably due to the fact that suturing is relatively easy compared to laying and securing the mesh, which is more tedious. Recurrence rate with the present technique was null, again a better result compared to the two previously published robotic herniorrhaphy studies. 3,13
To the best of our knowledge, this is the first series in the literature to report on concurrent nonprosthetic inguinal hernia repair during RARP. We acknowledge that there are limitations to our study. The retrospective nature of the study and the relatively small number of patients may have compromised our results. None of the patients had previous hernia repairs, so we cannot draw conclusions for cases with previous herniorraphy. Despite the fact that the mean follow-up of our patients is above 2 years, there are two cases in the hernia repair group that were followed only for 3 months, a period small for definitive conclusions about a possible recurrence.
Conclusions
Inguinal hernias represent an important health issue for prostate cancer patients undergoing radical prostatectomy. These coincidental hernias may be repaired concurrently during radical prostatectomy to minimize the risks of postoperative complications. The concurrent repair of small, nonbowel containing, direct inguinal hernias during robotic radical prostatectomy utilizing a nonprosthetic tissue-based technique is relatively easy, safe, and effective in short term and may be considered an alternative technique for repairing inguinal hernias during RARP.
Footnotes
Author Disclosure Statement
No competing financial interests exist.