
Abstract
Purpose:
There is little literature on robotic retroperitoneal lymph node dissection (RRPLND) in the difficult post-chemotherapy (PC) setting. We report on the outcome of RRPLND in patients with PC-residual masses.
Materials and Methods:
Between 2011 and 2015, we performed 12 PC-RRPLND. Mean patient age was 37.8 years. Mean body mass index was 30.78. Nine (75%) patients had nonseminomatus germ cell tumor (NSGCT) and three (25%) patients had seminoma tumors. Cancer stage was III in six (50%), II-C in three (25%), II-B in two (16.7%), and II-A in one (8.03%). International Germ Cell Cancer Collaborative Group (IGCCCG) prognostic classification in the NSGCT was good in six, intermediate in two, and poor in one, and was good in the three seminoma patients.
Results:
The procedure was completed effectively in 11 (91.7%) patients. Mean operative time was 312 minutes. The mean estimated blood loss was 475 mL. Mean hospital stay was 3.2 days. Mean number of lymph node excised was 12. Six of the excised masses were ≥5 cm (N3), largest was 7.5 cm. Pathology showed teratoma in five (45.5%), benign/necrosis in five (45.5%), and viable germ cells in one (9%). Major complication (Clavien ≥3) occurred in one patient and minor (Clavien ≤2) in two. Antegrade ejaculation was preserved in eight patients and in one could not be assessed. At a median follow-up of 31 months, no infield or outfield relapses occurred.
Conclusions:
Robotic PC-retroperitoneal lymph node dissection (RPLND) is technically feasible and with acceptable morbidity. It is associated with low blood loss and short hospital stay. More research is needed to assess the long-term outcome and to compare standard open RPLND.
Introduction
T
Lymphatic spread in testicular cancer is to the retroperitoneal lymph nodes (LNs), close to the embryologic origin of the testes near the great vessels. The primary landing zone for right testicular cancer is the interaortocaval LNs followed by the precaval and paracaval LNs. For left-sided testicular cancer, it is the para-aortic and preaortic LNs. Retroperitoneal lymph node dissection (RPLND) provides control to the retroperitoneal LNs, which is usually the first and often the only site of metastatic disease. 3
RPLND is indicated after radical orchiectomy in the chemotherapy naive patient and in the post-chemotherapy (PC) setting. RPLND is indicated after chemotherapy in the management of radiologic incomplete remission, consolidate chemotherapy to remove occult disease and in the presence of teratomatous elements in the initial orchiectomy specimen. 4
Open PC-RPLND is the gold standard. 5 However, the procedure is associated with 29.3% risk of intraoperative procedures and complications. 6 Also, research showed that there is reduced exposure to that particular surgery in urology residency programs. 7
Laparoscopic RPLND emerged as an attractive alternative. 8 Laparoscopic PC-RPLND is reported to have a favorable oncologic outcome compared with open surgery. 4 However, there were concerns regarding the difficulty of laparoscopic dissection in the retroaortic and retrocaval spaces as well as a steep learning curve. 9
Since its first report in 2006, robotic retroperitoneal lymph node dissection (RRPLND) is gaining wider acceptance in the treatment of testicular cancer. 10 RRPLND has the advantages of open surgery with the 360° wrist movement, three-dimensional vision, ease of management of intraoperative complications, in particular, vascular complications. In addition, it has the advantages of laparoscopic surgery, being minimally invasive, less blood loss, magnification up to 8×, shorter hospital stay, and shorter recovery. Reports describing the outcome of PC-RRPLND are sparse. The outcome is usually reported combined with the naive and PC-RRPLND. 11 –18
We herein report our academic institution experience in performing PC-RRPLND on 12 testicular cancer patients with emphasis on the surgical technique, intraoperative and postoperative considerations, and morbidity of the surgery.
Materials and Methods
Patient population
Between 2011 and 2015, 12 patients with PC residual retroperitoneal LN disease underwent PC-RRPLND. All the robotic surgeries were performed either using the da Vinci® S or Si robots (Intuitive Surgical, Sunnyvale, CA). The mean patient age was 37.8 years (range 20–55). Eleven patients were Caucasians and one African American. Mean body mass index was 30.78 (range 23.7–41.1). Mean Charleston Comorbidity Index was six (range 2–10). Eight (66.67%) were right testicular cancers and four (33.33%) left. Nine (75%) patients presented with nonseminomatus germ cell tumor (NSGCT) and three (25%) with seminomatus germ cell tumor. Ten patients had radical orchiectomy, one patient had radical orchiectomy with excision of enlarged inguinal lymphnodes, and one patient had an orchiectomy for a right undescended testis at the time of PC-RRPLND.
In 10 patients, the diagnosis for testicular cancer was achieved after radical orchiectomy. The remaining two patients were each found to have a retroperitoneal mass on CT scan. After a biopsy of the mass, they were diagnosed with a germ cell tumor. Three (25%) patients presented with nonfunctioning kidney at the time of their initial presentation, secondary to obstruction from the retroperitoneal mass.
Following the radical orchiectomy and before the chemotherapy, the cancer stage was III in six (50%) patients, II-C in three (25%), II-B in two (16.7%), and II-A in one (8.03%). Stage III patients (n = 6) had retroperitoneal lymphadenopathy in addition to pulmonary metastasis in four (66.6%), pulmonary metastasis in addition to large mass invading the psoas muscle in one (16.7%), and lumbar vertebrae metastasis in one (8.3%). One patient with stage III disease had a residual solitary lung mass for which he underwent thoracotomy and right middle lobe lobectomy before the PC-RRPLND. Pathology of the lung mass showed only a mass of necrotic tissue with no viable cancer cells or teratoma elements.
The International Germ Cell Cancer Collaborative Group (IGCCCG) prognostic classification of the NSGCT patients (n = 9) was good in six, intermediate in two, and poor in one. All seminoma patients (n = 3) had good prognostic classification. One of the three seminoma patients had inguinal LN dissection at the time of radical orchiectomy as the inguinal LNs were fungating and eroding through the groin skin. Seven patients received their adjuvant chemotherapy outside our academic institution and five by our medical oncology department. Of the NSGCT group (nine patients), five (55.6%) had a residual mass of ≥5 cm after the chemotherapy and before the PC-RRPLND. In the seminoma group (three patients), one (33.3%) had a preoperative LN mass of ≥5 cm. A summary of the preoperative chemotherapy administered and radiologic findings is illustrated in Table 1.
After chemotherapy and pre-PC-RRPLND; bPost-radical orchiectomy and before chemotheraphy; cFNA of retroperitoneal mass; dType of NSGCT was not provided.
BEP = bleomycin, cisplatin, etoposide; Bil = bilateral; EBL = estimated blood loss; FNA = fine needle aspirate; IGCCCG = International Germ Cell Cancer Collaborative Group; IT+PCE = ipsilateral template+post-chemotherapy mass excision; IVC = inferior vena cava; LN = lymph node; LOS = length of stay; N/A = not assessed; NSGCT = nonseminomatus germ cell tumor; OT = operative time; PC-RRPLND = post-chemotherapy robotic retroperitoneal lymph node dissection; RE = retrograde ejaculation; Rec = recurrence; Tx = transfusion; FNA = fine needle aspirate.
Indications of PC-RRPLND in the NSGCT patients (n = 9) were normal tumor markers and residual PC mass ≥1 cm in eight patients and to consolidate chemotherapy in a patient with adverse prognostic features in the initial orchiectomy specimen in one (100% embryonal carcinoma with positive lymphovascular invasion). In the seminoma patients (n = 3), a residual retroperitoneal mass ≥3 cm was the indication for the PC-RRPLND in two patients and one had a positive PET/CT scan with a residual mass <3 cm. All patients were advised to have sperm banking before the PC-RRPLND surgery.
Operative technique
In the first six PC-RRPLND performed, the flank approach was utilized with robot docking over the patient's side. As of the seventh PC-RRPLND, the technique changed to the lithotomy position with a steep Trendelenburg position and the robot docking over the patient's head. The main advantages and disadvantages of both approaches are summarized in Table 2.
Table 1: patients 7 to 12; bTable 1: patients 1 to 6.
Flank approach
The technique of PC-RRPLND in the flank position was described before. 12 Port placement is illustrated in Figure 1. For the first few patients, four robotic arms approach was used and with increasing skills the procedure was able to be performed with three arms only. In summary, the procedure was started by mobilizing the colon by taking down the line of Toldt. The dissection continued in a cephalic direction to mobilize the hepatic flexure on the right or the splenic flexure on the left. Dissection proceeded in a caudal direction until the peritoneal reflection over the iliac vessels. The ureter was identified and all the lymphatic tissue between the ureter and the inferior vena cava (IVC) on the right side and aorta on the left side was removed. The gonadal vein was identified at the level of the internal ring and traced to the IVC on the right side or the renal vein on the left side and divided in between silk sutures or Hem-o-Lok® (Teleflex, Morrisville, NC) clips (Fig. 2).
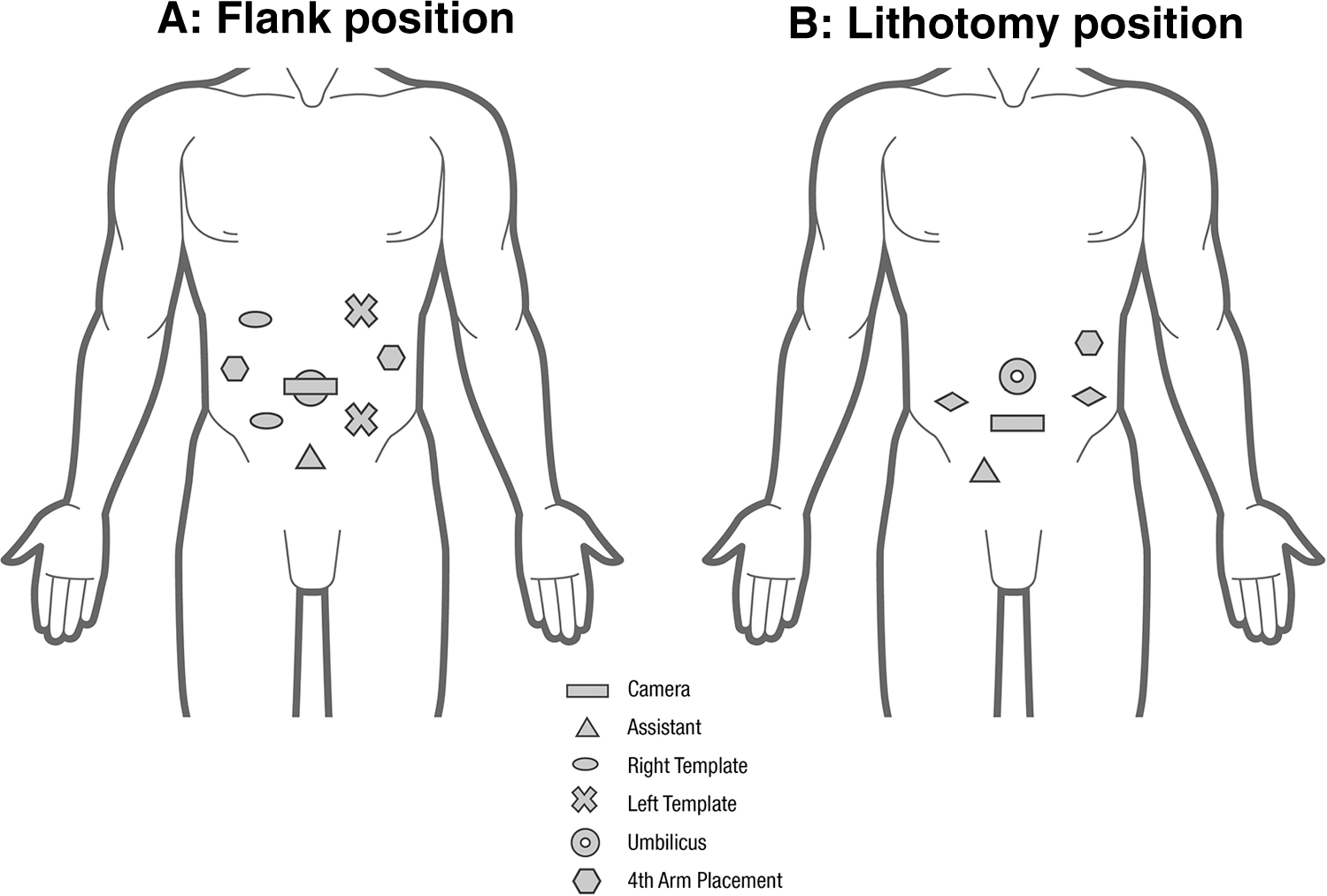
Ports placement.
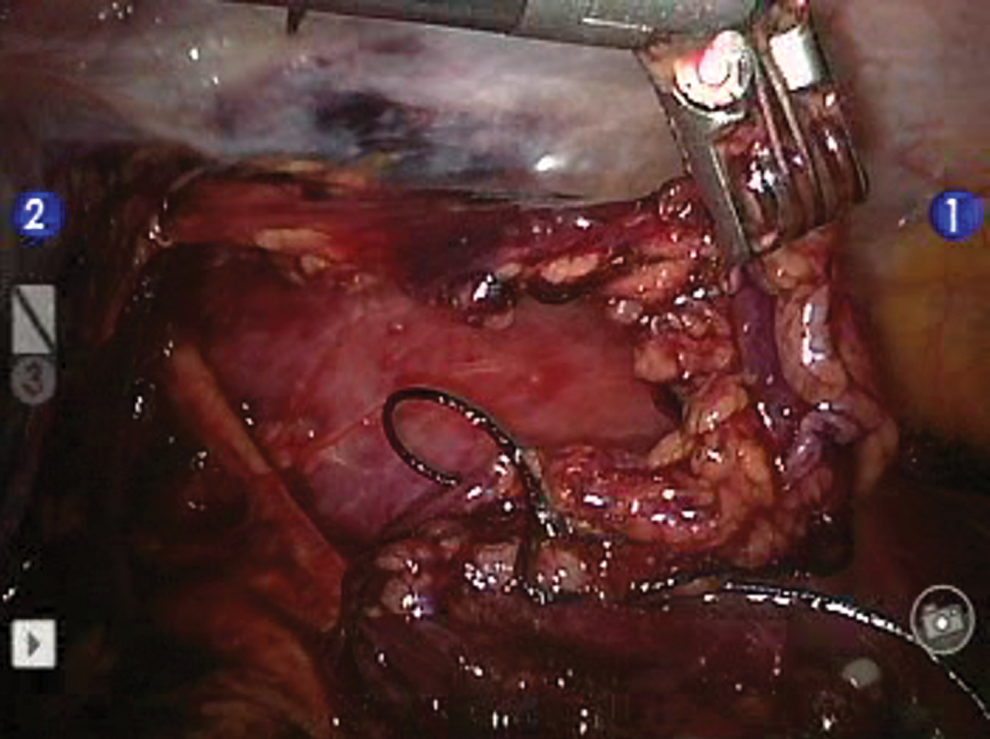
Spermatic cord excision at the level of internal ring.
To access the precaval and interaortocaval lymphatic tissue from the right side, the second part of duodenum was kocherized using gentle sharp and blunt dissection. Due to the right lie of mesenteric root, access to the interaortocaval area from the left is more challenging. The fourth part of duodenum was mobilized to access to the interaortocaval area and the right retroperitoneum from the left side. The lumbar vessels were controlled using Hem-o-lok or 3-0 silk sutures.
The postganglion sympathetic nerves were prospectively identified and preserved. All the lymphatic tissue in the interaortocaval area was removed exposing the anterior spinous ligament with the upper boundary of dissection being the inferior border of the renal vein. In excising the PC mass, the dissection started at the lower pole of the mass and working posteriorly elevating the mass off the underlying tissue. Following that, the lateral and medial attachments were exposed, clipped, and divided (Fig. 3).
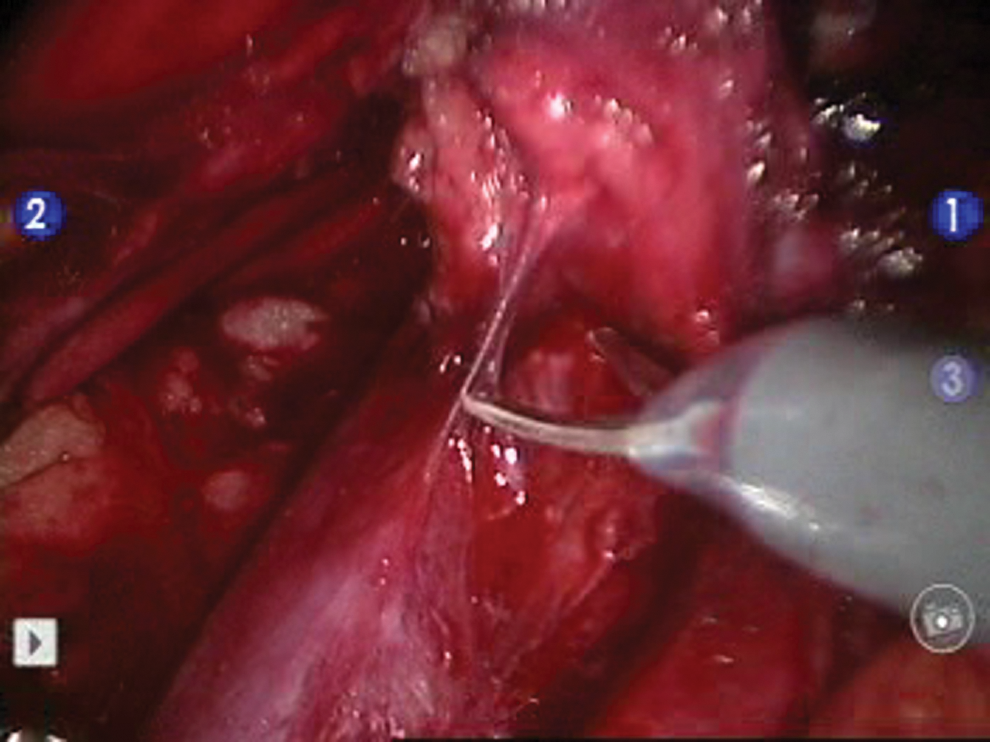
Mass dissection off the inferior vena cava.
Lithotomy approach
The patient was placed in the steep Trendelenburg position with the robot docked over the patient head. Port placement is illustrated in Figure 1. The procedure was started by dividing the peritoneal reflection on the common iliac artery bifurcation on either side. The peritoneal window dissection continued in a cephalic direction to the ligament of Treitz. Dissection of the ascending colon or cecum was not performed at that point of the procedure to keep the colon in place with its lateral attachment and minimize falling of the large bowel medially. Hammock-like sutures were used to retract the cut peritoneal edge on either side toward the anterior abdominal wall. The third part of duodenum was mobilized upward to expose the renal vein on either side forming the upper boundary of dissection. The duodenum was retracted by applying traction on the underlying peritoneal edge using the fourth robotic arm.
Following these steps, a rectangular field of dissection extending from the renal veins superiorly to the common iliac vessels inferiorly and ureters exposed on either side was developed, (Fig. 4) similar to the exposure achieved in standard open RPLND (Fig. 3). Dissection proceeded using the Split and Roll technique described by Donohue. 19 In the lithotomy approach, the cord was excised at the internal ring either by docking the robot in between the patient's legs or laparoscopic at the end of the procedure. In a seminoma patient with several residual PC masses along the aorta/IVC/common iliac and external iliac vessels, the procedure was performed by docking over the patient's head to remove the PC masses in the interaortocaval area and docking in between the patient's legs; similar to robotic prostatectomy to remove the external iliac and common iliac PC masses (Fig. 5).
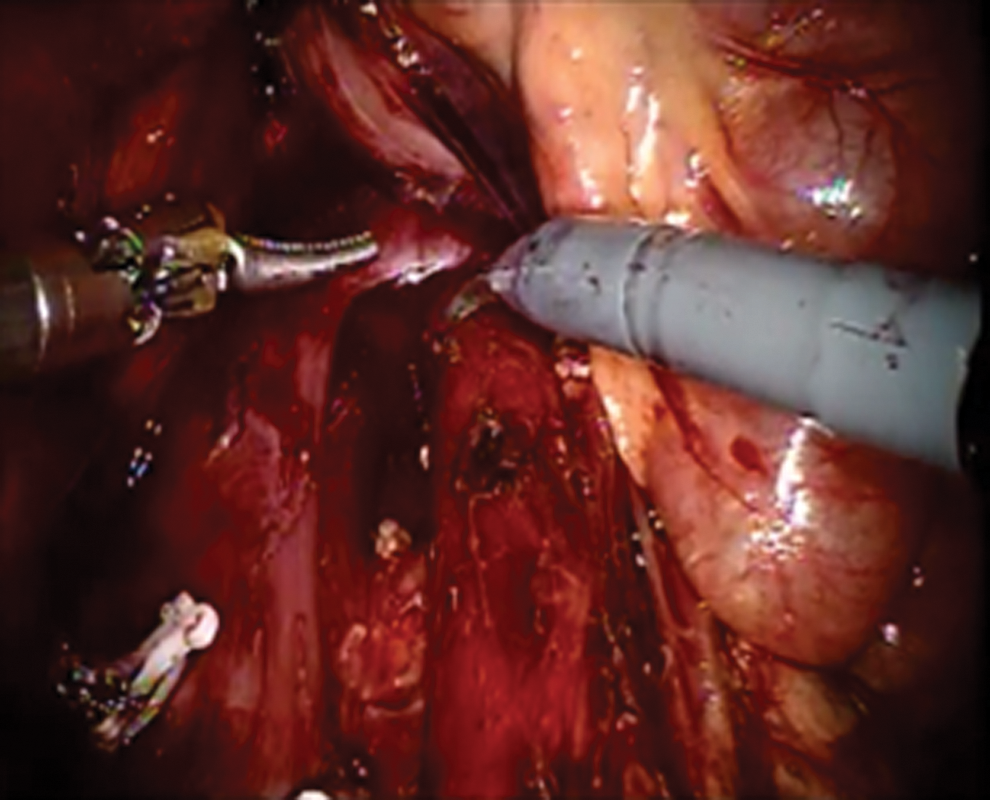
Rectangular field of dissection.
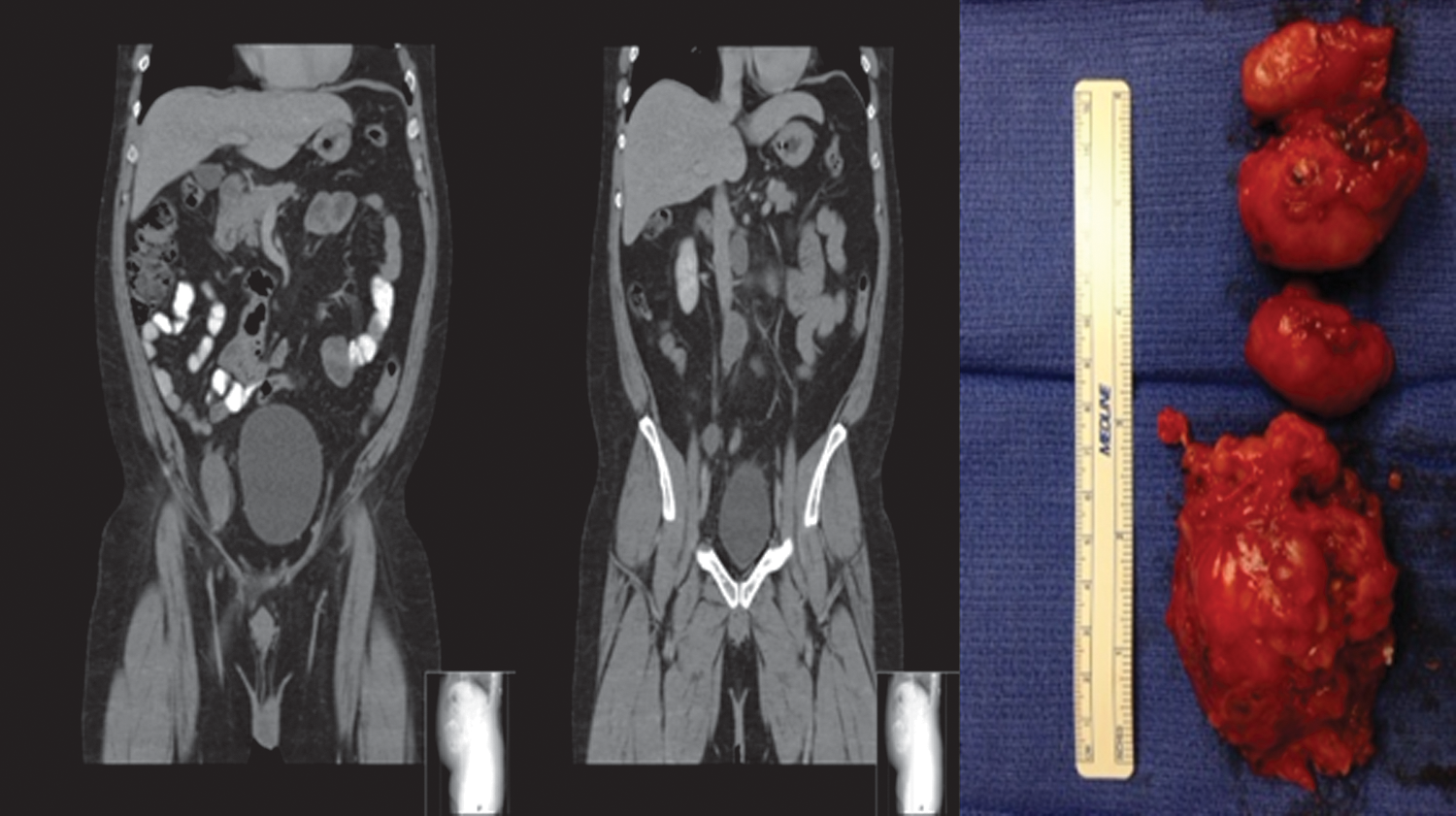
Multiple post-chemotherapy masses in a seminoma patient following effective excision.
Pathologic examination
The fibroadipose tissue received from surgery was palpated and sectioned to identify grossly visible LNs. In some cases, extensive involvement of LNs by tumor and/or necrosis resulting in fibrosis and matting of multiple LNs into one large mass where the individual LNs were no longer able to be identified and separated by the pathologist performing the gross examination. In such cases, the mass of LNs was called “multiple matted lymph nodes” and representative sections of the large mass of matted LNs were submitted for histologic examination.
Results
The procedure was effectively completed using the robot in 11 (91.7%) patients. In these 11 patients, the mean operative time (OT) was 312 minutes (range 205–408) and the mean blood loss was 475 mL (range 50–1800). Excluding the three seminoma patients, the mean blood loss was 202 mL (range 100–600 mL). Blood transfusion was needed in two (18.2%) patients and both were originally diagnosed with pure seminoma in the original orchiectomy specimen. The mean length of stay was 3.2 days (range 2–5).
Of the 11 patients, complete follow-up was available in 10 patients. One patient was lost to follow-up after the first clinic visit following his RRPLND. He did not present with any postoperative complication during that only clinic visit he had with us. For the remaining 10 patients, the median follow-up was 31 months (range 5–39). No patient developed a recurrence either infield or outfield. Of the 10 patients, 8 patients had antegrade ejaculation, 1 patient had retrograde ejaculation, and 1 patient's postoperative ejaculatory status could not be assessed due to erectile dysfunction.
Regarding LN count, in two patients, one in the NSGCT group and one in the seminoma group, pathologic examination to identify the number of excised LNs was not possible as the entire specimen was composed of necrotic tissue with complete loss of LN architecture. In addition, six masses of matted LNs ranging in size up to 3 inches (7.5 cm) were excised and counted as one LN mass by our pathologist, all in five NSGCT patients. The mean LN count in the NSGCT group was 12 (range 5–21).
In the 11 patients, postoperative pathologic examination of the excised LNs revealed teratoma in 5 (45.5%), necrotic tissue/benign LNs in 5 (45.5%), and rare viable germ cells in 1 (9%). The patient who had viable germ cell tumor in the excised LNs received additional two cycles of EP.
In one patient (patient 12, Table 1), conversion occurred following injury to the inferior mesenteric artery that was completely encased by tumor. The procedure was completed by open surgery, and pathology in the PC-residual mass showed only necrotic tissue with no teratoma or viable germ cells.
Complications
There were two (18.2%) minor complications (Clavien ≤ II); postoperative ileus and neuropathy affecting one upper limb. The patient who had the upper limb neuropathy had cisplatin-related neuropathy affecting his lower limb before the surgery. He developed an upper limb neuropathy following the PC-RRPLND, which we believe may be related to the prolonged lithotomy position. There was one (9.1%) major complication (Clavien ≥ III). This was in a seminoma patient with an aortic injury that was repaired intraoperative with polypropylene suture and with adequate hemostasis. He presented 6 weeks later with left loin pain. A CT scan showed an aortic pseudoaneurysm that was effectively repaired with percutaneous endovascular endograft by the vascular surgery team. Details of our results are illustrated in Table 1.
Discussion
We report on our academic institution experience in performing PC-RRPLND on 12 patients, including 3 patients who underwent RPLND for residual PC seminoma tumors. To our knowledge, this is the largest report describing the outcome of RRPLND only in the PC setting. Six (54.5%) of the 11 patients, in whom the procedure was completed robotically, had preoperative LN masses greater than 5 cm (N3), thus underscoring the challenging group of patients in this series. There are few reports that describe the outcome of RRPLND in the primary and post-chemotherapy patients. We summarized the main findings of these reports in Table 3.
Including matted LN masses; bOverall results (both primary and post-chemotherapy); cStage unavailable for the four post-chemotherapy cases; dPrimary/post-chemotherapy; eOne RE out of 11 had nerve sparing RRPLND.
↑K+ = intraoperative hyperkalemia.
PC-RPLND is a particularly difficult procedure with a high complication rate. Chemotherapy is associated with desmoplastic reaction causing the dissection to be difficult. Bleomycin can cause pulmonary fibrosis complicating intra- and postoperative fluid management with the risk of pulmonary edema. Additional intraoperative procedures such as nephrectomy, IVC resections, and arterial grafts were needed in 22% of patients in one large series. 20
The surgical boundaries of RPLND for PC residual retroperitoneal masses have been the subject of extensive debate and have undergone modifications in contemporary literature. Classically, the dissection field boundaries are the renal vessels superiorly, the ureters laterally, and common iliac vessels inferiorly. 21 In an attempt to reduce the morbidity of the surgery, reducing fluid requirements, maintenance of emission and ejaculation, and shorter OTs, some authors advocate a further limitation in the template in select patients.
In one study from Indiana University, 100 patients with PC residual masses limited to the primary landing zone underwent either modified or full template dissection. The 5-year disease survival rate was 95%. In that study, four patients developed all outfield recurrences. 22 In another large European study, 98 patients who had ipsilateral template dissection with residual mass excision were compared with 54 patients who had bilateral RPLND. Heidenreich and colleagues found only one infield relapse in the limited dissection group compared with seven outfield relapses in the bilateral group. The authors concluded that if the LN mass is corresponding to the landing zone of the primary tumor, limited dissection is justified. The recommendation is particularly valid for left-sided primary tumors as cross-lymphatic metastasis in the retroperitoneum occurs rarely. 23
The largest study to date describing outcomes of RRPLND is reported from the Mayo Clinic by Cheney and colleagues on 18 patients, of whom 8 underwent PC-RRPLND for stage I-IIB nonseminoma germ cell tumors. In this group, there was no difference between the patients who underwent RRPLND with or without prior chemotherapy when comparing LN yield, blood loss, or hospital stay. However, in this study, the OT was significantly shorter for primary vs post-chemotherapy RRPLLND. 15 Our study adds to the previously published reports and showed that PC-RRPLND is feasible in stage II-C and PC-seminoma tumors.
Over the years, the technique and approach of RRPLND were refined to provide a procedure similar to open RPLND. We changed from the flank position to the lithotomy position to enable performing the procedure in a similar manner to open surgery. The challenge in the lithotomy position is the spermatic cord dissection using the da Vinci S or Si models. Recently, Porter reported that he was able to dissect the spermatic cord without the need to redock the robot using the da Vinci Xi model with the patient in the lithotomy position. In this study, the robot was docked from the patient's side, thus allowing more room for the anesthesia team to manage the patient's airway. He attributed this success to the Xi surgical platform, which allows better multiquadrant surgery than older models. 24 Another important step in achieving excellent surgical field are the hammock sutures passed between the peritoneal edge and the inner side of the anterior abdominal wall or through the skin described by previous authors. 14–15
There were lessons learnt from performing these procedures. In the flank approach, ligation of the inferior mesenteric artery may be required to access the interaortocaval area and the precaval area from the left side. Also, when docking the robot over the patient head while in the lithotomy position, coordination with the anesthesia team is important to confirm they have good access to airway and central line. The surgeon should be cautious of the following structures to avoid their injury during the procedure; the origin of the inferior mesenteric artery just above the aortic bifurcation, the right gonadal artery in the interaortocaval area, and the origin of the left gonadal artery on the side of the aorta. Also by careful, thorough, and repeated inspection of the preoperative CT scan, the lumbar and accessory renal vessels can be counted and their position anticipated during the surgery.
In these PC-RRPLND surgeries, 3-0/4-0 polypropylene sutures on RB-1 and SH needles cut into 3 to 4 inches with a LAPRA-TY® at its end ready for control of an emerging vascular injury were prepared before the surgery started. Similarly, a laparoscopic bulldog vascular clamp ready on its applier and a laparoscopic Satinsky clamp were always present on the instruments table. Also, in all PC-RRPLNDs, there were 2 to 4 units of blood immediately available in the operating room.
The conversion rate in the current study is low (9%, patient 12 in Table 1) and compared favorably with previous reports 15–16 (Table 3). We attribute that only patient conversion to poor patient selection for the PC-RRPLND as the patient had a poor prognosis NSGCT. He had questionable extension of the mass into the vertebral column as well. He subsequently had internal fixation of the involved vertebral bodies by our neurosurgery team and pathology of the excised tissue from the vertebral bodies showed necrotic tissue as well. Also, this was the second patient performed after changing the approach from flank to lithotomy. In the present series, the transfusion rate was low (16.7%) and only one (8.3%) had significant postoperative complication (Clavien ≥3).
The present series, to our knowledge, is the first to include patients who underwent PC-robotic excision of residual PC mass in the seminoma patients (three patients). Although the procedure was completed safely in the three seminoma patients, the only two patients who required blood transfusion in the current series were seminoma patients. In addition, the only major complication that occurred was in a seminoma patient as well. PC-RPLND in the seminoma setting continues to be a morbid procedure. Seminoma tends to be associated with more desmoplastic reaction. The residual masses tend to be more intimately related to the great vessels, which makes dissection difficult.
A report on 97 patients who underwent open PC-RPLND in the seminoma setting from the group at Indiana University showed that often resection of the residual PC mass may not be safely completed. Almost 40% of patients required an additional procedure. 25 The average length of stay was 3.2 days in our current series. This is slightly longer to that reported by other series in the robotic PC setting (2.2 days). 15 However, our patient population is particularly complicated with more than 50% of our patients having residual PC masses 5 cm or larger (N3). The mean estimated blood loss (EBL) was 475 mL. Excluding the three seminoma patients, the mean EBL was only 202 mL in the NSGCT. This is an additional evidence of the difficulty of performing PC-RRPLND in the seminoma patients and is comparable to what was reported by Cheney and colleagues on their experience on PC-RRPLND in the NSGCT (313 mL). 15
The postoperative pathologic examination of excised LNs was positive in 5/11 patients (45.4%), either teratoma (4/11) or viable germ cells (1/11). This is similar to published data (23%–48%) in the primary RPLND and PC-setting. 26,15 Of the 10 patients in whom ejaculation was assessed, antegrade ejaculation was preserved in 9 (90%) patients. The rate of antegrade ejaculation in our study compares favorably with other series reporting on RRPLND (91%) in the PC setting. 15
The mean LN count (n = 12) was less than what was reported before in the PC-RRPLND (n = 18). 15 However, in the current study group, 6 of the LN masses excised, ≥5 cm and composed of matted LNs that our pathologist had difficulty counting, were reported as LN “mass.” The LN count is considered by some authors as an indication of the thoroughness of retroperitoneal dissection. However, most of these reports describe the LN count in the primary RPLND or NSGCT patients and with no prior chemotherapy or residual masses. In contrast to PC setting, LNs are discrete and easily counted in the primary setting. 26–27
We believe the thoroughness of dissection can be assessed as well by the surgeon's visual inspection of the surgical field at the end of the surgery with all lymphatic tissue excised and the great vessels skeletonized from the surrounding LNs. At a median follow-up of 31 months, we did not have any infield or outfield relapses. We acknowledge that this follow-up period, compared with the standard open RPLND is short. However, recurrence rates are highest in the early period following chemotherapy and RPLND; hence, most guidelines recommend intense follow-up during the early period followed by a less intense protocol. 28
Conclusions
In conclusion, we report on our experience on 12 patients who had PC-RRPLND at our academic institution. In patients undergoing PC-RRPLND, hospital stays were short, blood loss was low, and the complication rate was acceptable. Our study suffers from the limitations of small number, short follow-up, and retrospective nature. We acknowledge that PC-RRPLND is still a new procedure in urologic oncology. We acknowledge that the conclusion that PC-RRPLND is equivalent to the standard open PC-RPLND cannot be drawn from this study. Our report is more of the description of the procedure and validation of concept rather than a proof of viable procedure. It is also likely that pooled data on PC-RRPLND from various centers performing this procedure will lead to better understanding of the full oncologic outcomes of the procedure and advance this particular type of robotic surgery.
We stress these difficult procedures are not for the novice robotic surgeon and should be performed in tertiary referral centers with extensive experience in robotic surgery and high annual volume of different robotic urologic procedures.
Footnotes
Author Disclosure Statement
No competing financial interests exist.