
Abstract
Purpose:
To report chronological trends and geographical distributions related to the prevalence of hyperoxaluria in stone-forming patients.
Materials and Methods:
We systematically reviewed the existing literature between 1982 and 2013 seeking studies that assessed for hyperoxaluria (>45 mg/day [499.5 μmol/24 hour]) in recurrent stone formers. Studies that performed 24-hour urine analysis for urine oxalate in patients with recurrent urinary stones were included. Studies were divided chronologically and by geographical region, and prevalence rates of hyperoxaluria were compared between groups.
Results:
Our literature search provided 22 peer-reviewed articles involving 3636 patients in total. Ten studies were performed between 1982 and 2000, and 12 studies were performed between 2001 and 2013. The prevalence of hyperoxaluria in stone-forming patient cohorts was 24.8% and 45.1% (p = 0.019) in studies performed between 1982 and 2000 and 2001 and 2013, respectively. Hyperoxaluria rates were significantly higher in non-American cohorts compared with American cohorts (40.7% vs 23.0%; p = 0.018). Reported hyperoxaluria rates were higher in Asian countries compared with Western countries (56.8% and 23.8%; p < 0.001).
Conclusions:
The prevalence of hyperoxaluria in stone-forming patients has increased over the past two decades and may be a contributing factor to the rising global prevalence of urolithiasis. A geographical disparity in hyperoxaluria may exist between Asian and Western countries. Future studies are needed to explain these trends and their consequences.
Introduction
O
There are several metabolic imbalances that are known risk factors for urolithiasis, including hyperoxaluria, hypercalciuria, hyperuricosuria, and hypocitraturia, gouty diathesis, and low urine volume. 8 –11 In adults, hyperoxaluria is a major risk factor for CaOx urolithiasis as high urinary levels of oxalate have been shown to lead to supersaturation and stone crystallization. 8,9,12 Mechanisms involved in hyperoxaluria may include endogenous overproduction of oxalate, high levels of dietary intake, or increased gastrointestinal absorption. 13 Additionally, previous studies have linked obesity to increased urinary excretion of oxalate 14,15 and dietary factors, such as low calcium intake, high protein intake, and high vitamin C intake, with increased serum and urine oxalate levels. 16 –18 However, long-term epidemiological trends in the prevalence rates of hyperoxaluria have largely been unexplored. Herein, we report chronological and geographical trends related to hyperoxaluria in stone-forming patients.
Materials and Methods
Search methods and identification of studies
We conducted a systematic online literature search using PubMed for peer-reviewed studies related to hyperoxaluria and urolithiasis published up to May 23, 2013. Search key words used included “hyperoxaluria,” “urolithiasis,” “prevalence,” “metabolic evaluation,” and “24 hour urine.” We included all studies reporting prevalence of hyperoxaluria based on 24-hour urine measurements of urine oxalate in adult recurrent stone-forming patients. We included studies that defined hyperoxaluria as ≥45 mg/day (499.5 μmol/24 hour) (±5 mg/day). Studies were considered nonrelevant and excluded if they included laboratory measurements in only healthy patients with no history of urolithiasis, if no 24-hour urine analysis was performed, or if the study involved only pediatric patients. We excluded review articles, but additional searches were performed based on bibliographies of relevant review articles. The literature search was performed independently by two investigators (K.S. and C.K.).
Selection of studies
We reviewed each of the articles found on our literature search in three steps. First, titles and abstracts were screened, and nonrelevant studies were excluded. Second, we evaluated full articles and excluded those with incomplete data on hyperoxaluria prevalence using 24-hour urine measurements. Our initial screening of 110 titles yielded 36 abstracts to be reviewed. After reading each abstract and applying our eligibility criteria, we excluded six nonrelevant abstracts. Of the remaining 30 full articles evaluated, 5 were excluded as nonrelevant, 2 were excluded because hyperoxaluria prevalence data could not be found, and 1 was excluded for defining hyperoxaluria as ≥60 mg/day (666 μmol/24 hour). We included a total of 22 studies that we deemed appropriate for inclusion in our systemic review (Fig. 1).
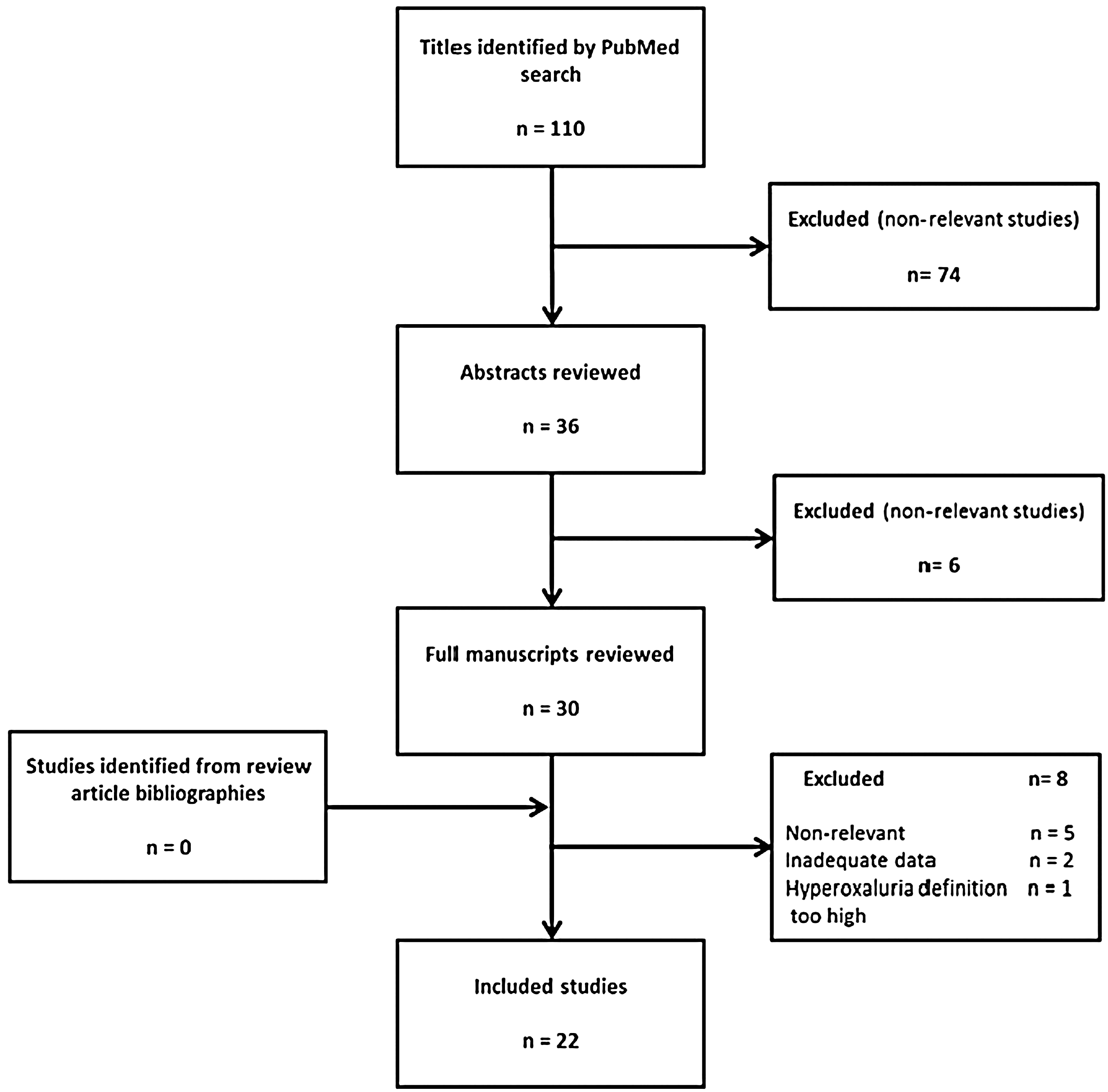
Method of study selection.
Statistical analysis
We divided the studies into two groups chronologically based on when hyperoxaluria prevalence data were collected (1982–2000 vs 2001–2013). We chose the year 2000 as the dividing year to keep the number of studies as equal as possible in each group. We also divided the studies into groups based on geographical location (US studies vs non-US studies and Asian studies vs Western studies). We compared the hyperoxaluria prevalence rates between groups. Statistical methods used included a two-tailed unpaired Student's t-test to compare prevalence rates between groups, with statistical significance set at p ≤ 0.05.
Results
The literature search provided 22 peer-reviewed articles published between 1982 and 2013 that were eligible for inclusion involving 3636 patients. 19 –39 Patient cohorts from 15 different countries were represented: 6 European countries, 6 Asian countries, 1 South American country, 1 African country, and 1 the United States (6 studies). Ten studies involving 1625 patients were performed between 1982 and 2000, and 12 studies involving 2011 patients were performed between 2001 and 2013 (Table 1).
NHS = National Health Service.
Chronological trends in hyperoxaluria
Based on the articles included in our review, overall reported prevalence rates of hyperoxaluria in stone-forming patients have increased over the past two decades. Mean prevalence rates of hyperoxaluria in stone-forming patient cohorts were 24.8% and 45.1% (3.6–56 vs 14–77; p = 0.019) in studies performed between 1982 and 2000 and 2001 and 2013, respectively (Fig. 2).
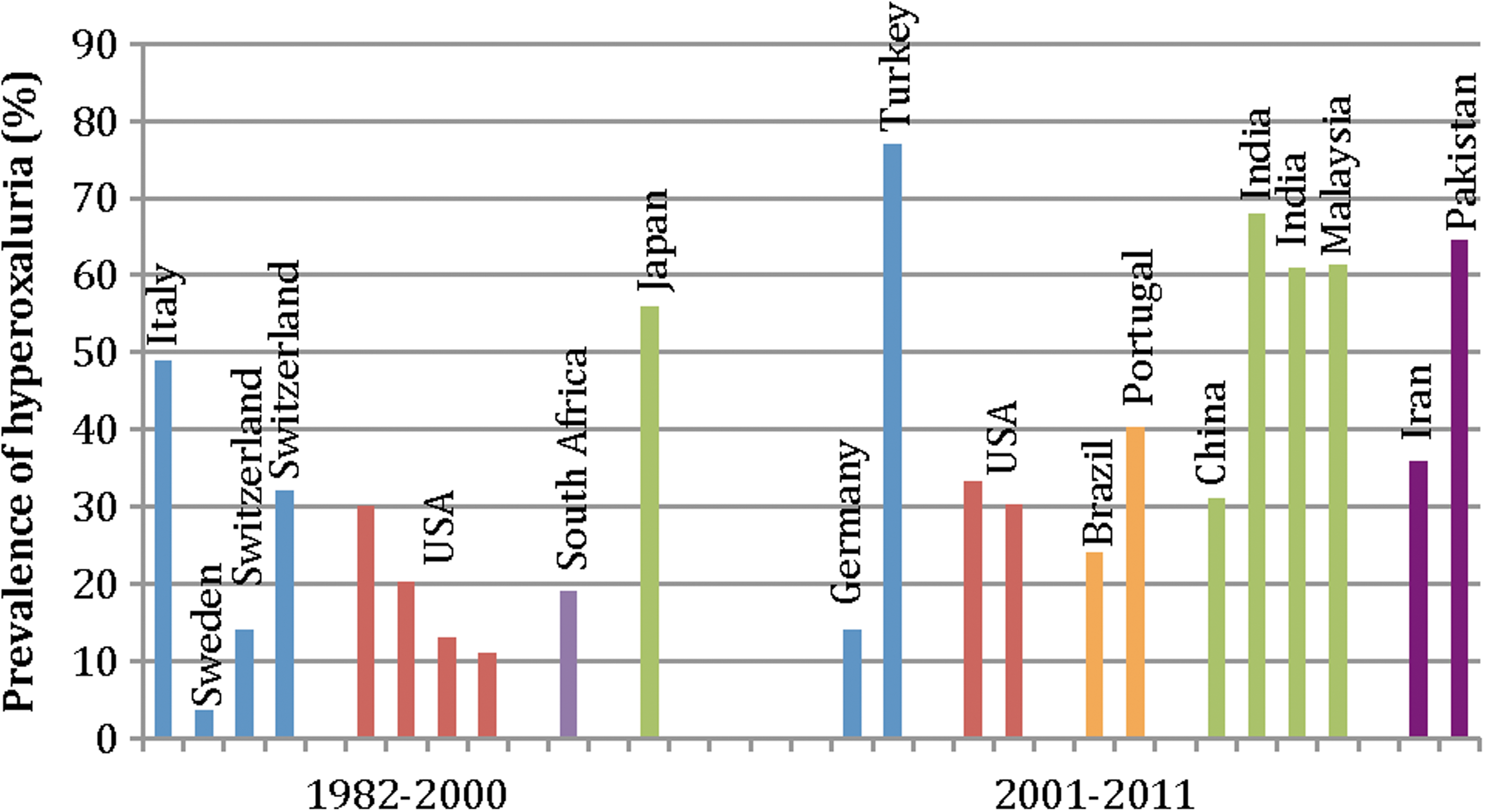
Regional prevalence rates of hyperoxaluria in stone-forming patients by year.
Geographical trends in hyperoxaluria
Overall, hyperoxaluria prevalence rates reported from abroad countries were significantly higher than those reported in U.S. studies for patients with recurrent stone disease between 1982 and 2013. Mean prevalence rates of hyperoxaluria in U.S. patient cohorts and foreign cohorts were 23.0% and 40.7% (11–33.3 vs 3.6–77; p = 0.018), respectively (Fig. 3). Reported hyperoxaluria prevalence rates were higher in Asian countries compared with Western countries. Average prevalence rates of hyperoxaluria in Asian and Western cohorts were 56.8% and 23.8% (31–77 vs 3.6–49; p < 0.001), respectively. Individual countries reporting the highest prevalence rates included Turkey (77%), India (64.5%), Pakistan (64.5%), and Malaysia (61.4%).
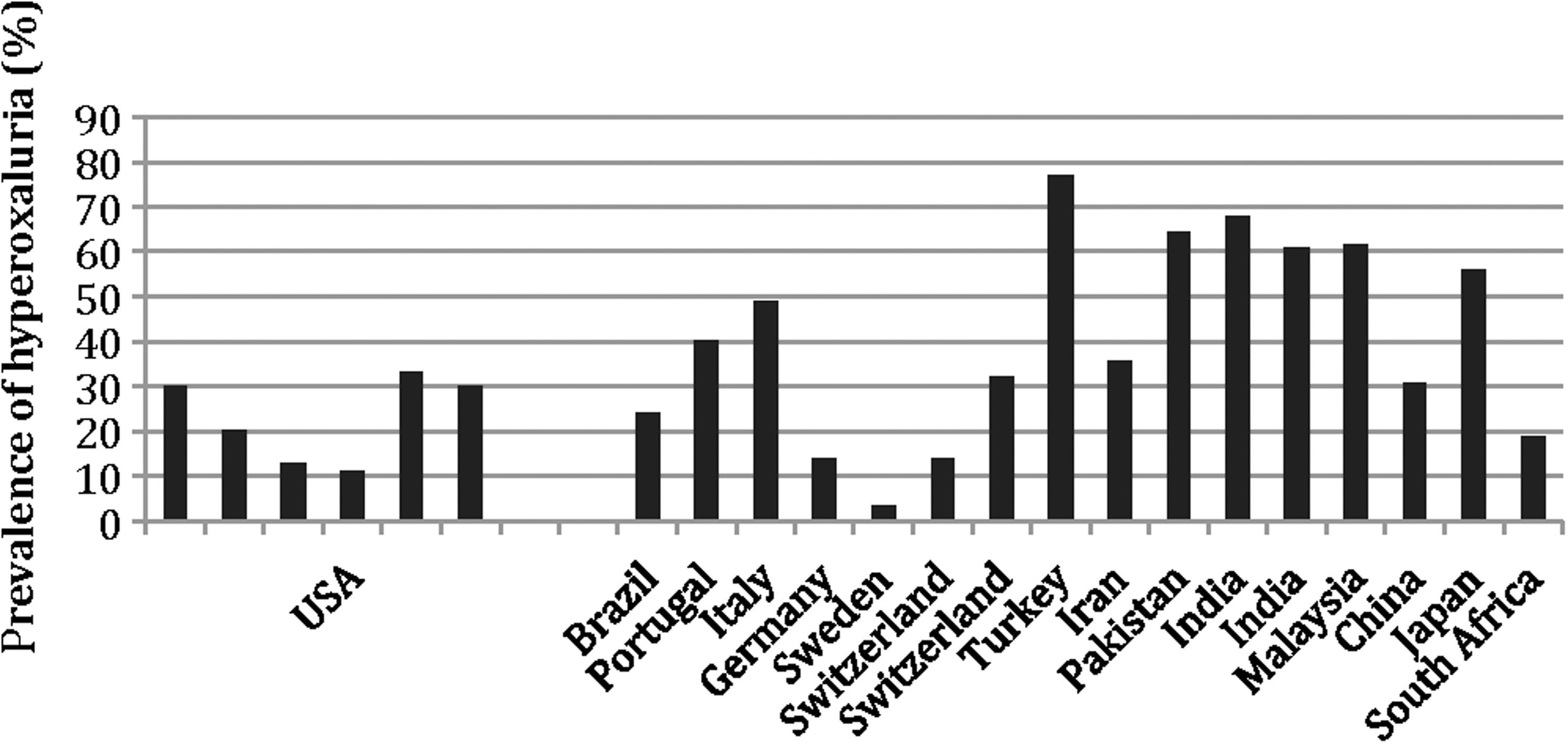
Prevalence of hyperoxaluria in stone-forming patients by nationality.
Discussion
Hyperoxaluria is one of the many factors that promotes the formation of calcium stones; however, its influence on stone disease has been shown to be particularly important in adult recurrent stone formers. 1,12 The mechanism underlying CaOx stone formation is multifactorial. 1,5,8,9 Mechanisms underlying increased urinary excretion of oxalate may include inborn errors of metabolism, leading to overproduction of endogenous oxalate, or excessive dietary intake or intestinal absorption, leading to increased bioavailability of oxalate. 13
Our findings suggest that a rising prevalence of hyperoxaluria may be a contributing factor in the overall increasing prevalence of nephrolithiasis. Based on our literature search, the reported prevalence of hyperoxaluria among recurrent stone formers has increased from 24.8% during the 1980s and 1990s to more than 45% from 2001 to 2013. This increase coincides with an overall increase in the United States stone disease prevalence from 5.2% to 8.8% in the past 20 years. 1 Given the multistep mechanism of stone formation and numerous metabolic factors involved, it is unlikely that oxalate levels are solely responsible for chronological changes in stone disease prevalence. It is, however, likely that hyperoxaluria constitutes a piece of this etiological puzzle. Additional prospective studies are needed to confirm and quantify the implications of epidemiological changes in hyperoxaluria prevalence and overall rates of nephrolithiasis.
While the primary purpose of our review was to describe apparent epidemiological trends in a major metabolic risk factor for calcium stone disease, we hope that these observations may serve as a foundation for future investigations to determine etiologies for rising rates of hyperoxaluria and urolithiasis. Recently, a growing body of evidence suggests that the higher prevalence of stone disease may be linked to changes in dietary or lifestyle factors. 40 Obesity and metabolic syndrome have been shown to be associated with increased risk for kidney stone disease. 2,41 Furthermore, a large retrospective study by Powell and colleagues found that obese patients had significantly higher levels of oxalate in their urine compared with nonobese patients. 15 Given that more than two thirds of adult Americans are currently overweight or obese, 42 this association between obesity and stone disease may provide a reasonable explanation for the increasing prevalence rates of urolithiasis.
Other dietary factors should be considered in the context of hyperoxaluria. While dietary intake of oxalate-rich foods, such as fruits and vegetables, has not been shown to have a significant impact on urinary excretion of oxalate, 16,43 diets high in protein and low in calcium have been associated with hyperoxaluria. 17 A 5-year randomized trial demonstrated that a low-calcium diet resulted in reduced calcium binding to oxalate in the gut, leading to increased gut absorption and increased urinary excretion of oxalate. 17 Their findings also supported previous findings that diets high in animal protein may lead to increased endogenous production of oxalate. 44 Indeed, in a comprehensive review comparing the dietary characteristics of patients in the Gulf States with their Western counterparts between 1980 and 1990 demonstrated that oxalate consumption in the Gulf States was three times as high, while calcium consumption was just half. In this review, Robertson concluded that this imbalance led to enteric hyperoxaluria, which when coupled with increased animal protein consumption and low urine volumes resulted in high incidence of uric acid and CaOx stones. 45 Finally, high dietary intake of vitamin C is associated with increased urinary excretion of oxalate and may also be a contributing factor to a rise in hyperoxaluria prevalence. Daily vitamin C supplements (2000 mg/day) were associated with a 22% increase in urinary oxalate excretion. 18 Since 1994, there has been a 30% increase in multivitamin use in the United States, with nearly half of Americans now using dietary supplements. 46 Between 1986 and 2000, the percentage of daily vitamin C intake from fortified beverages has also increased from 5% to 60%. 47 Excessive vitamin C intake may be partly responsible for the rising trends in hyperoxaluria, but long-term trends in supplemental vitamin C intake have been largely unexplored.
Increased availability and utilization of radiologic imaging, such as CT, may be a contributing factor to the rising prevalence of stone disease. In the United States, the use of CT imaging has increased nearly 20-fold over the past 20 years. 48 This improved capacity to diagnose incidental or clinically insignificant calculi may play a part in the increasing stone prevalence globally. However, previous analyses of patient-reported stone passage rates have also demonstrated an increasing prevalence of urolithiasis unrelated to radiologic imaging. 2 Similarly, improvements in metabolic testing technology or increased utilization of urine metabolic tests may be contributing factors for the observed increasing trends in prevalence rates of hyperoxaluria over the past two decades. Increased emphasis in recent years on stone prevention and metaphylaxis in stone-forming patients may lead to increased urine testing and increased detection of hyperoxaluria. Additional epidemiological studies evaluating trends in metabolic testing utilization are needed to assess for potential detection biases.
Geographic variability in the prevalence of kidney stone disease has been previously described. 49,50 In the United States, higher average temperatures, higher sunlight indices, and lower latitudes have been shown to be independently associated with stone prevalence. 51 –53 In fact, recent studies have proposed that global warming may play a role in the growing prevalence of nephrolithiasis worldwide. 54 To our knowledge, no previous study has reported global geographical differences in hyperoxaluria prevalence rates. Our findings suggest that the prevalence of hyperoxaluria is highest in Asian stone-forming cohorts and significantly lower in American cohorts. Plausible explanations for this disparity may include genetic factors, climate-related factors, dietary or lifestyle factors, or other environmental factors, such as hardness of drinking water. 53 Additional long-term studies, including larger numbers of patients from many geographical regions, are needed to further elucidate causes for geographical differences in hyperoxaluria or urolithiasis.
Our study has some limitations. The articles included in our review were heterogeneous in nature, and we did not account for variations in patient demographic factors, such as gender, race, or age. For instance, US studies favored female predominant cohorts, especially the National Health Service studies, which consisted of all female health workers. The prevalence of stone disease is higher among males, suggesting that there may be important differences among males and females. As a result, the generalizability of our findings may be limited. Additionally, methodological differences in both analytical and urine sample handling might have influenced the reported prevalence of hyperoxaluria in the cited studies. Finally, our search did not uncover studies indicating prevalence rates from Turkey, Pakistan, India, and Malaysia between 1982 and 2000, the four countries for which the highest prevalence rates were reported between 2001 and 2013. It is possible that prevalence rates in these countries were also relatively high in the past, and therefore, it is difficult to assess the magnitude and significance of the chronological increase in prevalence of hyperoxaluria observed. Furthermore, our literature search yielded few US cohort studies published in the past 10 years. More recent data on American stone-forming cohorts are needed to accurately assess chronological trends in the United States.
Conclusions
The prevalence of hyperoxaluria in stone-forming patients has increased over the past two decades and may be a significant contributing factor to the rising global prevalence of urolithiasis. A global geographic disparity in hyperoxaluria appears to exist, with higher prevalence rates in Asia. Future studies are needed to explore these epidemiological trends in hyperoxaluria and their impact on the prevalence of urolithiasis.
Footnotes
Author Disclosure Statement
No competing financial interests exist.