
Abstract
Introduction:
Robotic technology has been increasingly utilized for complicated reconstructive surgeries in pediatric urology, such as ureteroureterostomy (UU). The literature is limited regarding the performance of minimally invasive UU in children, and the existing published series utilize indwelling ureteral stents. We sought to report on our pediatric experience with robot-assisted laparoscopic (RAL)-UU using a temporary ureteral catheter in duplex systems with ureteral ectopia.
Methods:
A retrospective chart review was performed of all pediatric patients who underwent RAL-UU at a single institution over a 2-year period. An externalized ureteral catheter was kept overnight and removed with the indwelling catheter on postoperative day 1. Intraoperative as well as postoperative complications, length of stay (LOS), and analgesia were recorded. Follow-up renal ultrasound (US) and evaluation for symptom resolution were completed 3 months postoperatively.
Results:
Twelve patients (four male, eight female) underwent RAL-UU at a mean age of 19.4 months (range 9–48 months) during the study period. The majority of patients (83.3%) presented with hydronephrosis, and all were found to have duplicated systems with ureteral ectopia. No child had ipsilateral vesicoureteral reflux. Two children had bilateral duplicated systems, one of which required bilateral surgery. Median operative time was 138 minutes (IQR 119–180 minutes), and mean estimated blood loss was 1.5 mL. There were no intraoperative complications, and no case required open conversion. Median hospital LOS was 31 hours (IQR 30–39 hours). Median follow-up time was 11 months (range 3–22 months). One patient developed a postoperative febrile upper respiratory infection. All patients had improved hydroureteronephrosis on US at 3 months postoperatively. One patient with preoperative urinary incontinence was dry postoperatively. Therefore, the overall success rate was 100%.
Conclusion:
Our institutional results demonstrate that RAL-UU utilizing a temporary ureteral catheter is a safe and effective technique for managing duplicated, ectopic ureters in children and infants.
Introduction
U
The expansion of minimally invasive surgical techniques in reconstructive pediatric urology has led to several reports from investigators demonstrating excellent clinical outcomes utilizing both upper and lower tract laparoscopic procedures. 1 –6 Although heminephrectomy is the most commonly performed upper tract approach, it has been associated with loss of renal function in the remaining ipsilateral moiety in as much as 5% of patients, which is likely due to vascular injury or torsion of the renal pedicle from extensive renal mobilization. 7 In comparison, UU is considered by some to be a safer procedure. Although UU has traditionally been reserved for children with a functional upper moiety and absent ipsilateral VUR, UU is becoming more common for the management of duplex anomalies irrespective of functionality or reflux. 7 –9 However, the widespread application of laparoscopic UU may be limited due to technical difficulties, particularly with intracorporeal suturing.
Robot-assisted laparoscopic (RAL) surgery has increasingly been utilized for complex reconstructive surgeries in pediatric urology and minimizes the challenges associated with traditional laparoscopic surgery. Limited literature exists that evaluates RAL-UU in the pediatric and infant populations. 4 –6,10 –17 Given the paucity of pediatric reports evaluating the use of RAL surgery for management of ureteral duplication with ectopia, we present our pediatric experience with RAL-UU, noting our unique approach of employing a ureteral catheter that is removed in the immediate postoperative period.
Patients and Methods
We performed an Institutional Review Board-approved, retrospective review of all pediatric patients who underwent RAL-UU by two pediatric urologists at a single institution during a 2-year period, from March 2013 to March 2015. Demographic data were recorded, including age, sex, height, and weight. All patients included in this study had pathology notable for a duplicated collecting system with ureteral ectopia. Preoperative investigation included imaging with ultrasound (US) and voiding cystourethrogram (VCUG). Ipsilateral lower pole ureteral VUR was considered a contraindication to RAL-UU. On US, hydroureteronephrosis (HUN) was graded as mild, moderate, and severe by evaluation of the renal parenchyma of the upper pole and the degree of ureteral dilation. By Society for Fetal Urology grading, all patients had grade 3 to 5 hydronephrosis but this system was not utilized because it does not account for dilation of the ureter. Ureteral dilation was considered mild if less than 1 cm, moderate if 1 to 2 cm, and severe if greater than 2 cm. In addition, magnetic resonance urography (MRU) was also obtained in patients depending on the availability.
Surgical technique
RAL-UU was performed on all patients by using the da Vinci surgical system (Intuitive Surgical, Inc.). Patients first underwent cystoscopic evaluation with placement of an open-ended ureteral catheter into the lower pole ureter on the affected side. This ureteral catheter was secured externally to the urethral catheter. A transperitoneal robotic approach was utilized as previously described for robotic extravesical reimplantation in the literature. 18 In brief, patients were placed at a 45° angle in the lateral decubitus position by using a Hassan technique. Port placement began with a peri-umbilical incision and placement of an 8.5 mm robotic camera trocar, followed by two separate 8 mm working ports placed under direct vision lateral to the ipsilateral rectus muscle at the levels of the anterior superior iliac spine and subcostal margin. The upper pole proximal ectopic ureter was dissected free, transected, and spatulated. This upper pole ureter was then anastamosed to the lower pole ureter as high as possible, just off the lower pole or directly into the lower pole pelvis when possible, in an end-to-side fashion. There is often a caliber mismatch between the ureters, and it is crucial to ensure an adequate opening in the normal lower pole ureter. A running, non-locking 5-0 or 6-0 braided suture was utilized on the posterior and anterior aspects to create a watertight anastomosis. Since it does not slip back, this has been technically easier to use than a monofilament. The distal portion of the upper pole ureter was then dissected down to the insertion point, and ureteral segments were removed all the way to the level of the vagina in girls and the prostate in boys. In our opinion, removal of the distal ectopic ureteral stump is an important step, as this can be a reservoir for infection even if it does not reflux. No drains were left in place. Before closure, 0.25% bupivicaine was injected at the port sites.
Outcomes
Intraoperative data were recorded, including operative time and estimated blood loss, as well as postoperative complications such as postoperative pain, hematuria, fever, urinary tract infection, and hospital readmissions. Postoperative analgesia and hospital length of stay (LOS) were also noted. All patients were discharged with instructions to use over-the-counter acetaminophen alternating with ibuprofen as required for pain. A follow-up evaluation was performed at 3 months after the operation, which included assessment of symptoms and a renal US. The surgery was considered successful if there was symptom resolution and/or improved HUN on US.
Results
Overall, 12 patients (4 male, 8 female) underwent RAL-UU during the 2-year study period. Demographic data and imaging results can be found in Table 1. Initial presentations included hydronephrosis in the majority of patients (10 of 12 patients, 83.3%), urinary incontinence (1 of 12 patients, 8.3%), and febrile urinary tract infection (1 of 12 patients, 8.3%). Mean patient age at the time of the procedure was 19.4 months (range 9–48 months), with a mean weight of 11.8 kg (range 9–14.2 kg) and a height of 79.4 cm (range 67.5–93 cm). On preoperative imaging, all patients had evidence of HUN on US and none had VUR of the duplicated system. However, one patient demonstrated contralateral grade 2 reflux on VCUG. Five patients (41.7%) underwent MRU, which demonstrated upper pole ureteral ectopia to the vagina in two children, urethra in one child, prostate in one child, and an indeterminate location in one child.
HUN = hydroureteronephrosis; LP = lower pole; MRU = magnetic resonance urography; UP = upper pole; US = ultrasound; VCUG = voiding cystourethrogram; VUR = vesicoureteral reflux.
The mean operative time, which includes cystoscopy, positioning, and robotic operative time, was 167 minutes (range 100–345 minutes) with a median of 138 minutes (IQR 119–180 minutes, Table 2). Of note, two patients had duplicated systems bilaterally, one of whom required bilateral repair for ureteral ectopia. Both of their procedures lasted significantly longer than unilateral procedures, with operative times of 293 and 345 minutes. There were no intraoperative complications or conversions to open surgery. The mean estimated blood loss was 1.5 mL (range 0–3 mL).
LOS = length of stay; POD = postoperative day; PRN = pro re nata (as needed); URI = upper respiratory tract infection.
The mean hospital LOS was 45 hours (range 17–129 hours) with a median of 31 hours (IQR 30–39 hours, Table 2). The two patients with bilateral pathology had extended hospital stays. One of these patients presented with a positive urine culture 2 days before her procedure and remained in the hospital 3 days after her operation for a 5-day course of antibiotic treatment. The other patient was pre-admitted 2 days before the procedure for preoperative antibiotic treatment due to pseudomonas colonization of bilateral nephrostomy tubes. If these two patients were excluded, the mean length of hospital stay for the other 10 patients was ∼1 day. There were no immediate postoperative complications. All ureteral and urethral catheters were removed on postoperative day 1. Most patients (10 of 12, 83.3%) were started on a regular diet on postoperative day 1. All patients received standing IV ketorolac and oral acetaminophen as needed for pain control postoperatively. Three patients were also prescribed oxycodone for breakthrough pain. No patient required narcotics after discharge.
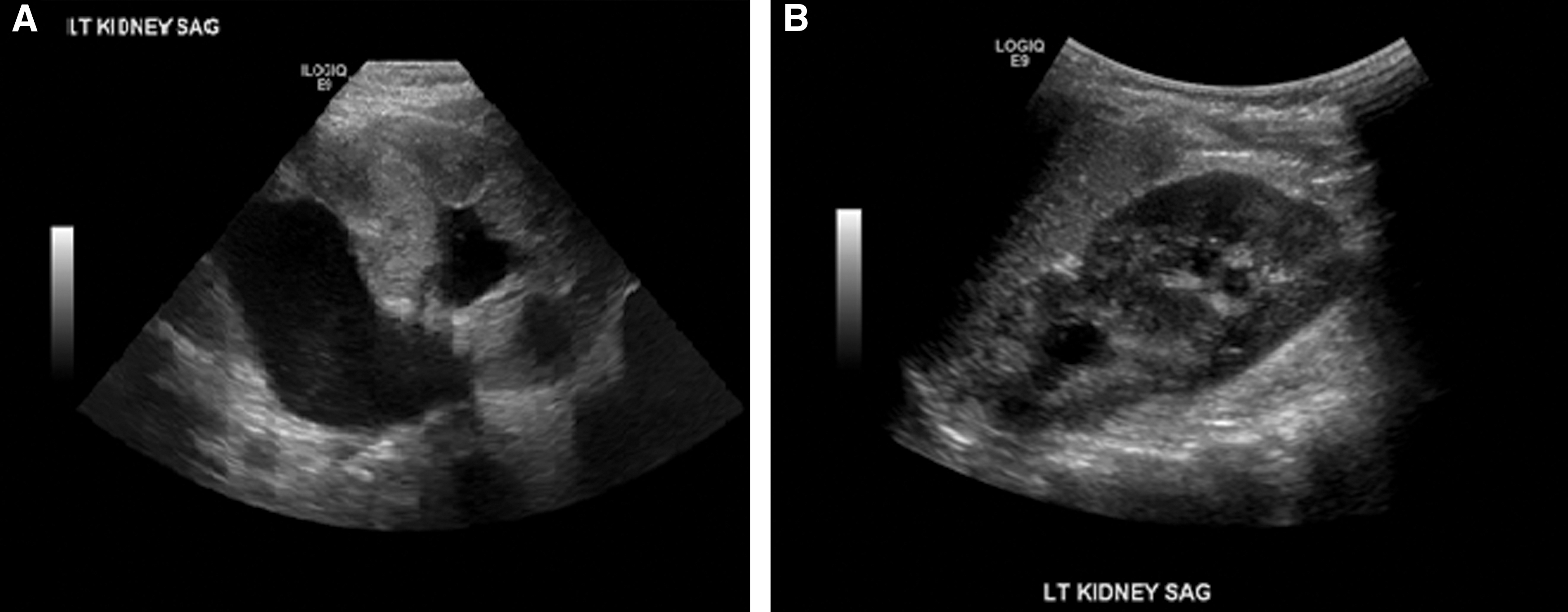
Median and mean follow-up times were 11 months (range 3–22 months). Before her postoperative urology follow-up appointment, one patient (8.3%) developed a febrile upper respiratory tract infection that was managed by her primary care provider. There were no other postoperative complications. On 3-month follow-up, renal US demonstrated improvement in HUN in all patients (12 of 12, 100%, Fig. 1). One 4-year-old girl with a history of persistent urinary incontinence became dry postoperatively (1 of 1, 100%). All three patients (100%) who attempted toilet training postoperatively were successful. In summary, all patients had improved HUN on US, resolution of preoperative symptoms, and were able to attain continence if toilet training was attempted. Only one patient experienced a postoperative complication, yielding an overall 8.3% complication rate and a 100% success rate.
Discussion
Minimally invasive surgical techniques are increasingly utilized in the pediatric population for complex reconstructive operations. In comparison to open surgery, laparoscopic surgery has been associated with decreased morbidity, less postoperative pain, lower analgesic requirements, quicker postoperative recovery, and shorter hospital stays. 19 –22 However, the technical difficulty associated with laparoscopic suturing and anastomoses has limited widespread application. This technical challenge is particularly significant in pediatric urology, where the surgical volume for complex urologic reconstruction is limited for most pediatric urologists. RAL surgery can overcome the limitations of traditional laparoscopic techniques and possibly increase the use of minimally invasive surgery for reconstructive pediatric urology. Here, we sought to demonstrate the safety and efficacy of performing RAL-UU in our pediatric patients utilizing an innovative approach.
Robotic surgery has demonstrated advantages to both open and laparoscopic surgery. The advantages of the da Vinci Surgical system include tremor filtration, motion scaling, and wrist-like instrumentation, providing 90° of articulation and 7° of freedom. 19,23 These features increase surgeon dexterity by almost 50% in comparison to conventional laparoscopic surgery, and they have been shown to decrease skills-based errors by 93%. 24 This is particularly important in complex procedures such as UUs that require precise suturing to establish a watertight anastomosis. In addition, identification of the affected ureter through the limited incision made in an open UU can be challenging. With robotic technology, there is improved exposure and visualization with a highly magnified three-dimensional image, which may convey a potentially decreased risk of complications while improving cosmesis with smaller port incisions. 25 Furthermore, in studies comparing RAL with open pediatric UUs, pyeloplasties, and extravesical reimplantations, patients in the robotic group benefited from decreased LOS, narcotic use, and operative times. 17,26,27
Despite the advantages of performing RAL surgery, its use in the pediatric population was initially limited due to concerns regarding operating the robot in smaller working spaces. Only three reports currently exist that analyze the use of RAL surgery exclusively in infants. 10,16,28 However, as it has increasingly been demonstrated to be feasible and safe, the role of robotic surgery in the pediatric population has expanded. Pyeloplasty for ureteropelvic junction obstruction remains the most commonly performed robotic procedure in pediatrics, but robotic technology is also being utilized for ureteral reimplantation, partial and total nephrectomy, as well as complex reconstructions, including bladder neck reconstruction, appendicovesicostomy, and bladder augmentation. 19,26,29 –31
Although RAL surgery is increasingly employed throughout pediatric urology, there are currently limited data evaluating RAL-UU and most of the existing literature is descriptive. To our knowledge, only nine studies from 2005 to 2014, encompassing a total of 45 patients with an average age of 58 months (range 4–192 months), critically appraise minimally invasive surgical techniques for pediatric UU (Table 3). Six of these studies assessed robotic surgery, whereas the other three evaluated conventional laparoscopic surgery. Indications for UU in these studies included ectopic ureters (84%), ureteral strictures (9%), VUR (4%), and ureterocele (2%). Seven studies reported operative times, of which five included the time spent performing cystoscopy in the operative time whereas the other two did not. The average operative time per patient was 144 minutes (range 45–338 minutes), and the average hospital LOS was 2 days (range 1–4 days). Outcomes were favorable with improved dilatation and resolution of incontinence in all patients. Complications included pyelonephritis in 7% of patients and urine leak in 2%. The largest study in this group included a total of 15 patients. A recent bi-institutional study by Lee et al. 17 comparing open surgery with RAL-UU included 25 children who underwent robotic surgery.
To the best of our knowledge, our current study with 12 patients represents the third largest study evaluating RAL-UU. 4 –6,10 –15 The results from our analysis are generally comparable to the other studies assessing the use of minimally invasive surgery for UU. Our patient population was younger than the patient populations in eight of the nine studies, with an average age of 19 months, including four infants. In analyzing the safety of performing RAL-UU in children, our estimated intraoperative blood loss was negligible and there were no intraoperative complications or conversions to open surgery. Postoperative pain was minimal and well controlled with standing IV ketorolac and oral acetaminophen as needed. Thus, our series confirms the results of previous reports that RAL-UU is feasible and safe, while offering minimal postoperative analgesic requirements, in children and infants.
Notably, the other existing published series on performing minimally invasive UU in the pediatric population describe utilizing indwelling ureteral stents, typically for 4 to 6 weeks or at a minimum of 1 to 2 weeks. Ureteral stents are often left in place for a longer duration to reduce the risk of an anastomotic leak during the initial recovery period. Unlike these other reports, in our series, a temporary open-ended ureteral catheter was placed at the start of the procedure and then removed along with the urethral catheter on postoperative day 1. The senior author found that stents on a string were frequently pulled accidentally when foley catheters were removed postoperatively. So his practice transitioned to utilize open-ended ureteral catheters, which are intended to be removed postoperatively along with the foley catheter. We believe that it is unnecessary to stent across the anastomosis for a longer duration, since the urine passage from the upper pole moiety is sufficient to maintain ureteral patency, and the ureteral catheter is only necessary to temporarily divert urine from a potentially leaking site in the immediate postoperative period. Importantly, no patient in our study developed a urine leak in the postoperative period after ureteral catheter removal, which suggests that leaving a ureteral stent for a longer duration may be unnecessary with a well-executed anastomosis. This practice obviates the need for children to undergo a second procedure to remove the stent, if there is no extraction string. For instance, almost 25% of cases in Lee's series required a second procedure for stent removal. 17 Furthermore, this technique mitigates stent-related morbidity, including stent migration, flank pain, and bladder spasms, and it avoids the use of antibiotic prophylaxis, which surgeons may prescribe postoperatively while a ureteral stent is in place. Altogether, in the pediatric population, this can simplify postoperative care for families.
In the study of Lee et al., 17 a ureteral stent was utilized in all robotic cases, whereas less than half of the children who underwent open repair had a stent placed. They did find a higher rate of improved or resolved HUN in robotic cases compared with open surgery cases, which may be explained by the use of ureteral stents in robotic cases. However, here, we demonstrate that RAL-UU with the use of a temporary ureteral catheter is an effective treatment for the management of duplex systems with ectopic ureters. We evaluated procedure success based on the improvement of HUN on postoperative US and resolution of symptoms. At a 3-month follow-up, all patients who were evaluated had improved HUN. The only symptomatic patient preoperatively with persistent urinary incontinence became dry after surgery, and all three children who attempted toilet training were successful. Therefore, RAL-UU was 100% successful in our pediatric series.
There are several limitations to this study, which include the retrospective design, small patient sample size, lack of a comparison group, single institution, and only two surgeons performing all procedures. In addition, we do not address concerns over use of robotic technology such as cost analysis. However, our study achieves its main purpose of demonstrating that RAL-UU utilizing a temporary ureteral catheter is feasible, safe, and effective in pediatric patients with ectopic ureters, and that it should be considered in the armament of minimally invasive surgical techniques in the management of these children. Further investigation is warranted to study the role of ureteral catheters and stents in the reconstruction of ureteral duplication anomalies.
Conclusions
We demonstrate that RAL-UU is a feasible, safe, and effective approach to manage duplicated, ectopic ureters in the pediatric population. Given the technical difficulties associated with conventional laparoscopic suturing, RAL surgery may reduce the learning curve and increase the prevalence of performing minimally invasive surgery for UU on infants and children with ectopic ureters. Increased visualization, in situ repair, and improved reconstructive maneuvers provide excellent surgical outcomes. Use of a temporary ureteral catheter, minimal postoperative pain, and early hospital discharge facilitate the recovery for the child and their family.
Footnotes
Author Disclosure Statement
No competing financial interests exist.