
Abstract
Introduction:
Several prostatic stents were developed in the last three decades, none of which were able to provide a real alternative in patients unfit or unwilling to undergo classical prostatic surgeries. In this study, we report the results of the use of a newly developed prostatic stent—the Allium™ Triangular Prostatic Stent (TPS).
Patients and Methods:
The Allium TPS is a highly flexible, nitinol-built polymer-covered stent, which prevents tissue ingrowth and reduces encrustations. Between 2008 and 2014, at two centers (Israel and Turkey), the stent was inserted under local or regional anesthesia in 51 patients with benign prostatic obstruction (BPO) who are unwilling or unfit for surgery. Patients were followed for 12 months from surgery. The primary outcome was symptom improvement as measured by the international prostate symptom score (IPSS) and improvement in peak urinary flow.
Results:
Stent insertion was successful in all patients. The mean IPSS decreased from 26.4 to 7.7 on the last follow-up. The mean peak flow increased from 5.5 mL/second before stent insertion to 16.0 mL/second 1 year thereafter. The main adverse effect was transient pain in nine patients. No stent migration or obstruction was seen. Patients reported satisfaction and improvement in quality of life.
Conclusion:
Our short-term results show that Allium TPS is safe and effective for the treatment of patients with BPO.
Introduction
P
Regarding efficacy, all clinically studied prostatic stents showed some degree of symptoms (international prostate symptom score [IPSS]) and flow (maximal urinary flow [Qmax]) improvement. 2,3,6 –9 However, several stents showed high short- and long-term failure rates of as much as 46% in 3 months. 9
The stent design can significantly affect its safety and efficacy. This fact has been shown in a randomized controlled study of blind prostatic stents. 10
The available stents in use nowadays have a high failure rate and significant side effects, and as such, the latest European Association of Urology (EAU) guidelines state that prostatic stents have a limited role in the treatment of moderate-to-severe low urinary tract symptoms (LUTS).
In our study, we are reporting the efficacy and safety of a newly designed prostatic stent called Allium™ Triangular Prostatic Stent (Allium™ TPS; by Allium Medical, Caesarea, Israel).
Patients and Methods
Stent design
Allium TPS is a coiled, superelastic highly flexible stent built of nitinol and fully covered with a copolymer, which prevents tissue ingrowth. It also reduces encrustations, stone formation, and calcifications. The stent (shown in Fig. 1) is designed in a triangular shape, which, compared with circular stents, allows for less tissue to be pushed aside, causing less irritative symptoms. It is built of a body of eight different lengths ranging from 30 to 65 mm with a large caliber (45F); attached to the body with a trans-sphincteric wire is an anchor (Fig. 1), which reduces the chance of stent migration. Once inserted into the urethra with the aid of its special inserter, the stent is released to allow its self-expansion.

Allium™ triangular prostatic stent (TPS) and Tiemman-like delivery system.
Stent insertion
Patients received prophylaxis antibiotics before surgery with vancomycin and third-generation cephalosporin. Stent insertion can be done under local or regional anesthesia with minimal patient discomfort using a specially designed delivery system (Fig. 2). First, a 12F measuring catheter is inserted and its balloon inflated with 15 mL saline. Then, a 15F to 17F cystoscope is inserted beside the catheter and advanced to the bladder neck. The balloon is then pulled to the bladder neck and the cystoscope withdrawn while counting the marks on the measuring catheter between the bladder neck and the verumontanum. This measure gives the length of the prostatic urethra and its appropriate Allium TPS length (30–65 mm, with 5 mm difference between each). The cystoscope and the measuring catheter are then removed and the delivery system, which includes the stent, is inserted (like a urethral catheter) and its balloon inflated with 15 mL saline (Fig. 2). While keeping the balloon at the bladder neck with gentle traction, the trigger on the delivery system should be pulled 6 to 10 times until the stent is totally deployed (Fig. 2). The balloon is then deflated and the delivery system removed. Another important feature of the Allium TPS stent is the unraveling feature, which ensures a safe, easy, and nontraumatic removal (Fig. 3).
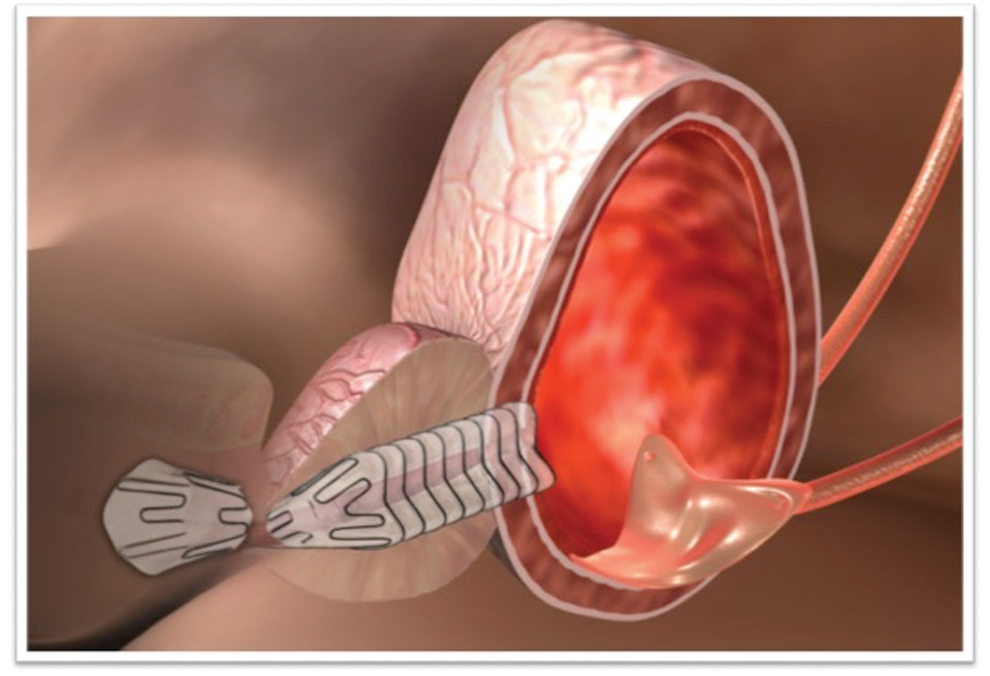
Illustration of indwelling Allium TPS.
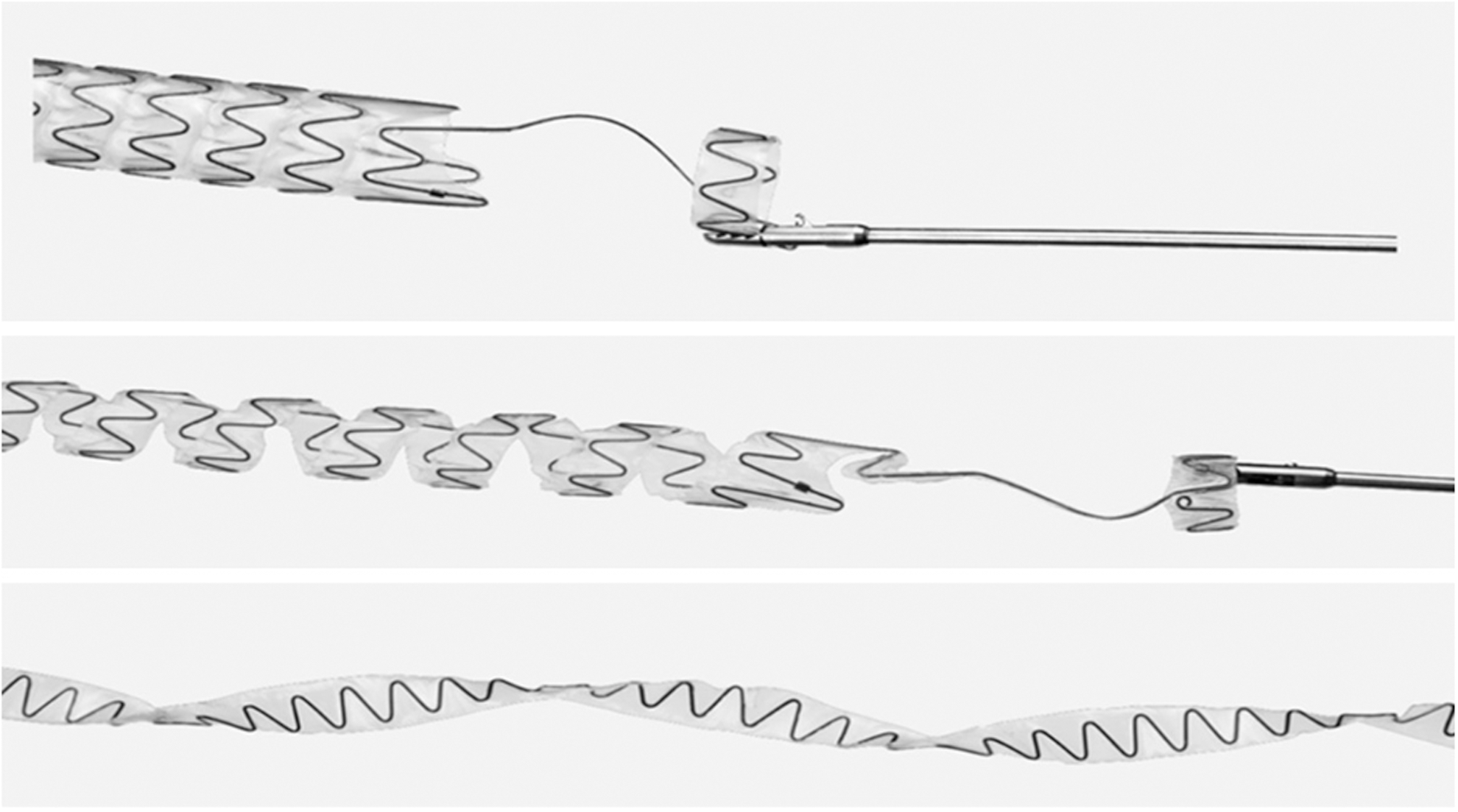
Unraveling feature of Allium TPS.
Patients
Between 2008 and 2014, 51 Allium TPSs were inserted in 51 patients with clinically diagnosed severe BPO, who failed medical treatment, and were not willing or unfit (because of high risk for anesthetic complications) to undergo classical prostatic surgery. BPO was diagnosed based on the clinical diagnosis score (IPSS >20) and decreased Qmax (<10 mL/second). All procedures were performed in the following urology departments: Bnai-Zion Medical Center, Haifa, Israel and Dr. Suat Seren Chest Diseases and Surgery Teaching and Research Hospital, Izmir, Turkey. All patients received a detailed explanation of the procedure and its sequela. All patients signed an informed consent form and each institutional review board approved the study. Exclusion criteria included age younger than 18 years, acute urinary tract infection, patients with penile or artificial sphincter implants, cystolithiasis, atonic bladder, non-BPO-related LUTS, and patients with large prostate volume (>100 cc).
Patients were discharged on postoperative day 1. Follow-up data were obtained on postoperative day 1 and 3, 6, and 12 months following surgery. Follow-up data included peak urinary flow, postvoiding residual (PVR), and patient-assessed IPSS. In addition, patients were asked about adverse events related to stent insertion.
Statistical analyses
Continuous variables were summarized with a mean standard deviation and median. Categorical variables were analyzed by a count and percentage. Peak flow, IPSS, and PVR were all analyzed with repeated-measures ANOVA (SAS PROC MIXED), where each was modeled as a function of visit. Least squares (LS) mean (model-estimated means) differences between the visits were estimated from the models and are presented with respective levels of significance (only for the baseline to 12-month visit, others are not shown). All statistical tests were two-sided and tested at a 5% level of significance. Nominal p-values are presented. Statistical analyses were performed using SAS V9.3 (SAS Institute, Cary, NC).
Results
Patients' baseline characteristics are summarized in Table 1. Patients' mean age was 72.8 ± 7.4 (Median = 73) years and all, except one, had an American Society of Anesthesiologists (ASA) score of 3. Mean prostate volume, as measured by abdominal ultrasonography, was 38 ± 14.6 cc (Median = 33). All patients had severe symptoms with IPSS of 22 or more. All patients had abnormal peak urinary flow with a mean of 5.5 ± 1.4 mL/second (Median = 5) and a range of 3.8 to 8.0 mL/second. Mean PVR was 58.8 ± 37 cc (Median = 62.5).
All patients had an ASA score of 3, except one (ASA = 4).
Measured by abdominal ultrasonography.
ASA = American Society of Anesthesiologists; IPSS = international prostate symptom score; PVR = postvoiding residual.
Stent insertion was done in all 51 patients under local or regional anesthesia with no intraoperative complications. Six different stent lengths were used as shown in Table 2.
Immediately following stent insertion, all patients had statistically significant improvement in peak urinary flow. On the last available follow-up (12 months following surgery), all patients had significantly higher peak flow and significant improvement in IPSS. The mean IPSS significantly decreased from 26.4 to 7.7 on the last follow-up (Table 3). The mean peak flow significantly increased from 5.5 mL/second before stent insertion to 16.0 mL/second 1 year following thereafter. Most patients reported significant improvement in quality of life when asked to compare current symptoms with preoperative symptoms. Data are summarized in Table 3.
p-Value is the level of significance of the LS mean difference between baseline and 12 months from the repeated-measures ANOVA models.
ANOVA = analysis of variance; LS = least squares; NA = not available; NR = not relevant.
The stent was tolerated in all patients, with few adverse effects. The main complications are summarized in Table 4. Most adverse events were mild (Clavien–Dindo grade I or II). However, two patients had Clavien–Dindo grade III complications and needed surgery for stent removal. The 12-month failure rate was 3.9% (two patients: the first patient underwent stent removal 1 month from insertion due to chronic infection; the second patient underwent stent removal 2 months following insertion due to recurrent gross hematuria). The main adverse effect was pain in nine patients (18%), which resolved in all patients in 1 to 5 days after stent insertion. Another adverse effect was infection, seen in five patients (9.8%), which resolved in all but one patient after an antibiotics course. None of the patients reported stent-induced incontinence. No stent migration or occlusions were seen in any of the patients.
Two stents were removed: one due to hematuria (after 2 months) and the other due to chronic infection (after 1 month).
Discussion
Prostatic stent is a three-decade-old idea, but since its introduction, several improvements have been implemented. The stents that are in clinical use nowadays have limited role mainly due to high failure rates. 11,12
In a systematic review of 990 patients who underwent UroLume® stent insertion, Armitage et al. reported a 16% failure rate in the first year (only 61% of the patients were evaluable at that point). 11 In another systematic review of Memokath® thermo-expanding metallic stent, failure rates of as much as 48% were reported. 12
The main reasons of failure after Memokath or UroLume insertions were incorrect stent placement, stent migration, encrustations, urinary retention (stent occlusion), and incontinence. 11,12 Allium TPS was designed to overcome these limitations. The delivery system makes stent placement easy and safe, minimizing the risk of stent misplacement. The anchoring part, which is placed in the urethra, minimizes the risk of stent migration. The Allium TPS is coated with a specifically designed copolymer that prevents tissue ingrowth and encrustations. None of the patients had encrustations. Moreover, none of the stents were occluded. None of our patients had urinary incontinence following Allium TPS insertion. The reason for this finding is the trans-sphincteric wire, which does not compress the sphincter.
Markovic and coworkers were the first to report the use of Allium stents, including TPS, in preliminary studies of safety. 13 However, no data were published about the use of Allium TPS, despite it being approved for clinical use for several years.
Regarding stent efficacy, the mean IPSS following stent insertion showed that all patients, who started with severe symptoms, had significant decrease in IPSS and were regarded as having mild symptoms (IPSS change of −18.7). We also provided urinary peak flow, which, despite its limitations, provides an objective measurement. We showed an increase of 10.5 mL/second in the peak urinary flow following Allium TPS insertion.
We are aware of our study limitations, which include a small number of patients and short-term follow-up. Most patients are still on follow-up and we will report a longer follow-up when available.
Conclusions
In this primary study of Allium TPS, we showed a new promising treatment option in patients with BPO who are unfit or unwilling to undergo classical prostatic surgery. Allium TPS is safe with minimal adverse effects and is effective, showing significant reduction in IPSS and increment in urinary flow. The stent can be easily inserted and easily removed if needed. A larger, randomized multicenter study should be conducted to prove our results.
Footnotes
Acknowledgment
The authors would like to thank Dr. Lisa Deutsch for statistical analysis.
Author Disclosure Statement
No competing financial interests exist.