
Abstract
Aim:
The management of malignant ureteral obstruction (MUO) is a challenging but common problem for urologists. The different techniques currently used to address this complicated issue include percutaneous nephrostomy, extra-anatomical stents, retrograde (single) stent insertion, and metallic stents. In those situations where single ureteral stent insertion has failed, retrograde tandem or twin ureteral stent (TUS) insertion can be completed. The aim of this study was to report our clinical experience and also assess the efficacy of TUS insertion within our tertiary referral center.
Methods:
Data were prospectively collected from patients requiring TUSs over an 8-year period between January 1, 2006, and December 31, 2014. A number of variables, including the improvement in renal function following TUS insertion, were recorded.
Results:
Twenty-two TUS insertion procedures were performed on 15 patients between the period of January 1, 2006, and December 31, 2014. The mean patient age was 68.0 years (39–85 years). There were 15 primary insertions as well as 7 subsequent stent changes. The average prenephrostomy creatinine was 428 μmol/L; an average improvement of 196 μmol/L was observed after percutaneous drainage. Serum creatinine after TUS remained stable on discharge, 214 μmol/L vs 227 μmol/L preoperatively, p = 0.34. Eleven patients died at a median 131 days post-TUS insertion. TUS failure occurred in three patients; this was characterized by rising creatinine and worsening hydronephrosis. Patients with failing TUS had a median life expectancy of 45.6 days compared with 162.5 days for those with functioning TUS (p < 0.05). Overall, the patency rate at 3 months was 80%.
Conclusion:
TUS insertion is a technically efficient and effective procedure in the management of MUO, with the majority of patients treated dying of the underlying condition with functioning stents in situ.
Introduction
T
A number of solutions have been proposed to the problem of MUO refractory of single ureteral stent insertion. The choice of treatment ranges from indwelling Double-J stents, nephrostomy tube drainage, metallic stents, extra-anatomic stenting, open, laparoscopic, or robotic corrections, urinary diversions, or nephrectomy. 5,6 Failure necessitates the placement of a percutaneous nephrostomy, which has associated complications and impact on quality of life.
The use of twin ureteral stents (TUSs) is considered an alternative to a single Double-J stent by urologists for several years. It has been thought that placement of two stents provides additional drainage both due to the extra lumen of the second stent and the creation of a space between the two stents and the ureteral wall. A 2006 study by Hafron and colleagues 7 showed that the usage of a dual-lumen ureteral stent in a porcine ex vivo kidney model increase the flow as much as five times more than the use of a single stent. Despite this pervasive concept, there are still limited published data and evidence to support their use.
We report our experience with the use of TUSs in the management of MUO.
Methods
Our prospectively maintained stent register was interrogated to identify all twin stent insertions for malignant disease between February 2006 and June 2014. All procedures were performed or supervised by a single consultant endourologist. All TUS insertions followed the same technique as detailed below.
Exclusion criteria included patients who had a previous ureteral balloon dilation, retrograde/antegrade endopyelotomy. Technical success, postoperative renal function, and patients' survival were the measured outcomes. Twin stent failure was defined with increasing hydronephrosis and associated deterioration of renal function.
Technique
Under general anesthesia, rigid cystoscopy was completed. This was followed by retrograde insertion of a superstiff guidewire under fluoroscopic guidance to the renal pelvis and progressive coaxial ureteral dilatation of the ureteral stricture to 16F over the guidewire. A dual-lumen ureteral catheter was then inserted not only to complete a retrograde study but also to facilitate the insertion of a second superstiff guidewire. After removal of the dual catheter, the two ureteral guidewires were closely aligned; two 8F ureteral stents were subsequently advanced over the guidewires to the renal collecting system. The guidewires were then removed to allow for the coiling of the stents in the renal pelvis under fluoroscopic imaging. Nephrostomies, when present, were removed after an antegrade nephrostogram confirmed drainage (Figure 1).
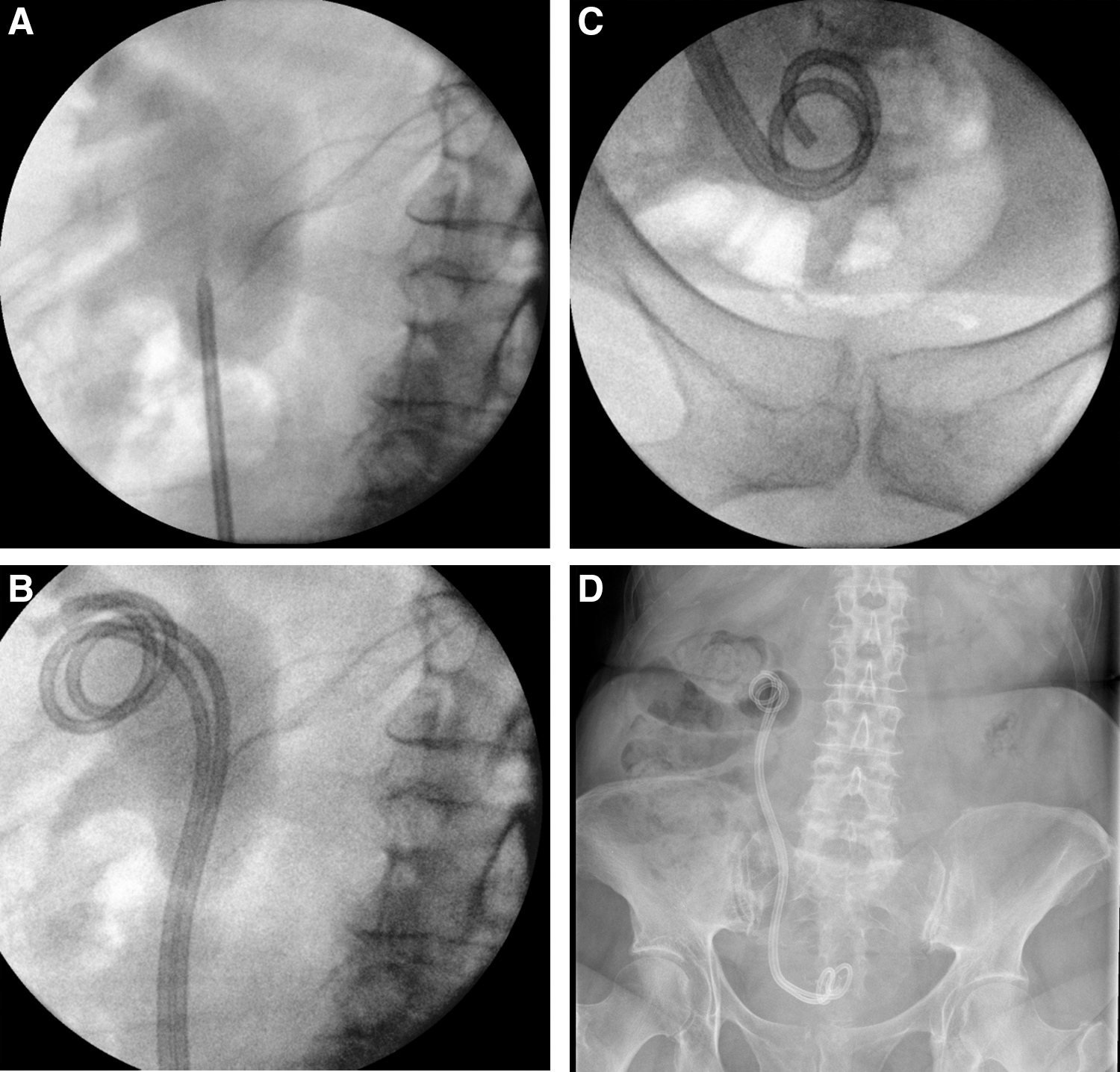
Positioning of twin ureteral stent (TUS).
Results
Overall, 22 TUS insertion procedures were performed on 15 patients. The mean patient age was 68.0 years (39–85 years). There were 15 primary insertions as well as 7 subsequent stent changes. Eighteen of these procedures were performed bilaterally. There was one procedure-related complication recorded, a urinary tract infection 2 days postoperatively.
Indications for TUS insertion included colorectal adenocarcinoma (40.9%), prostate (31.8%), and ovaries (18.2%) (Table 1). All the patients had a single ureteral Double-J stent, which failed at the time of presentation. The selection of patients was guided by the treating oncology teams. This was governed by both the expected survival time and the suitability for further treatment primarily in the form of chemotherapy. Thirteen patients had a cutaneous nephrostomy in place before TUS insertion; the average duration of the percutaneous drainage was 21 days. All the patients had removal of the nephrostomy after TUS insertion.
TUS = twin ureteral stent.
The procedure was deemed technically efficient in all patients, with all patients having TUSs placed at the end of the procedure. The average prenephrostomy creatinine was 428 μmol/L; an average improvement of 196 μmol/L was observed after percutaneous drainage. Serum creatinine after TUS remained stable on discharge, 214 μmol/L vs 227 μmol/L preoperatively, p = 0.34 (Table 2).
Eleven patients died at a median 131 days post-TUS insertion. The median survival time of patients with prostate cancer was 140.8 days, 213.3 days with ovarian cancer, 378.8 days with colorectal cancer, and 80.3 days with transitional cell cancer. TUS failure occurred in three patients, this was characterized by rising creatinine and worsening hydronephrosis. Two of the failures were observed in patients with prostate cancer and one with ovarian cancer. All the failures were observed within the first 3 months; therefore, the overall patency rate at the 3-month interval was 80%. There were no failures thereafter. Patients with failing TUS had a median life expectancy of 45.6 days compared with 162.5 days for those with functioning TUS (p < 0.05).
Five of the 15 patients had stents exchanged during the duration of the study, 2 of those had a further exchange. One patient had an extra-anatomical stent inserted after 9 months of TUS insertion. The median stent life was 156 days (95% CI 131, 181.07) (Table 2).
Discussion
MUO remains a difficult clinical problem in a group of patients with a high mortality rate. Our study provides further evidence that TUSs can be effective in the management of MUO in patients with failing single Double-J ureteral stents. The failure rate in our study was 20% at 3 months. This is similar to the reported TUS failure rate of 12.8% recorded in a larger study by Elsamra et al., 8 which is the largest study to date. Median survival after stent failure in the patients included in this study was 66 days. In our study, the median survival time in this group was 45.6 days. From this, it is apparent that early stent failure is a poor prognostic sign, associated with short survival periods even after percutaneous drainage of the obstructed system.
Four older retrospective studies with smaller cohords reported variable failure rates. Chen and colleagues 9 with a cohort size of 39 patients had a failure rate of 73% at 3 months, but it has to be noted that a large number of the cases had the tandem stent placed alongside an already failed single stent. The other three studies reported one TUS failure in a total of 16 patients. 10 –12
The aforementioned low failure rates in our experience with TUS are comparable with the results observed with the use of metal mesh ureteral stents, especially the Memokath 051 stent, which has the best available results to date and has been in use since 1996. 13,14 Both of these studies included patients with both MUO and benign strictures. Their results showed that the primary failure rate ranged between 7% and 8%. However, if you add the cases that required early stent manipulation due to migration and encrustation, the failure rates rise to 23% and 29%, respectively. Despite the emergenging evidence to support the use of metallic ureteral stents due to the better symptom profile, 15 the prior studies have not commented on the number of hyperplastic reactions recorded. Furthermore, other confounding reasons limiting their use are the lack of availability, cost and complexity of insertion, and complexity of subsequent changes.
Conclusion
Our study suggests that TUS is a technically efficient and effective procedure in the management of MUO, with the majority of patients treated dying of the underlying condition with functioning stents in situ. TUS allows discharge from the hospital without percutaneous nephrostomies and thus allows a better quality of life for these patients. Despite these good results, there is still lack of larger, randomized prospective trials to establish their use in daily practice.
Footnotes
Author Disclosure Statement
No competing financial interests exist.