
Abstract
Purpose:
To describe our initial experience with confocal laser endomicroscopy (CLE) for the evaluation and treatment of patients with upper urinary tract transitional cell carcinoma (UUT-TCC).
Materials and Methods:
Preliminary data were analyzed from 11 patients with suspicion of UUT-TCC scheduled for flexible ureteroscopy (f-URS) and consensual holmium-YAG laser tumor ablation. CLE was performed before endoscopic biopsy and laser photoablation of the suspected lesion using a 3F-diameter flexible probe UroFlex™ B (Cellvizio® system; Mauna Kea Technologies, Paris, France), which allows to obtain microscopic resolution imaging (3.5 μm), with a field of view of 325 μm and a depth of tissue imaging of 40 to 70 μm. Video sequences were analyzed offline and thereafter compared with histopathologic findings.
Results:
CLE technique was feasible and showed good quality imaging in all patients. Overall, the Cellvizio system provided reliable images of healthy urothelium when the probe was pointed toward normal tissue, showing umbrella cells on the surface and vessels in the lamina propria. Moreover, CLE displayed the characteristic features of high-density cellular aggregates and fibrovascular stalks in four patients with pathologically confirmed low-grade UUT-TCC. In the patient with pathologically confirmed high-grade UUT-TCC, more distorted microarchitecture and tortuous vessels were clearly recognized with CLE.
Conclusions:
These preliminary data showed the feasibility of CLE technique when applied to the diagnosis of UUT-TCC. Further clinical studies are required to confirm CLE accuracy in distinguishing healthy urothelial tissue from malignant lesions, thus helping clinicians in targeting ureteroscopic biopsy and improving the conservative management of UUT-TCC patients.
Introduction
M
In this context, the development of technology and the miniaturization of the equipment have made flexible ureteroscopy (f-URS) with holmium-YAG laser photoablation the ideal compromise between the possibility of offering a definitive radical treatment while reducing surgical morbidity and renal function impairment. 2 –6
However, some issues still need to be improved for optimizing the endoscopic treatment of UUT-TCC. The major shortcomings are represented by the difficulties in distinguishing small-size and flat-shape malignant urothelial carcinoma from inflammatory lesions and in obtaining adequate sample of tissue for the histopathologic analysis. 7,8 While enhanced imaging techniques (i.e., Narrow Band Imaging system, photodynamic diagnosis with 5-aminolevulinic acid) and real-time optical coherence tomography (OCT) have been proposed to help surgeons increase the accuracy of white light inspection not only in the diagnosis of bladder cancer but also in the context of UUT-TCC, 9,10 real-time confocal laser endomicroscopy (CLE), providing in vivo microscopic histology images of the tissue exposed to a fluorescent dye by using a low-energy laser light source, could represent a further step to overcome concerns related to the reliability of ureteroscopic biopsy. 11 This innovative technology was initially used in the endoscopic management of gastrointestinal and bronchial pathologies 12,13 and has been recently studied in the context of bladder cancer diagnosis. 14,15 Interestingly, CLE has been preliminary tested for evaluating patients with UUT-TCC, 16 although no full report is available in the literature on this topic. In the current study, we sought to (1) evaluate the feasibility of using CLE in the context of conservative management of UUT-TCC and (2) discuss CLE imaging quality in comparison with the histopathologic analysis and previous CLE findings obtained in patients with bladder cancer.
Materials and Methods
Between March and September 2014, f-URS with CLE was performed in 11 consecutive patients at a single tertiary care referral center. Of all patients, four (36.4%) patients had been previously treated with f-URS combined with laser photoablation for UUT-TCC; therefore, they were included in the study as a part of their regular endoscopic follow-up. Conversely, six (54.5%) patients were included after the discovery of suspected UUT-TCC at conventional imaging (CT scan). Finally, one (9.1%) patient was referred for CLE due to the presence of positive urine cytology with no suspected bladder lesion at cystoscopy.
Endoscopic technique and in vivo CLE
Due to the differences in terms of quality of view, 17,18 a digital ureteroscope [Flex-XC; Storz, Tuttlingen, Germany, (8.5F) and URF-V; Olympus Surgical, Orangeburg, NY (10.9F)] was preferred to fiber-optic ureteroscope for performing f-URS in all the patients. We used ureteral access sheath (10/12F when we used Flex-XC or 12/14F when we used URF-V) to facilitate the access to renal cavities and to enhance backflow during the procedure and reduce overpressure in the kidney. An initial inspection of the renal collecting system was performed in white light to macroscopically identify all potential suspicious lesions.
CLE was then performed using the Cellvizio® system (Mauna Kea Technologies, Paris, France) according to the following protocol: 3 to 5 mL of 0.1% fluorescein was injected into the renal cavities and left indwelling for 5 minutes. A 3F-diameter probe (UroFlex™ B), which guarantees a 3.5 μm resolution, a field of view of 325 μm, and a depth of tissue imaging of 40 to 70 μm, was inserted through the working channel of the ureteroscope and then placed in contact first with the apparently normal urothelium and thereafter with the lesions suspicious for UUT-TCC. Real-time video sequences were acquired at 12 frames per second allowing micron-scale resolution of the area of interest by placing the probe perpendicular to and in contact with the tissues. An endoscopic biopsy of suspected lesion was then performed. Finally, laser photoablation was adopted to achieve a complete ablation of the tumor.
Image selection and comparison with histologic evaluation
After being registered, the in vivo video sequences were analyzed offline to identify the most significant images suggestive for malignancies. Because CLE has never been systematically tested in the evaluation of the upper urinary tract, current findings have been evaluated on the basis of the results previouslyreported using CLE in the diagnosis of bladder cancer. 19 All specimens were examined by the same dedicated genitourinary pathologist. The information obtained with CLE was compared with the corresponding histologic findings afterward.
Results
Patient characteristics are described in Table 1. A diagnosis of noninvasive papillary urothelial tumor was made at histopathologic examination in five (45.4%) patients (four patients with a newly diagnosed UUT-TCC and one patient on a regular follow-up regimen, respectively). Tissue specimens resulted positive for high-grade and low-grade tumors in one (9.1%) and four (36.4%) patients, respectively. The histopathologic results from the remaining six patients showed either dysplastic alterations or tissue inflammation in one (9.1%) patient each; in contrast, the samples of the last four (36.4%) patients resulted not reliable due to the small size of the specimens.
CLE = confocal laser endomicroscopy; f-URS = flexible ureteroscopy; NMIBC = nonmuscle-invasive bladder cancer; RNU = radical nephroureterectomy; UUT-TCC = upper urinary tract transitional cell carcinoma.
Overall, CLE provided reliable images of healthy urothelium when the probe was pointed toward normal tissue, thus depicting superficial cells of different size, probably corresponding to the larger umbrella cells of the surface (Fig. 1A) and the smaller intermediate cells of the deeper layer (Fig. 1B). By applying soft pressure with the probe on the normal urothelium, the typical structures of lamina propria, such as connective tissue and vascular network, were eventually observed (Fig. 1C).

Endomicroscopic images of normal urothelium depicting the larger monomorphic-shape umbrella cells
When looking at the five patients with a pathologically confirmed UUT-TCC, CLE provided good quality images depicting urothelial cancer features similar to those previously described in the CLE imaging atlas of urothelial cancer by Wu et al. 19 When the probe was placed in contact with the polypoid lesion, characteristic features compatible with low-grade tumor, including densely packed homogeneous and monomorphic urothelial cells with papillary structure and fibrovascular stalks, were visualized (Fig. 2A–C) in a half of patients with low-grade tumors. In the patient with a pathologically confirmed diagnosis of high-grade UUT-TCC, the analysis of video sequences revealed the presence of more densely packed, urothelial irregularly shaped cells with distorted microarchitecture, indistinct cell borders, and tortuous fibrovascular stalks (Fig. 3A–C).
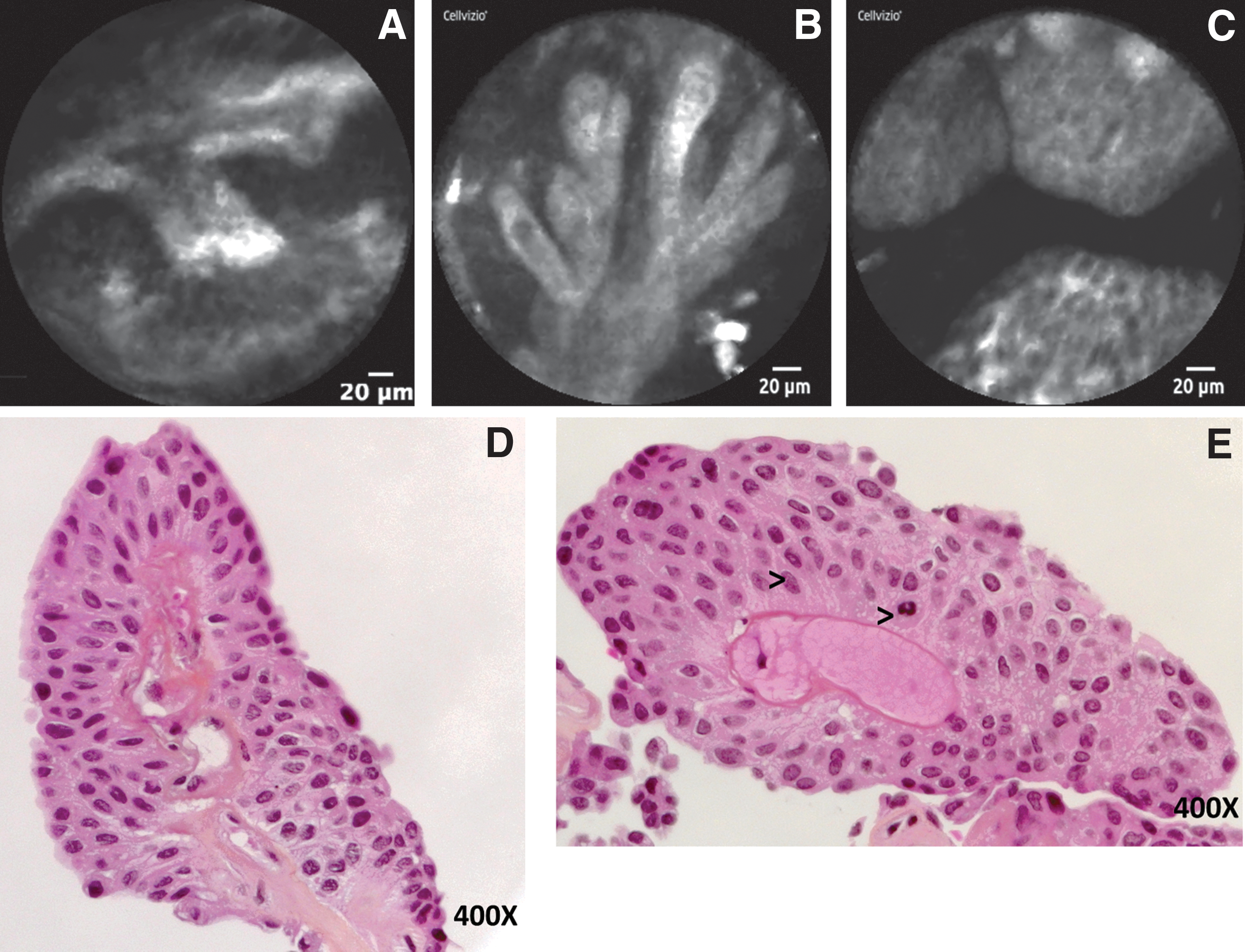
Endomicroscopic images of low-grade papillary urothelial tumor depicting longitudinally cellular aggregates arranged uniformly around fibrovascular stalks
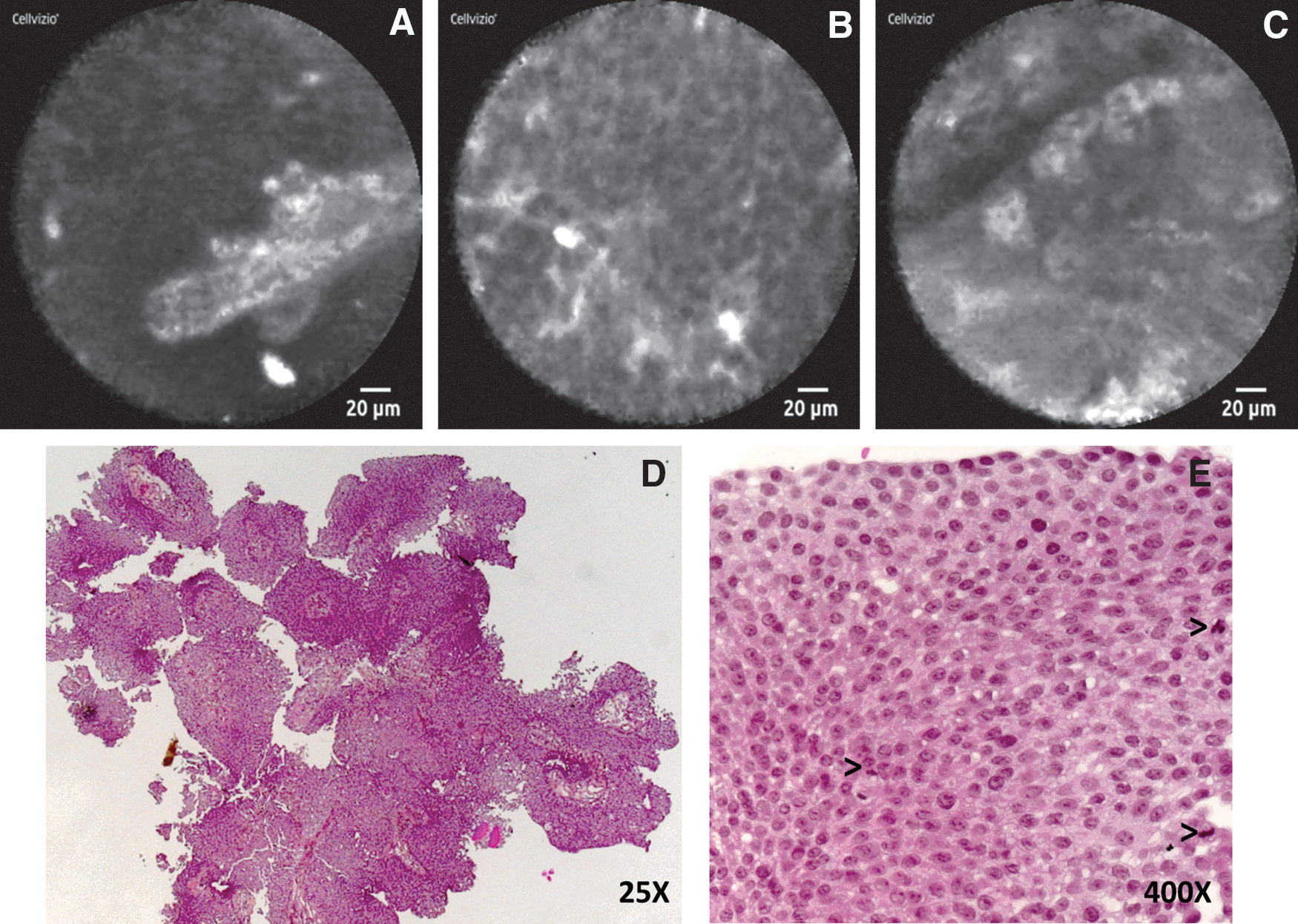
Endomicroscopic images of high-grade papillary urothelial tumor depicting dismorphic cellular aggregates with distorted microarchitecture and indistinct cell borders
Moreover, CLE allowed to obtain images compatible with malignant tumors even in the four patients for whom biopsy results were not valid and in the patient with dysplastic alterations. The patient with inflammatory alterations at biopsy had normal urothelium at CLE as well, with enlarged vessels in the lamina propria (Fig. 1D).
Intracellular details and nuclear morphology were not visible because of the lack of permeability of the cell membrane to fluorescein, which only stained extracellularly.
No patients experienced systemic toxicity events from intrarenal injection of fluorescein, and no hypersensitivity reactions were observed in the perioperative. Maneuverability of the ureteroscope was not impaired by the presence of the probe into the working channel. Fluorescein staining of the urothelial structures allowed acquisition of CLE imaging for roughly 5 minutes; subsequently, fluorescein was washed out by the active irrigation system and the quality of CLE video sequences diminished.
Discussion
The results of the current study showed that the acquisition of CLE of the upper urinary tract is safe, reliable in terms of imaging quality, and it does not impair the maneuverability of the ureteroscope. The fluorescein staining of the urothelial structures remained detectable for ∼5 minutes, which represented an adequate time to acquire good quality CLE imaging.
Similar to what described for the lower urinary tract, 19 normal urothelium and malignant tumors are characterized by different specific features at CLE. While healthy tissue appeared as a uniform polygonal-shaped cell layer with capillary networks (Fig. 1A–C), macroscopic neoplastic lesions detected using white light ureteroscopy appeared as high-density cellular aggregates surrounding a fibrovascular core (Fig. 2A–C). Moreover, some lesions were also characterized by distorted microarchitecture with irregularly shaped cells, indistinct cell borders, and tortuous vessels (Fig. 3A–C). Unfortunately, a real estimation of the sensitivity and the specificity of the technique was not possible due to the lack of a complete histopathologic confirmation. Indeed, biopsy findings could not be considered representative of the real pathologic stage and grade of the disease because they consisted of a limited portion of the lesion only. However, several advantages may be derived by using CLE in UUT-TTC patients suitable for conservative management; if further studies compare in vivo CLE imaging of the whole collecting system with histologic findings of patients, candidates to nephroureterectomy will confirm the efficacy and the reliability of such a technique.
First, taking an endoscopic biopsy of the upper urinary tract could be difficult to perform, especially in the presence of small-size or flat-shape suspected lesion. Second, although it results feasible, the amount of tissue obtained with forceps may not be sufficient for obtaining a reliable histopathologic analysis, as reported in 4 of 11 patients of the current study and consistently with data available in the literature, where up to 25% of upper urinary tract biopsies are not diagnostic because of the inadequate tissue. 20 Furthermore, the CLE probe can explore the whole surface of an extended lesion too, thus allowing to entirely characterize its microscopic details and specific features, while bioptic specimens of suspected UUT-TCC are necessarily the picture of a limited area. These observations could explain why in the current study CLE allowed to obtain images compatible with malignant tumors, even in those patients for whom biopsy results were not valid or compatible with dysplastic alterations only, and to identify foci of high-grade cancer, even in two patients with a pathologically confirmed diagnosis of low-grade cancer (Table 1).
Finally, we can hypothesize that if urologists were able to interpret in vivo and in real time the CLE imaging during f-URS, thus identifying the area with features compatible with high-grade cancer and tumor boundaries, they could immediately take advantage from such a technology by targeting the site of biopsy and the laser photoablation. Unfortunately, this evaluation could not be assessed in the current preliminary report and could be the subject for further investigations.
The possibility of better characterizing the real nature and aggressiveness of the disease may consequently help clinicians in the clinical decision-making process, mainly represented by the option of carrying on a conservative treatment rather than advocating a radical surgery.
As reported in some studies dealing with the role of CLE in the diagnosis of bladder cancer, 19,21 current findings could represent the basis for further studies to validate a complete atlas of CLE imaging in a larger cohort of UUT-TCC patients and to prospectively evaluate the interobserver level of agreement regarding variations in the interpretation of real-time CLE, thus determining the accuracy and confirming the reliability of such a technique even when applied in the diagnosis of upper tract malignancies.
Conclusions
These preliminary data showed for the first time that CLE imaging represents a feasible technique for the endoscopic investigation of patients affected with UUT-TTC. The Cellvizio system provided good quality imaging of both healthy urothelium and urothelial cancer, with specific features that distinguish low-grade from high-grade tumors. Larger cohort of patients are required to validate the use of CLE imaging in this field and to create an imaging atlas. If confirmed by further studies, this technology might improve the accuracy of the available current tools to diagnose and characterize stage and grade of upper urinary tract malignancies, thus potentially improving the patient selection and the outcome of conservative treatment in patients with UUT-TCC.
Footnotes
Author Disclosure Statement
No competing financial interests exist.