
Abstract
Purpose:
We found current robotic positioning devices to be inadequate and cumbersome. Furthermore, we realized there were no premarket well-designed studies to prove their safety and efficacy. In this prospective pilot study, we aimed to investigate the safety and effectiveness of a novel patient-positioning device (SAF-R) to secure the patient in Trendelenburg (T-burg) position for robot-assisted pelvic surgery.
Patients and Methods:
Sixteen patients undergoing robot-assisted pelvic operation in T-burg position were enrolled. Patients were positioned using SAF-R board. Pressure sensor mats were used for real-time monitoring of the contact pressures and contact area on the shoulders and calves throughout the surgery. Data collection included patients' body mass index (BMI), time needed for positioning, total time in the T-burg position, contact pressure and contact area readings from the sensor mats, and the patient shifting distance on the table. Patients were also followed for 1-month postoperatively for any position-related adverse event.
Results:
The median age of the patients was 56.5 years with median BMI of 27.3. The median positioning time was 6 minutes, duration of T-burg position was 3.5 hours, and patient shift on the table was 1 cm. The contact pressure over the shoulders was in the safe range (<80 mm Hg) before and at the end of the surgery in all cases (right: 13.12 ± 1.12 vs 20.25 ± 1.56 mm Hg, left: 12.84 ± 1.05 vs 19.60 ± 1.09 mm Hg, p = 0.001). The changes in the mean contact pressure over the calves and the mean contact area for the shoulders and calves during the T-burg position were not significantly different. No significant position-related complication was detected during follow-up.
Conclusions:
SAF-R surgical board is a safe, reliable, and timesaving positioning device for patients undergoing robotic pelvic surgery in the T-burg position.
Introduction
R
Currently, the available devices used for patient positioning in steep T-burg are often time-consuming to set up or perform in a suboptimal fashion. Besides, these devices lack sufficient premarket studies to prove their safety and efficacy. Through collaboration among medical engineers, surgeons, and anesthesiologists, the SAF-R positioning device is configured to secure the patient quickly, easily, and reproducibly for such operations with minimal slippage on the operating table.
In this prospective pilot study, we aimed to test our hypothesis by investigating the safety and effectiveness of the SAF-R positioning device during robot-assisted pelvic surgery.
Patients and Methods
The hospital institutional review board approved the protocol for this prospective pilot study. Patients undergoing robot-assisted urologic or gynecologic procedures were enrolled. A thorough informed consent was obtained from each patient in the study. Exclusion criteria included weight of more than 250 lbs, a past medical history of neuropathic pain, and/or considerable joints disorder such as rheumatoid arthritis and degenerative joint disease.
Surgical board (SAF-R)
The Massachusetts General Hospital design team agreed that our product should meet the following criteria: (1) The device should be safe to the patient and cause no abnormal pressure on joints and/or soft tissue, particularly over the shoulders, (2) it should not cover the chest, neck, or arms, (3) it should add no pressure on the chest, hence minimizing any adverse effects on intraoperative ventilation for the patient, and (4) it should be easy to assemble and use. These prerequisites led to the design depicted in Figure 1. The device consists of a main baseboard and two detachable upper back supports (Fig. 1). The main board is attached to the upper back supports by means of a dovetail interlocking mechanism. The detachable back supports are secured to the operating table by means of L-shaped rods and Clark adaptors. The baseboard is made of plexiglass and is curved to follow the arch of the upper back. A separate, detachable, reusable, durable waffle gel mat covers the entire board and also envelops the arms on either side. This medical grade waffle gel has lower interface dermal pressures, hence lowering the risk of causing pressure sores compared to existing gel mats.

SAF-R Surgical board.
Patient positioning
The assembled board with the gel mat was placed on the operating room table without fixing it to the side rails. The patient was asked to lie on the board with his shoulders snugly against the upper back supports. Following induction of anesthesia, the upper back supports were secured to the operating table once the surgeon was satisfied with the position of the patient. All patients were placed in a modified dorsal lithotomy position with legs padded and secured in stirrups (Yellofins®, Allen Medical Systems; Hill-Rom Holdings, Inc., Acton, MA). The patients' arms were tucked to the side of patients with the arm extensions of the SAF-R board and secured to the operating table by using side toboggan arm boards. At this point, the patient was placed in the T-burg position and robot was docked. The patient's T-burg angle was maintained and did not change throughout the console time.
Measurements and data collection
Patient demographic data including age and body mass index (BMI), as well as time needed for positioning, total time in the T-burg position, and the degree of T-burg position were recorded in each case.
We used TekScan pressure sensor systems (Tekscan, Inc., Boston, MA) for monitoring the contact pressures over the shoulders and calves areas (Figs. 1D and 2). For this purpose, interface pressure sensor mats were placed between the patients' skin and the gel mat over the shoulders and posterior calves. The system was capable of real-time, continuous dermal interface pressure measurement and mapping. 5 The pressure zones were seen as color pixels on a computer screen ranging from light blue to deep red depending on the pressure scale set at the outset of the study. We recorded a single snapshot from each of the four pressure sensors every minute starting after finalizing the patients' positioning and continuing throughout the operation. For analysis purposes, we used the data snapshots before T-burg positioning and every 20 minutes during the T-burg position. The average of three consecutive recording was used for each interval (Fig. 3). Data regarding contact area, mean contact pressure, and maximum contact pressure were recorded.
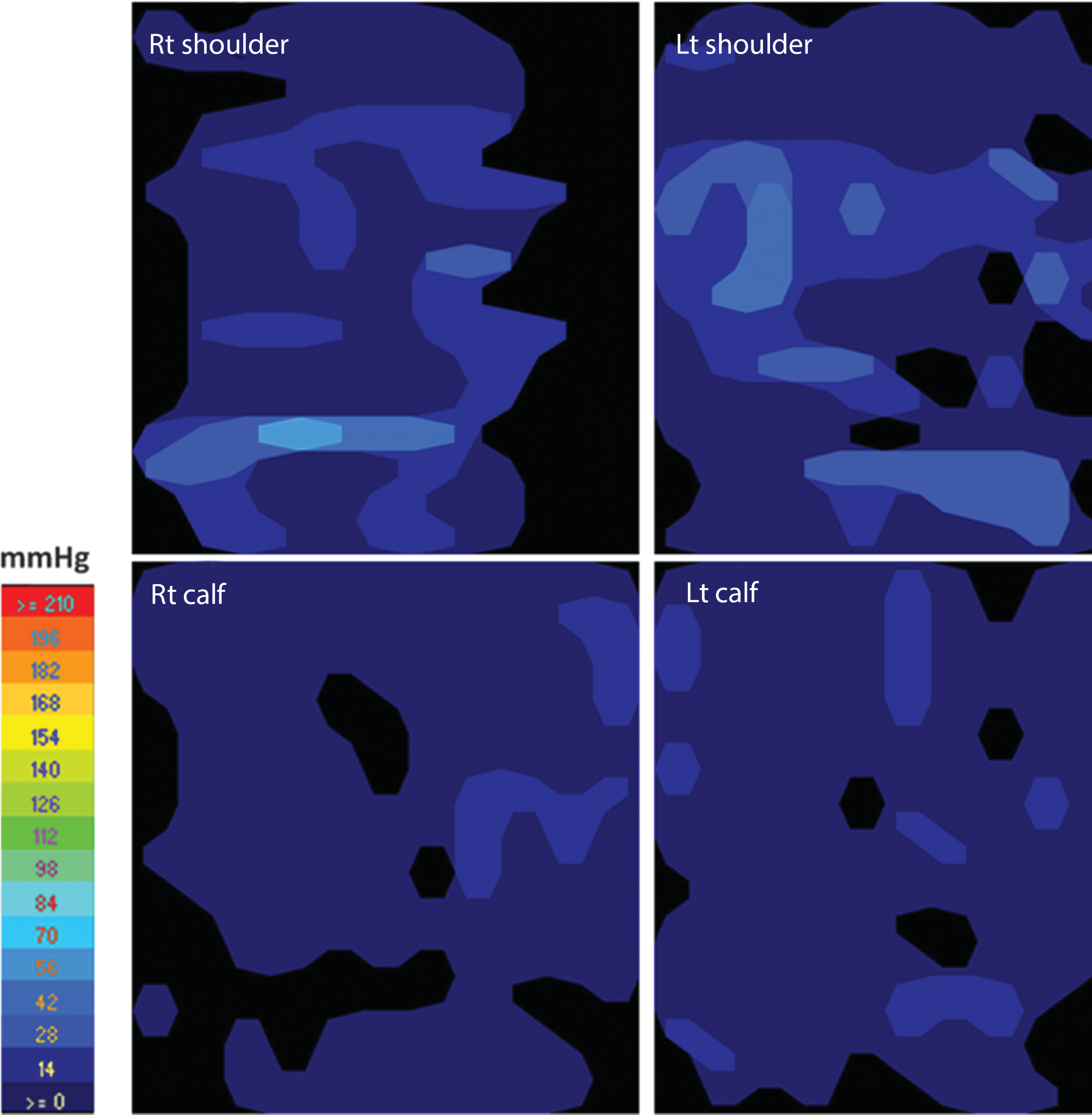
TekScan pressure sensor systems for real-time monitoring and mapping of the contact pressures and contact area over the shoulders and posterior calves.
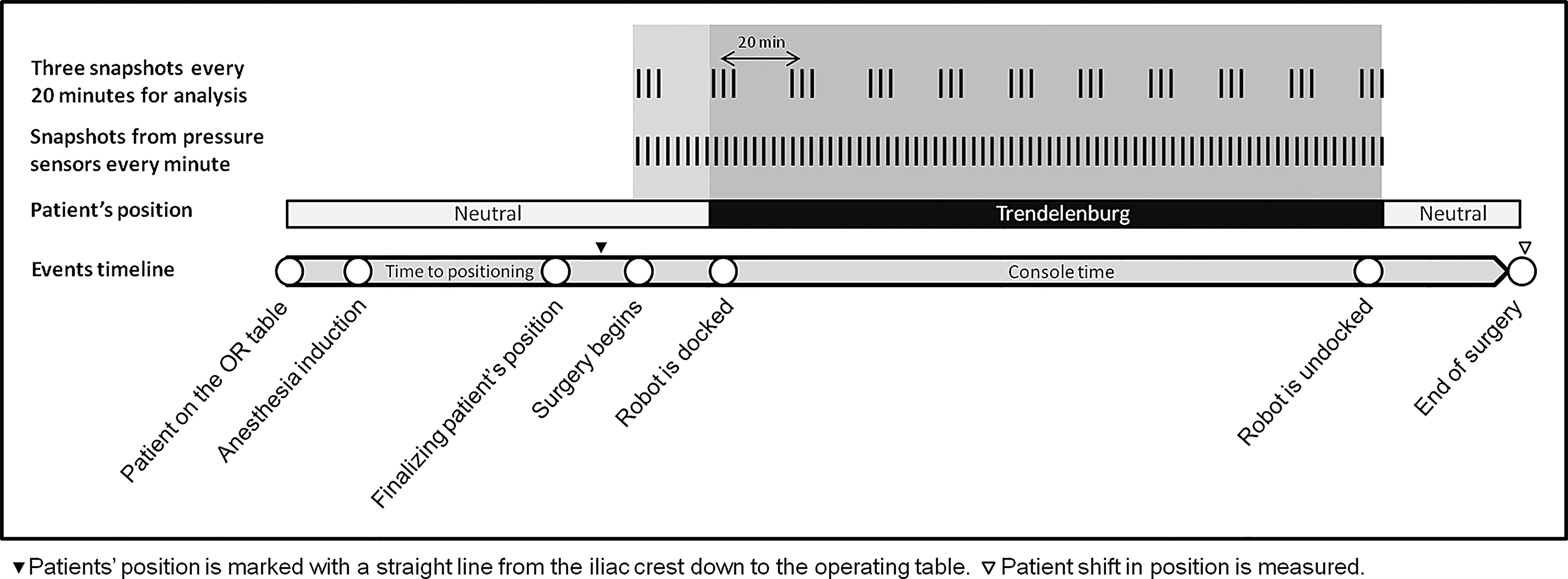
The timeline representing the event flow in the operating room.
To evaluate the patients' shifting distance on the operating table, the subjects' position was marked at the beginning of the surgery with a straight line from the iliac crest down to the operating table. At the completion of the procedure and on return to a neutral position, any shift in position was measured.
The subjects were followed at 2 hours, 1 day, and 1 month after the operation for signs of neurologic or musculoskeletal injuries related to positioning. Patients were asked and examined for neck, shoulder, or knee pain, numbness or tingling of the upper or lower extremities, and for any skin damage in dependent areas such as redness, abrasion, or blistering.
Data analyses
Statistical analyses were performed using SPSS statistical software (version 17.0). Wilcoxon signed-rank test was used for the comparison of contact pressure with area between different intervals. Correlation coefficients were Pearson's r-values. The results were considered significant only with a value of p < 0.05.
Results
From May 2013 to September 2013, 16 patients were enrolled in this study. Patients' demographic and perioperative characteristics have been summarized in Table 1. Median age of 56.5 years (11 male; 5 female), median BMI was 27.3, median positioning time was 6 minutes, duration of surgery was 3.5 hours, T-burg angle was 20°, and patient shift on the table was 1 cm.
T-burg = Trendelenburg.
There was no significant association between patients' shift and either BMI, T-burg angle, duration of T-burg position, or change in mean contact pressure.
Figure 4 shows the changes in interface contact pressure and contact area over the shoulders and calves during the surgery in the T-burg position. There was a statistically significant change in the mean contact pressure of the shoulders when comparing the pressure in neutral position and the last contact pressure measured in the T-burg position (13.12 ± 1.12 mm Hg vs 20.25 ± 1.56 mm Hg, p-value = 0.001, for right shoulder and 12.84 ± 1.05 mm Hg vs 19.60 ± 1.09 mm Hg, p-value = 0.001, for left shoulder). The maximum changes in mean contact pressure were reported during the first 40 minutes after starting the T-burg positioning and this was calculated as 82% and 84.8% of the change of the mean contact pressure for the right and left shoulders, respectively. There was no significant change in the mean contact area of the shoulders during the surgery (p-value = 0.305). The mean contact pressure before T-burg positioning and the last measurement during the T-burg position was 12.25 ± 0.73 mm Hg vs 13.15 ± 0.07 mm Hg for right calf (p-value = 0.066) and 12.75 ± 0.76 mm Hg vs 14.25 ± 0.78 mm Hg for left calf (p-value = 0.061), respectively. The mean contact area of the calves did not change significantly during the operation in the T-burg position (p-value = 0.152 and 0.806 for right and left calves, respectively).

Mean contact pressure and mean contact area over the right and left shoulders and calves. Thin lines represent measurements for each individual patient and the red thick line represents the average values of all patients.
The maximum contact pressure that was recorded in this study was 74 mm Hg, which was reported over the shoulder area in only one 2 cm × 2 cm pixel in one case at 200 and 260 minutes after beginning of T-burg positioning. However, the mean contact pressures at these time points for this patient were 25 and 26 mm Hg. This patient did not have any skin changes at the site of maximum pressure and did not complain of any pain or discomfort postoperatively.
There were no major postoperative complications related to the patients positioning. One patient complained of right shoulder pain 2 hours after her surgery. However, she reported no pain or discomfort 24 hours or 30 days later. There was no nerve injury, joint pain, and skin abrasions or discoloration detected during the postoperative follow-up.
Discussion
Robot-assisted laparoscopic surgery is rapidly becoming a common practice for procedures within the lower abdomen and pelvis. Safe patient positioning in T-burg is a challenge and concern for the operating room team. Patient positioning is a crucial presurgical step, with significant consequences if it is performed suboptimally. Despite an incredible research and investment on the surgical instruments and technology, such as robotics, we have not been able to standardize our positioning methods, yet. Furthermore, we do not have a universally accepted methodology to appropriately evaluate positioning devices. Current methods and devices used for patient positioning are suboptimal and have inherent risks. They can be time consuming to set up and do not prevent slippage and nerve damage in patients.
In our search to find an adequately studied positioning device for our robotic surgery procedures, we were surprised to find out that there are no peer-reviewed publications for most of the currently available devices to show their safety and efficiency before being introduced for clinical use. These devices do not need to obtain an FDA approval and most consumers do not ask for any safety study before acquiring them. In the current setting, surgeons and hospitals carry the liability burden for any positioning-related injuries. Position-related injuries are usually under-reported, hiding the magnitude of the problem. Understanding the status quo, we attempted to design a device and evaluate it based on some current accepted methodologies. This prospective pilot study is the first of its kind where continuous interface dermal pressures were used to demonstrate the reliability and safety inherent with the use of the SAF-R positioning device.
The study showed that the SAF-R board is safe, reliable, and efficient. We found some features to this design that are appealing. First, the surgeon now has full access to the entire abdomen and chest wall. Second, the anesthesiologist has full access to the arms for his intravenous lines. There is no need to wrap the patient's arms with sheaths or belts, therefore lowering the risk of upper extremity compartment syndrome. Third, the detachable upper back pieces allow the anesthesiologist to have full access to the patient's neck to place any neck lines or perform Cardiopulmonary resuscitation (CPR), should the need arise.
Prevention of slippage along with tension/compression-free positioning of the extremities during surgeries in steep T-burg are the most crucial components of an optimal positioning technique to ensure patient safety. In robot-assisted surgery after the robot is docked to the table, no movement of the patient is allowed. Any slippage in such situations increases the risk of abdominal wall injury, incisional hernia development, and/or trauma to the internal organs. 3 Movement may result in suboptimal positioning of the extremities and can result in nerve injury from stretching and compression. Positioning-related nerve injuries have been shown to occur in more than 6% of all robot-assisted urologic surgeries. 4 It is reassuring to find that the device allowed minimal movement (1 cm), matching the expected amount of movement for subcutaneous and soft tissue under physiologic pressure. In previous studies investigating the application of currently used positioning techniques, patient shifting of up to 7.5 cm has been reported. 3
The purpose of the SAF-R surgical board is to provide an easy, quick, and safe means of securing the patient during the extremes of T-burg position. The device helps decrease the tension on pressure points in the shoulders and lowers the risk of nerve injury incidents. The key component of the design is the proprietary upper back supports of SAF-R. They fix the board to the operation table and help stabilize the patient in a steep T-burg position and prevent the slippage. A number of published studies discourage the use of shoulder braces to prevent cephalad migration of patient. It has been shown that shoulder braces put the brachial plexus under severe stretch and compression and are associated with an increased risk of brachial plexus injuries. 6 –8 This is true particularly when the shoulder pads are placed medial to the acromioclavicular joint, causing direct compression of the nerve tracts and/or when the patient's arms are abducted, which drives the humeral head downward and stretches the brachial plexus, 9,10 This critical point has been considered and addressed in the design of the SAF-R board by following the body's natural curvatures. The upper back support is connected to the main board and follows the curve of the back over the patient's scapula and does not go above the shoulder zone; this helps to distribute the pressure from body weight over a larger area on both sides and prevents high focal pressures over the shoulders, which can result in nerve compression. On the other hand, the upper back supports cover all the way from the tip of the scapula to the acromion process, but not the acromioclavicular joint, and that helps to prevent pressure transduction to the joint and subsequent compression of the nerve tracts traveling under it (Fig. 5). Moreover, the arms are tucked to the patient's sides using toboggan arm boards with the palms facing the thighs, which puts the humeral head in a neutral position and prevents stretching of the brachial plexus.
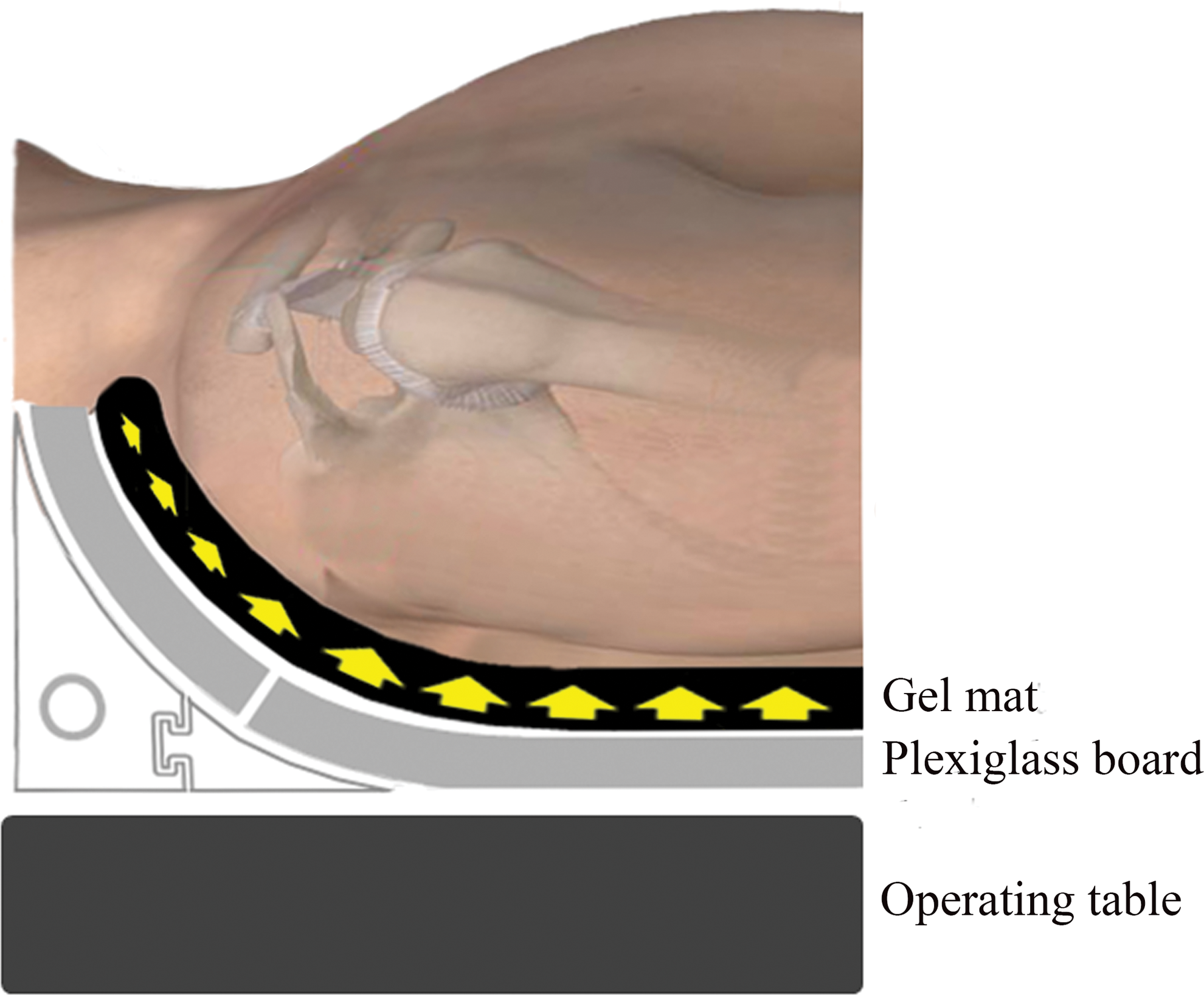
Schematic representation of the upper back supports. The upper back support is connected to the main board and follows the curve of the back over the patient's scapula; this helps to distribute the pressure from body weight over a larger area on both sides and prevents high focal pressures over the shoulders. The upper back supports cover all the way from the tip of scapula to the acromion process, but not the acromioclavicular joint, and that helps to prevent pressure transduction to the joint and subsequent compression of the nerve tracts traveling under it. Color images available online at
The results from this study show that the SAF-R surgical board was able to keep the patient's position stable with minimal slippage at the end of the operation. This was consistent for all 16 cases that were evaluated in this study with a maximum weight of 113 kg and maximum BMI of 34.1.
The shoulder pressure sensors show that the maximum change in mean interface pressure happened right after changing the patient's position to T-burg, after which the contact pressure became stable throughout the surgery. Furthermore, there is no significant change in mean contact area over the shoulders. This indicates negligible cephalad shifting of the patient. The mean interface pressure and mean contact area from the calves' sensors also show no significant change during the operation, which represents minimal tension on lower extremities and hip and knee joints.
Theoretically, when the skin interface pressure exceeds the mean capillary pressure (32 mm Hg), tissue ischemia and skin injury may occur. 11 However, it has been shown that with an interface pressure of less than 80 mm Hg and good pressure distribution, skin injuries are unlikely. 12 The real-time pressure mapping in this study showed that the mean contact pressure in dependent areas was below 21 mm Hg with a maximum point pressure of 74 mm Hg during the surgery, which is reassuring. It is noteworthy that in our study, no acute or late dermatologic complication related to the patients' positioning, including skin abrasion, discoloration, or blisters were reported. Moreover, no neurologic complication or clinically significant musculoskeletal pain has occurred.
Alternate positioning methods often necessitate the padding and wrapping of the arms and upper torso to secure the patient's position, which restricts access to the arms and chest, which is challenging for the anesthesia team, particularly in the case of emergency. Using the SAF-R board, the upper extremities and the chest remain accessible during the entire case, an added benefit of this positioning technique. Moreover, pressure from gel mats across the chest and the use of adhesive tape can constrain chest expansion and theoretically interfere with optimum ventilation when in the T-burg position; this can be avoided by using an SAF-R positioning board.
The current required time for positioning patients for robot-assisted operation has been reported to take up to 1 hour before the actual surgery. 13 This is valuable operative and anesthesia time that were being wasted in the past. A major advantage of the SAF-R board is the fact that the patient will be positioned for surgery before induction of anesthesia and while still awake. The patient will be able to give feedback regarding any pressure sites or any discomfort with his/her positioning that could be instantly corrected. This makes patient positioning easy to achieve following induction of anesthesia. Our findings show that the application of SAF-R positioning board is extremely timesaving, and it takes only four to eight minutes in most patients to finalize the positioning. During this time, the anesthesia team simultaneously prepares the patient for induction. Therefore, there is no added time in the operating room when preparing the patient positioning. This can reduce operating room costs and anesthesia time.
This study also has some limitations. This was a pilot feasibility study, and the number of patients in this cohort was fairly small to draw any firm conclusions. This only helps to introduce a set of vigorous measures to assess our positioning devices before using them in clinical settings. Moreover, only patients weighing less than 250 lbs. were included in this study, in accordance with the recommendation of the manufacturing team. The number of patients weighing close to 250 lbs is limited, mainly because the design of the study allowed for the recruitment of 16 consecutive patients. Due to both the promising outcome of this study and further safety testing of the SAF-R board, we currently effectively use the device for patients weighing as much as 370 lbs. Certainly, this needs to be studied on a bigger scale to prove its efficacy in patients with high BMIs.
The other limitation is the lack of a control group in this study to compare data with. These limitations necessitate further trials that include a larger cohort of patients, as well as control groups.
Conclusion
This pilot study shows that the SAF-R surgical board is a safe, reliable, and time-saving positioning device for patients undergoing robotic pelvic surgery in the steep T-burg position. We believe that this device has a valuable role in the operating room where such surgery is performed and will set a new standard in patient-positioning safety for operations requiring the steep T-burg positioning.
Footnotes
Author Disclosure Statement
Dr. Sarma and Dr. Tabatabaei have applied for a U.S. patent. For the remaining authors, no competing financial interests exist.