
Abstract
Ileal ureter formation has been found to be a suitable treatment option for long, chronic ureteral strictures not amendable to less invasive forms of repair. Minimally invasive surgical techniques for this condition have been investigated. We report the first series of robotic completely intracorporeal ileal ureter using a four-arm robotic technique. Three patients underwent this procedure, including one patient with a solitary kidney. All procedures were performed effectively with a median operative time of 450 minutes (range: 420–540) and median estimated blood loss of 100 mL (range: 50–200). Postoperatively, one patient suffered volvulus and subsequent necrosis of small bowel and ileal ureter, which required re-operation and small bowel resection, including the ileal ureter. The other two patients report no surgical complications to date. This early series represents preliminary technical procedure feasibility. Further experience is necessary.
Introduction
T
An ileal ureter is a suitable treatment option for treatment of ureteral strictures. This can be utilized in patients who require complex ureteral reconstruction, due to either benign (i.e., strictures) or malignant etiologies. There have been limited reports within the literature on the use of robotics for creating an ileal ureter. 1 –3 However, further experiences of using robotics for this procedure are necessary. Herein, we provide the details and our experience of using a four-arm technique for robotic creation of an intracorporeal ileal ureter utilized at our institution.
Discussion of Technology
Three patients underwent completely intracorporeal robotic ileal ureter, with one patient having a solitary kidney. All three patients were male and two of the ileal ureters were right sided. One patient had malignant disease and each procedure included concomitant procedures, ranging from cystoscopy to antegrade nephrostogram.
Procedures were performed transperitoneally as follows (Supplementary Video 1; Supplementary Data are available online at
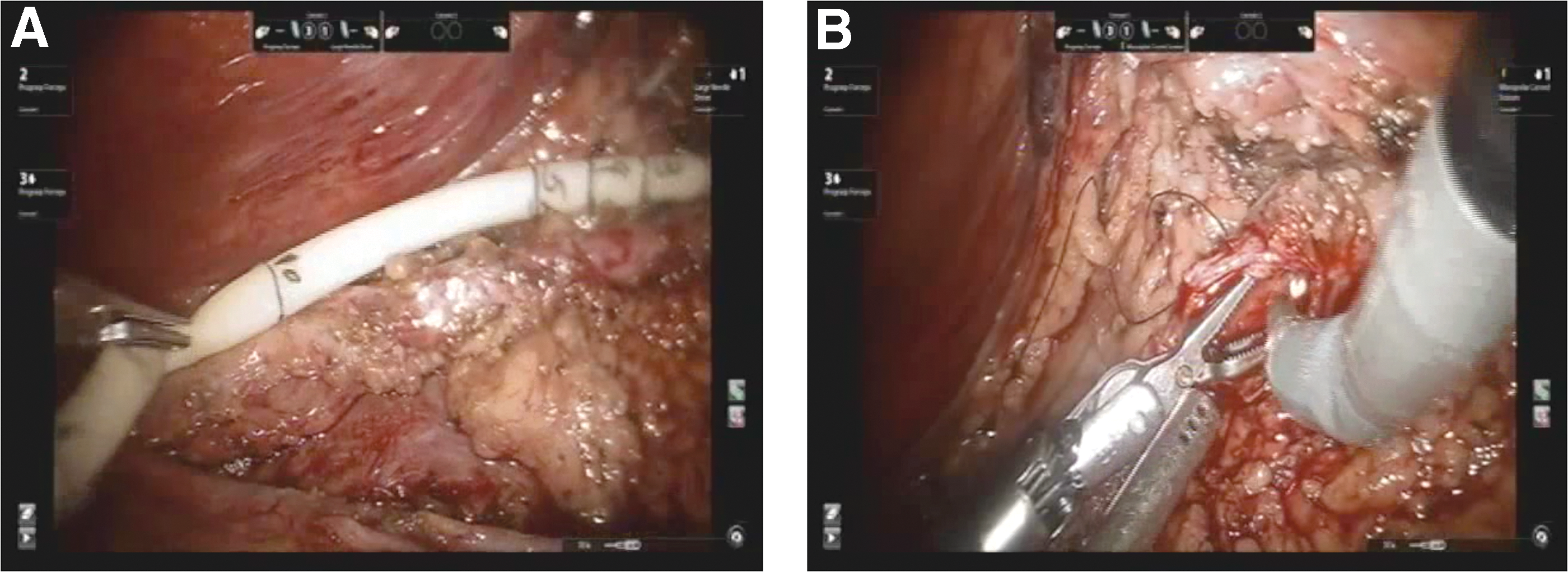
The procedure begins with mobilization of the colon medially and kocherization of the duodenum. Colon is incised at the line of Toldt and mobilized from the iliac vessels up to the splenic flexure. The ureter and gonadal vein are then identified and mobilized from the level of the pelvic brim up to the renal pelvis. The length of the ureter is measured using a previously measured Penrose drain to determine the minimum length of ileum needed to create the ileal ureter (Fig. 1A). Renal hilum is identified and the renal vein and artery are skeletonized (Fig. 1B).
The patient is then repositioned to supine lithotomy with the port placement for radical prostatectomy. 4 The bladder is first separated from the anterior abdominal wall and a psoas hitch maneuver is performed using three 2-0 Vicryl® (Ethicon, Inc., Somerville, NJ) sutures. The ileum and ileocecal valve are identified. A segment of ileum (with a minimum length of the ureter that was previously measured) is isolated at least 15 cm above the ileocecal valve and divided using Endo-GIA staplers (Fig. 2). The ends of ileum that will be used for the ileal ureter are marked using undyed 2-0 Vicryl (undyed for urinary diversion) and the ends of the gastrointestinal ileum are marked using dyed 2-0 Vicryl. Once these portions are identified, a side-to-side bowel anastomosis is performed on the portion of ileum that is marked with dyed 2-0 Vicryl using an Endo-GIA stapler.
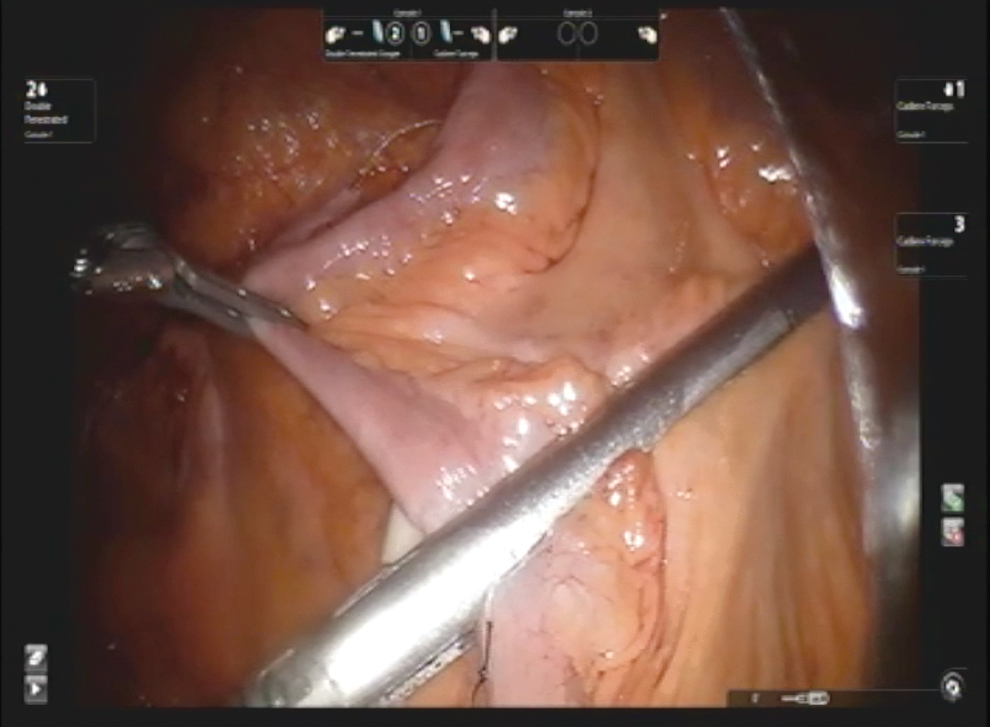
Isolation of ileum. The segment of ileum that will become the ileal ureter is divided using Endo-GIA staplers.
After isolation of the ileum, if a left ileal ureter is to be constructed, a window is required between the sigmoid and the sacrum, up to the transition between the sigmoid and the left descending colon. This allows the ileal ureter to move anatomically to the left side for formation of the left ureter. This window allows the ureter portion of bowel to be below the sigmoid and descending colon (Fig. 3A, B).
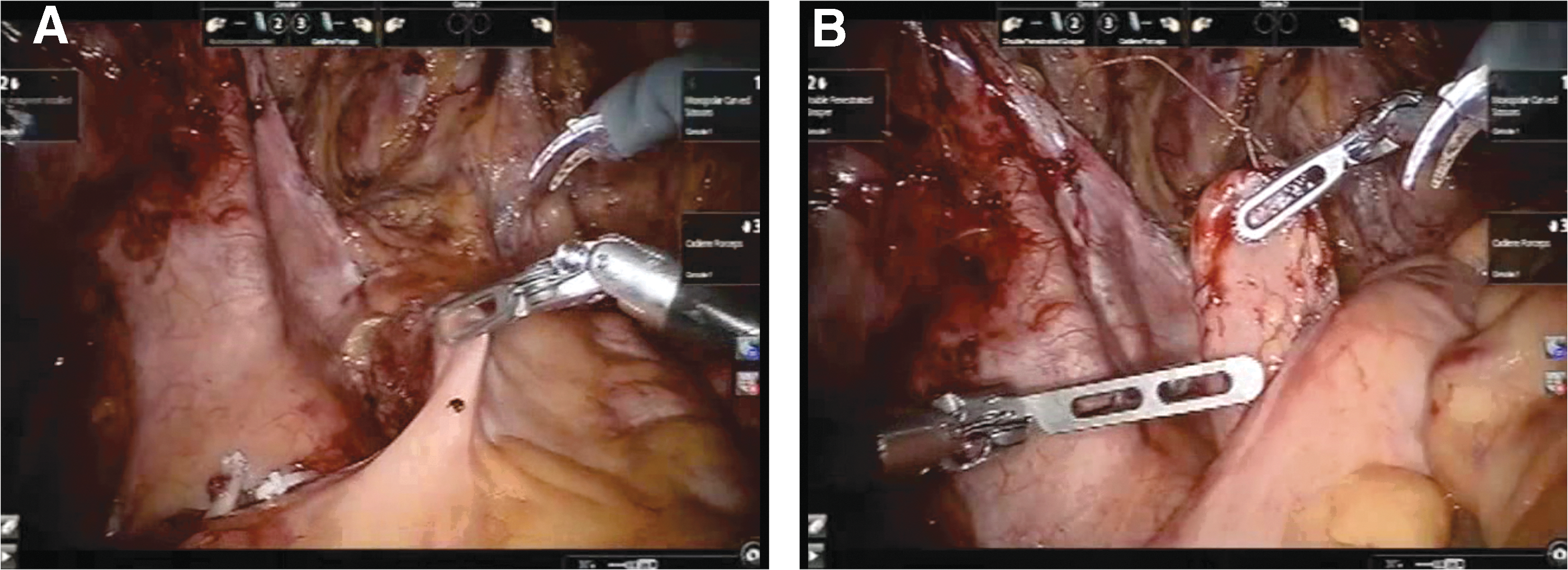
Creation of window.
The distal bowel is then anastomosed to the bladder, to maintain iso-peristalsis using a 3-0 Vicryl stitch in a running manner (Fig. 4).
Ileo-vesical anastomosis. The distal bowel is anastomosed to the bladder using a 3-0 Vicryl® stitch in a running manner to maintain iso-peristalsis.
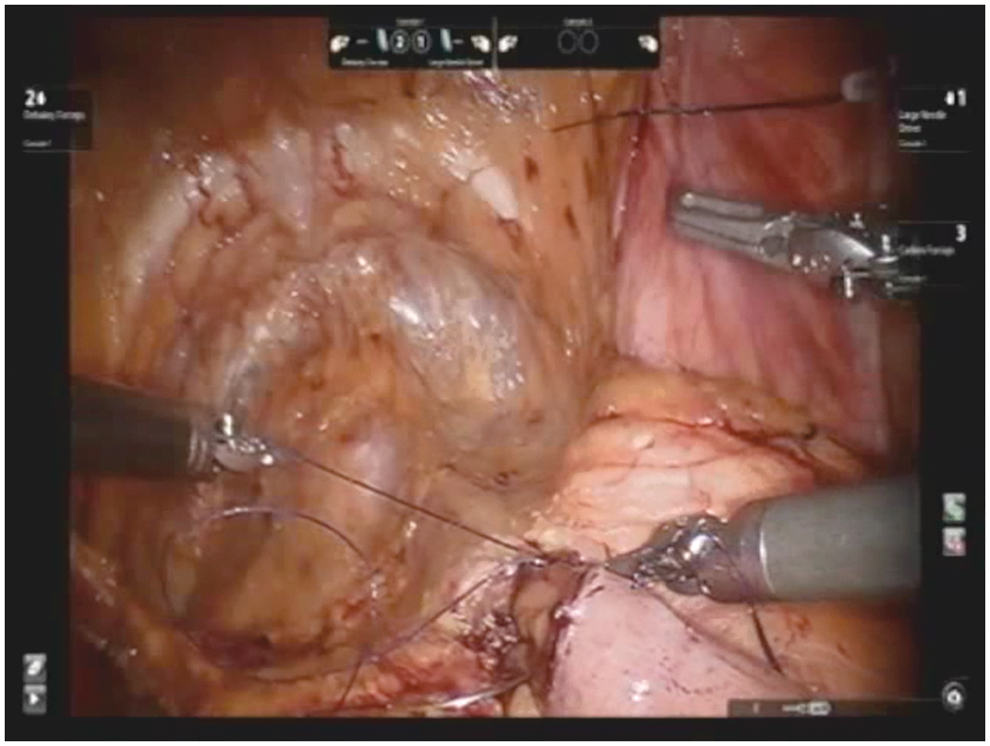
At this point, the robot is undocked and the patient is repositioned in the flank position. The ports are repositioned back to the original configuration. 4 The renal pelvis is identified and the kidney is mobilized. The renal pelvis is incised and a side-to-side anastomosis with the ileal segment and the renal pelvis is done in a running manner using 3-0 Vicryl (Fig. 5). A Double-J stent is inserted before complete closure, and indocyanine green dye is used to confirm that both the bowel and ileal segment are viable and perfused.

Ileo-pyelo side-to-side anastomosis. After incising the renal pelvis, a side-to-side anastomosis between the ileal ureter and the renal pelvis is done in a running manner using 3-0 Vicryl.
Results
Table 1 lists demographics and outcomes. Median operative time (range) was 450 minutes (420–540) and median estimated blood loss (EBL) was 100 mL (50–200). Each case underwent concomitant procedures, which included cystoscopy and antegrade nephrostogram. There were no intraoperative complications or need for blood transfusions. Median length of hospital stay (LOS) (range) was 9 days (2–12).
f, Necrosis of small bowel requiring reoperation and small bowel resection (Clavien IVa).
Patient 1 was found to have malignant transitional cell carcinoma in the original ureter that required resection and implantation of an ileal ureter. The procedure was done effectively and has reported no complications to date. On follow-up surveillance cystoscopy, he was found to have recurrence of transitional-cell carcinoma. The patient then underwent radical nephroureterectomy with excision of the ileal ureter.
Patient 2 initially reported with a solitary right kidney due to left kidney donor nephrectomy. Patient 2 was stable on discharge at postoperative day (POD) 2. On POD 3, the patient began to complain of acute abdominal pain. Computed tomography (CT) imaging revealed dilated bowel and the patient was admitted at an outside hospital. On POD 4, the patient's condition appeared to be worsening and the patient was transferred to our facility where he underwent an exploratory laparotomy. The distal ileum was herniating behind the mesentery of the ileal ureter. The herniated bowel had swollen significantly and occluded blood supply to the ileal ureter, requiring ileal ureter and bowel resection. Two months later, the appendix and cecum were used to bridge the defect in the ureter. To date, the patient reports to be doing well.
Patient 3 was ready to be discharged on POD 3. However, the patient was found to be addicted to pain medication and the pain management team was consulted to control his narcotic use. To date, Patient 3 has been healthy with no evidence of ileal ureter obstruction during a follow-up of 13 months.
Role in Endourology
We report on our initial experience of performing completely intracorporeal ileal ureter formation using a four-arm robotic approach. We describe our point of technique for this procedure, as two of three patients eventually had their ileal ureter resected. We believe that the resection of these two ileal ureters was not attributed to the use of a minimally invasive technique. With regard to the Clavien IVa complication, it is unclear as to why this complication occurred, as there was no significant mesenteric window (right ileal ureter formation). If there is one, it should be closed. We do not believe this to be attributed to the use of a robotic approach but rather a general possible complication to the procedure, as this complication has occurred previously when utilizing an open approach. 5 However, to reduce the likelihood of this complication occurring, it is important that the surgeon ensures that the bowel loops are medial to the ileal ureter and that the length of bowel for ileal ureter formation is minimized to not allow for additional ileal ureter to get tangled. There are limited reports demonstrating the use of robotics for this procedure, and this report contributes to the literature demonstrating that a robotic approach is reproducible, although initially by high-volume robotic surgeons.
Gill et al. reported the first effective laparoscopic ileal ureter case in 2000. 6 Ileovesical and pyeloileal anastomoses were performed intracorporally, while the ileum was isolated extracorporally. Since the advent of a minimally invasive technique for this procedure, other teams have sought to reproduce this technique, involving more patients and improved surgical times. 7 –11
To our knowledge, only three other groups have demonstrated the use of robotics for this procedure. The first case report in the literature occurred in 2008 by Wagner et al. 1 In this report, a modified robot-assisted technique was done. The ileal-pyelo and ileal-vesical anastomoses were performed robotically; however, an extracorporeal bowel anastomosis was utilized. The total operative time for this procedure was 720 minutes with minimal EBL and an LOS of 5 days.
Sim et al. reported on their series on intracorporeal ileal ureter replacement using both laparoscopy and robotics. 3 Five patients underwent minimally invasive intracorporeal ileal ureter formation, with one undergoing robotic intracorporeal ileal ureter. The operative time was 320 minutes with EBL of 50 mL. The patient had an LOS of 8 days and no significant complications during a follow-up of 33 months.
Brandao et al. recently reported an effective case of robotic completely intracorporeal ileal ureter in a 50-year-old gentleman with multiple strictures. 2 A three-arm robotic technique was used, with a total operative time of 420 minutes. EBL was 50 mL and the patient was discharged on day 4. The patient is reported to be stable with acceptable kidney function 2 years after surgery. Our technique uses four arms, which we believe provides better mobilization and exposure of the renal hilum. The advent of the new da Vinci Xi robotic system (Intuitive Surgical, Sunnyvale, CA) may reduce the time for this surgical procedure as the robot will not need to be redocked and instead the robotic arms can be repositioned and needs to be explored. However, we believe that the addition of the console steered table, although it may open the field for many robotic procedures, will not assist in intracorporeal ileal ureter formation. Having said that, we do not have the experience using console steered tables. Table 2 provides a summary of reported series for robot-assisted ileal interposition.
four cases were laparoscopic, one was robotic.
EBL = estimated blood loss.
Our study is not without limitations. While we experienced no intraoperative complications, one patient required ileal ureter resection within 1 week postoperation. The patient's hospital stay was uneventful and had progressed to a full diet and reported to be doing well by day 3. This small sample size's preliminary data do not demonstrate this technique to provide better functional outcomes compared with either open or pure laparoscopic techniques. It does, however, provide a description of our point of technique for a robotic approach for completely intracorporeal ileal ureter formation. For this procedure to become increasingly used, larger studies involving more institutions need to occur. At the current state, this technique at this point should be reserved for surgeons with advanced robotic skills. We believe this technique has been slow to adoption because of its inherent long procedural time (over 7 hours), the amount of bowel manipulation required, the difficult reconstructive steps (i.e. bowel resection, bowel to bowel anastomosis, bowel to bladder anastomosis, and bowel to kidney anastomosis), and the rarity of the procedure thus alluding to it more commonly occurring at tertiary referral centers. In addition, the surgeon is more likely to be familiar with complex robotic surgeries such as robot-assisted radical cystectomy with intracorporeal urinary diversion before attempting this procedure.
Conclusions
Complex robotic reconstructive procedures are still considerably challenging. In this article, we provide our point of technique for performing a robotic approach for completely intracorporeal ileal ureter formation. Further investigation is warranted.
Footnotes
Author Disclosure Statement
All authors report no disclosures relevant to the data contained within this article.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.