
Abstract
Introduction:
The internal structure of renal calculi can be determined on CT using bone windows and may be classified as homogeneous or inhomogeneous with void regions. In vitro studies have shown homogeneous stones to be less responsive to extracorporeal shockwave lithotripsy (SWL). The objective was to evaluate whether the internal morphology of calculi defined by CT bone window influences SWL outcome in vivo.
Materials and Methods:
One hundred eleven patients with solitary renal calculi treated with SWL were included. Treatment data were registered prospectively and follow-up data were collected retrospectively. All patients had noncontrast computed tomography (NCCT) performed before SWL and at 3-month follow-up. The stones were categorized as homogeneous or inhomogeneous. At follow-up, the patient's stone status was registered. Stone-free status was defined as no evidence of calculi on NCCT. Treatment was considered successful if the patient was either stone free or had clinically insignificant residual fragments.
Results:
Using simple logistic regression, the odds for being stone free 3 months post-SWL were significantly reduced in the patients with inhomogeneous stones compared with patients with homogeneous stones (odds ratio 0.43 [95% confidence interval 0.20, 0.92; p < 0.05]). However, when adjusting for stone size by multiple logistic regression, including stone size (area) as a covariate, this difference became insignificant.
Conclusion:
The internal structure of kidney stones did not predict the outcome of SWL in vivo.
Introduction
E
Materials and Methods
A retrospective study was performed of consecutive patients undergoing SWL (Storz Medical Modulith® SLX F2) at the Department of Urology, Lillebaelt Hospital, University of Southern Denmark, Denmark, from March 2011 to February 2014. The inclusion criteria were adult patients with solitary renal calculi treated with SWL and in whom noncontrast computed tomography (NCCT) had been performed both before SWL and at follow-up to achieve the most accurate and objective judgment of outcome.
Before SWL, NCCT was performed, defining localization, size, and HUs of the stone. HU was measured on the smallest slice thickness (0.625–3 mm) at axial series. We used window settings at soft tissue as well as bone tissue to evaluate the stone. To minimize partial volume averaging with surrounding tissues, the diameter of the region of interest used for attenuation measurement was standardized at approximately one-half the diameter of the stone. 1 The internal morphology (homogeneity) of the calculi was evaluated on CT bone window with magnification and described as homogeneous or inhomogeneous (Fig. 1). Inhomogeneous kidney calculi have visible internal void regions present on NCCT. 6
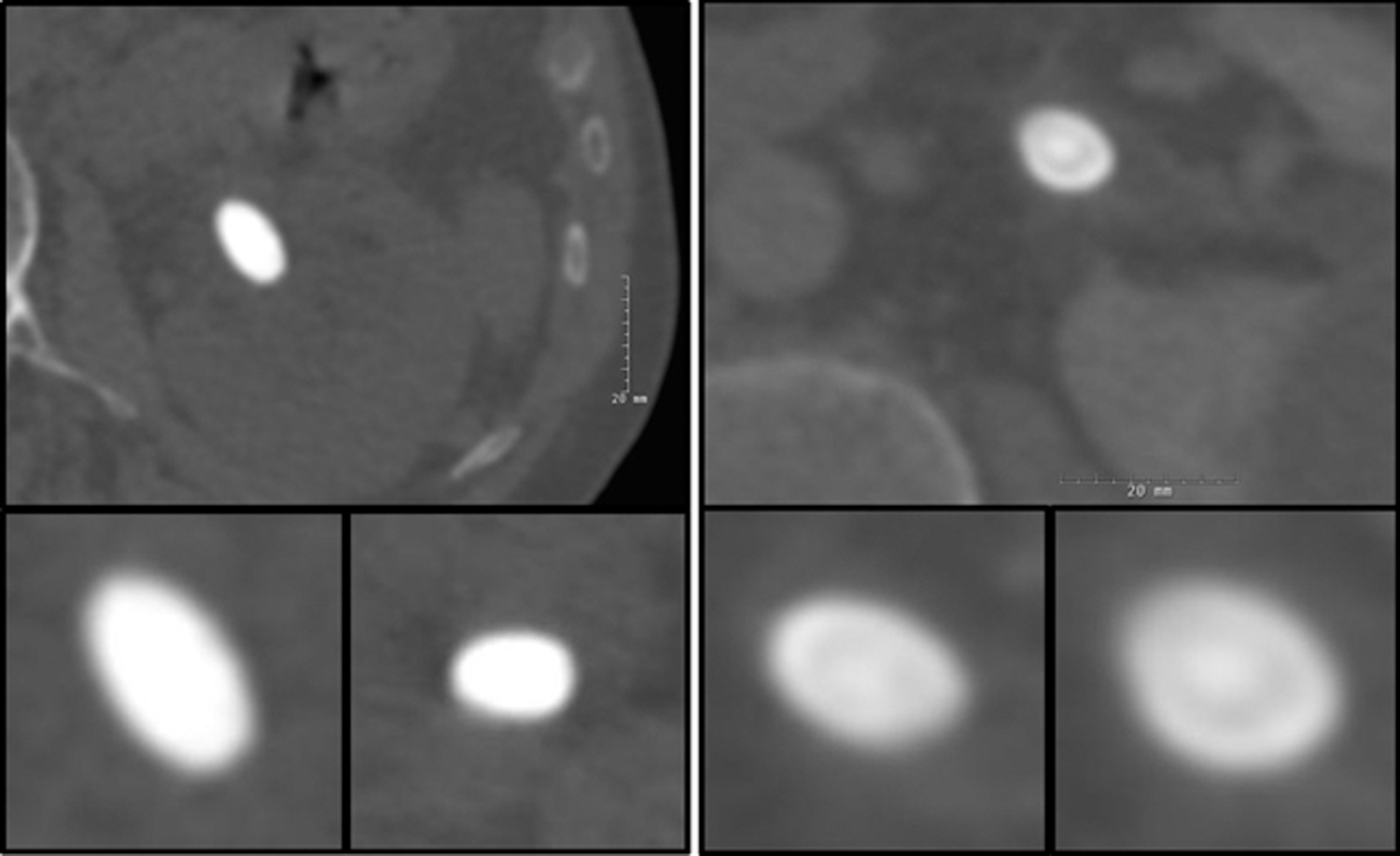
Left: Examples of homogeneous stones. Right: Examples of inhomogeneous stones with void regions.
An experienced technician and an experienced urologist or uroradiologist performed the treatments. Flouroscopy and/or in-line ultrasonography was used for stone targeting. Data from each treatment were prospectively registered in the patient's medical journal. Data included total number of shock waves, frequency, focal size, maximum energy level, and total energy expressed as Storz Medical Lithotripsy Index (SMLI).
SWL was performed on an outpatient basis and all the patients except one were given intravenous analgesia with Remifentanil (Ultiva®). Patients with ureteral stents, nephrostomy tubes, or a history of urinary tract infection received antibiotics intravenously. All patients were initially selected for SWL without considering homogeneity of the calculi, and outcome was registered. Subsequently, the stones were graded as homogeneous or inhomogeneous based on the criteria described without knowledge of outcome. Outcome was assessed 3 months post-SWL by NCCT. Auxiliary procedures and retreatments were recorded, and efficiency quotient (EQ) calculated. 7
Definitions
Stone free was defined as totally stone free with no evidence of residuals on NCCT. Clinically insignificant residual fragments (CIRFs) were defined as residual fragments ≤4 mm in noninfected patients with no symptoms. Treatment was defined successful if the patient was either stone free or had CIRFs. Patients who did not meet these criteria were considered treatment failures.
Data were retrospectively collected by systematic review of the patient's medical records. The radiological stone data were collected from the patient's NCCT. Stone area was calculated as length × width × π × 0.25.
Statistics
For comparing patient characteristics (sex, age) and stone characteristics (stone size, density, morphology) between the two groups, we used the Wilcoxon rank-sum test. Simple as well as multiple logistic regressions were used to compare success between the two groups. To compare the stone-free rate (SFR) and success rate (SR), we used the chi-square test. Stone analysis data were compared by use of Fisher exact test. Statistical analyses were performed using STATA 13.
Results
The study included 111 consecutive patients with solitary kidney calculi; 61 males and 50 females. The median age was 51 years (range: 21–88 years). Characteristics of the two groups are presented in Table 1, including distribution of stones in the different calices. Importantly, the number of stones in the lower calix was comparable between the two groups.
BMI = body mass index; SMLI = Storz Medical Lithotripsy Index.
Stone size was larger in the group with inhomogeneous stones compared with homogeneous stones: area was median 66 mm2 (95% confidence interval [CI]: 47, 79 mm2) vs 33 mm2 (95% CI: 25, 44 mm2) (p < 0.001) and the largest diameter of the stone was median 10 mm (95% CI: 10, 12 mm) vs 7 mm (95% CI: 7, 9 mm) (p < 0.001). There was no difference in the highest measured HU between the group with inhomogeneous stones (median: 988 [95% CI: 826, 1031]) and the group with homogeneous stones (median: 1000 [95% CI: 860, 1138]; p > 0.05). In the homogeneous group, the HUs of course were almost equal throughout the stone, whereas in the inhomogeneous group, HUs varied considerably within the individual stone. The retreatment rate (re-SWL or endoscopy) was comparable in the two groups (26% vs 25%; p > 0.05).
With the definition of stone free = totally stone free, the EQ was 30% (standard error [SE] = 6%) vs 48% (SE = 7%) for inhomogeneous vs homogeneous stones. When including CIRFs in the definition of stone free, the EQ was 47% (SE = 7%) vs 61% (SE = 7%).
Using simple logistic regression, the odds for being stone free 3 months post-SWL were significantly reduced in the patients with inhomogeneous stones compared with patients with homogeneous stones (odds ratio [OR] = 0.43 [95% CI: 0.20, 0.92; p < 0.05]). However, when adjusting for stone size by multiple logistic regression, including stone size (area) as a covariate, this difference became insignificant. Linearity of the continuous covariate stone size was checked by the LOWESS method.
The odds for achieving the criteria of success tended to be lower in the group with inhomogeneous stones; however, this difference was not statistically significant: OR = 0.49 (95% CI: 0.21, 1.12; p = 0.09). When adjusting for stone size, the trend of a difference in SR disappeared (OR = 0.66; p = 0.36) (Table 2).
SFR: Stone free was defined as totally stone free with no evidence of residuals on NCCT. SR: Treatment was defined successful if the patient was either stone free or had clinical insignificant fragments (<4 mm) on NCCT.
Adjusted for stone size by multiple logistic regression.
SFR = stone-free rate; SR = success rate; NCCT = noncontrast computed tomography.
Discussion
To optimize the treatment of kidney calculi, pretreatment analysis of the patient and stone is important to select the right treatment for the right patient. As a predictor for a successful outcome of SWL, the internal structure or morphology of the calculi has been suggested. In vitro studies on cystine and COM calculi showed that stones appearing inhomogeneous on CT imaging required fewer shock waves to be fragmented than the stones that appeared homogeneous. 4,5 This was not true for brushite calculi, in which only brushite content and stone density correlated with stone fragility. 8 In our study, the odds for patients with inhomogeneous stones to become stone free and achieve the criteria of success compared with patients with homogeneous stones were comparable when adjusted for stone size, thus the internal structure of the stone did not seem to predict fragility.
Patients with a variety of different stone compositions were included in the present study. Stone analysis (infrared spectroscopy) was performed in 42% of the patients. In the group with homogeneous stones, there were significantly more COM stones (p = 0.006). Although stone analysis was not available in all patients, our results are contradictory to the results of the in vitro studies. 3 The reason for this finding is unclear, and an explanation can only be speculative. A possible explanation could be that the inhomogeneous stones were less visible on fluoroscopy after initial fragmentation, thereby escaping subsequent fragmentation. The higher percentage of COM stones in the homogeneous group cannot explain our results. On the contrary, since COM stones are considered to be SWL resistant, one might have suspected a lower SFR in the homogeneous group. Our results seem to correlate better with in vitro data on brushite stones, in which it was found that SWL fragility did not correlate with internal structure discernable using helical CT. 8
An SSD <9 cm has been suggested a predictor for successful SWL outcome. 1,9 We did not register SSD. In our series, there was, however, no difference in body mass–index (BMI) between groups, indicating that differences in SSD probably were not the cause of the differences in outcome between the groups.
An important limitation of the present study was that the homogeneous stones were significantly smaller than the inhomogeneous stones. Knowing that stone size has a powerful impact on stone breakage, this may have influenced the results. 10 Furthermore, since it is more difficult to identify the internal structure in smaller stones, this finding may have influenced our classification of the stones being either homogeneous or inhomogeneous. A more gradual scale of homogeneity may give a better picture of the link between fragility and stone morphology. Furthermore, automated processing of CT images may provide a more objective scale for defining differences in inner stone structure.
Conclusion
In the present study, we were not able to show that the internal structure of kidney stones predicts the outcome of SWL in vivo.
Footnotes
Acknowledgment
Statistician René dePont Christensen is thanked for support in the statistical analysis of the data.
Author Disclosure Statement
No competing financial interests exist.