
Abstract
Objective:
To evaluate the effectiveness of a polymeric flap valve-attached ureteral stent for preventing vesicoureteral reflux (VUR) in an animal model.
Materials and Methods:
One female Yorkshire pig was included in this study. A flap valve-attached and a conventional stent was inserted in the right and left ureters, respectively. The bladder was filled with contrast medium until the intravesical pressure reached 20 cm H2O. Subsequently, simulated voiding cystourethrography (VCUG) was performed 50 times by manually compressing the suprapubic area until the intravesical pressure reached 50 cm H2O. Intravenous pyelography (IVP) was performed thereafter to evaluate the urinary drainage. In addition, an in vitro durability test of the function of the flap valve was conducted under continuous hydrostatic pressure for 24 h.
Results:
The volume of contrast medium needed to achieve an intravesical pressure of 20 cm H2O was 1740 mL. In the repeated simulated VCUG for the right ureter, VUR grades of 0 and I were recorded in 82.0 (n = 41) and 18.0% (n = 9) tests, respectively, whereas for the left ureter, grades of I, II, and III were recorded in 14.0 (n = 7), 82.0 (n = 41), and 4.0% (n = 2), respectively. Thus, a significantly lower VUR grade was recorded for the right ureter than for the left ureter (p < 0.001). In the bilateral VUR condition, the pressure for VUR occurrence was significantly greater in the right ureter than in the left ureter (p = 0.007). No urinary obstruction was caused by the flap valve-attached ureteral stent according to the IVP findings. The in vitro durability test demonstrated slightly enhanced antireflux function and slightly decreased intraluminal drainage at 12 h, and these findings sustained thereafter.
Conclusion:
A flap valve-attached ureteral stent effectively prevented VUR under conditions of elevated intravesical pressure without urinary obstruction.
Introduction
U
Despite the benefit and wide usage of ureteral stents, several side effects such as dysuria, bladder irritation, and flank pain are frequently encountered after stent insertion. 11,12 Vesicoureteral reflux (VUR) is a critical side effect that causes flank pain in patients, following ureteral stent insertion. The flank pain observed in patients with VUR is believed to be caused by the pressure in the renal pelvis generated by urine reflux under conditions of elevated intravesical pressure, such as micturition. 13,14 VUR may also be a rare predisposing factor for urinary tract infection and renal parenchymal scarring. To reduce VUR, several research groups have sought to develop antireflux ureteral stents. 15 –18
Our group has also been attempting to develop antireflux ureteral stents for the past few years. In our prior work published in 2015, 19 a flexible polymeric flap valve that can be attached at the vesical edge of a conventional ureteral stent was introduced to prevent VUR. The flap valve was fabricated efficiently and easily using a three-dimensional (3D) printer.
We conducted in vitro tests to evaluate the antireflux function and intraluminal drainage capability of the flap valve-attached ureteral stent in comparison with a conventional ureteral stent. In this in vitro study, anterograde and retrograde hydrostatic pressure were applied to both stents using deionized (DI) water, and the intraluminal flow rates of DI water were measured. The results demonstrated that the flap valve-attached ureteral stent reduced the simulated reflux by fourfold compared to the conventional ureteral stent, concurrently with a slightly decreased (from 22.2 to 20.0 mL/min), but sustained anterograde intraluminal flow rate of DI water. This in vitro study demonstrated the high potential of flap valve-attached ureteral stents for reducing VUR under elevated intravesical pressure conditions, while maintaining ureteral urinary drainage without obstruction.
As an extension of the prior study, 19 in the present study, we conducted a pilot in vivo test using a porcine model to evaluate the VUR prevention efficacy of a flap valve-attached ureteral stent. The VUR findings between the two ureters, with a flap valve-attached ureteral stent inserted into one ureter and a conventional ureteral stent inserted into the other, were compared under elevated intravesical pressure conditions in the porcine model. An additional in vitro study to evaluate the durability of the flap valve function was also conducted by applying continuous hydrostatic pressure for 24 h at the distal end of the flap valve-attached ureteral stent.
Materials and Methods
Two identical 6F/28 cm ureteral stents (BARD® INLAY™ Double Pigtail Stent; C. R. Bard, Inc.) were used in the present study. A polymeric flap valve was attached to one of the stents at the vesical edge (Fig. 1), whereas the other stent lacking a flap valve was used as a conventional stent. The flap valve was fabricated by a stereodeposition process in a 3D printer (Objet500 Connex printer; Stratasys Ltd.) using a computer-aided design. Flexible Tango-Plus FLX980 (tensile strength of 1.50 MPa, elongation at break of 218%, hardness 27 Shore A) was used as the material of the flap valve. The surface of the flap valve was coated with parylene C (1 μm thickness) using low-pressure chemical deposition to enhance the biocompatibility. The specific dimensions and detailed fabrication method of the flap valve were described in our prior published work. 19
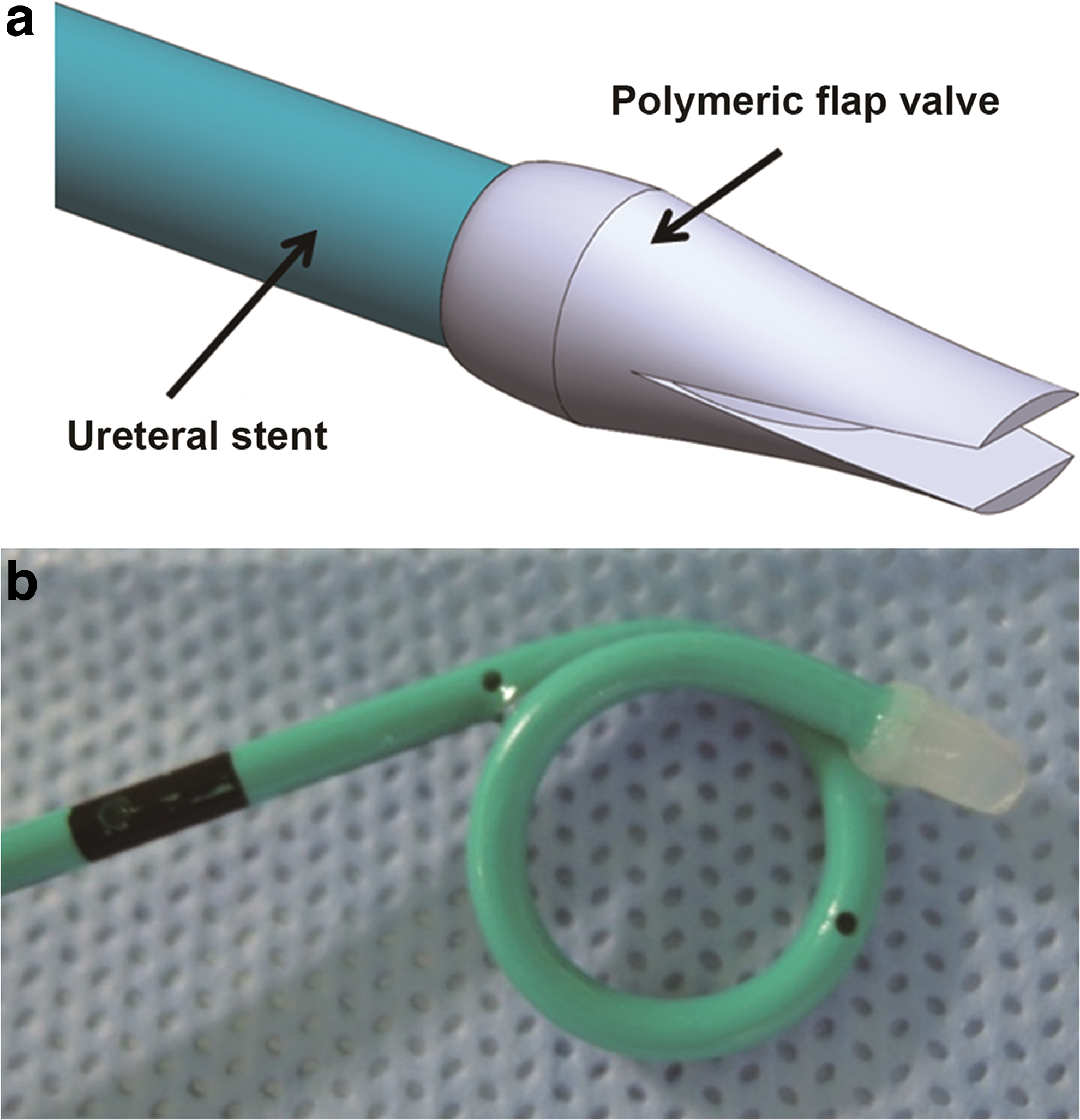
The schematic
In vivo study: flap valve evaluation in a porcine model
A female Yorkshire pig (49 kg) was prepared under general anesthesia for the study. Before insertion of the ureteral stents, intravenous pyelography (IVP) and simulated voiding cystourethrography (VCUG) were performed to check for the urinary tract anomalies. Once the contrast medium for the two tests was completely drained from the collecting system, the ureteral stents were inserted.
The flap valve-attached and conventional ureteral stents were inserted in the right and left ureters, respectively, using a 7.5F semi-rigid ureteroscope (Karl Storz). The detailed sequence of ureteral stent insertion in the porcine model was as follows: (1) the ureteroscope was inserted into the ureter retrogradely; (2) once the ureteroscope reached the renal pelvis, a guidewire was inserted through the ureteroscope until it reached and coiled in the renal pelvis; (3) the ureteroscope was removed from the pig, leaving the guidewire within the ureter; and (4) a ureteral stent was inserted into the ureter by following the guidewire, using X-rays to verify the proper stent placement. Because of the narrow porcine urethra and difficulty in inserting the guidewire reaching to the porcine renal pelvis, ureteroscopy was an appropriate choice for ureteral stent placement without causing any injuries.
Simulated VCUG, as described by Lumiaho et al. 15 was performed after the stent insertion. The bladder was filled with a 50% diluted solution of 300 mg/mL iohexol through a 14F silicon Foley catheter (Medline) until the intravesical pressure reached 20 cm H2O. Subsequently, simulated micturition was performed by manually compressing the suprapubic area until the intravesical pressure reached 50 cm H2O; thereafter, the pressure was maintained for 60 s. 15,16 To measure the intravesical pressure, a suprapubic puncture was performed using a spinal needle (18G) connected to a digital pressure gauge (ADT 681; Additel Corporation). Simulated VCUG was performed 50 times to evaluate the flap valve function by comparing the VUR findings for both ureters. Each simulated VCUG trial was performed after the contrast medium from the previous trial was removed.
The VUR findings were graded according to the international system of radiographic grading of VUR 20 as follows: grade 0 = no reflux; grade I = reflux into the nondilated ureter only; grade II = reflux into the pelvis and calyces without dilatation; grade III = mild to moderate dilatation of the ureter, renal pelvis, and calices, with no or slight blunting of the fornix; grade IV = moderate dilatation and/or tortuosity of the ureter and moderate dilatation of the renal pelvis and calices; and grade V = gross dilatation and tortuosity of the ureter, renal pelvis, and calices, with a loss of papillary impressions.
The pressures at which VUR occurred were compared between the two ureters in the simulated VCUG trials of bilateral VUR. IVP was also performed after emptying the bladder to evaluate whether the flap valve-attached ureteral stent caused urinary obstruction. The present in vivo study was approved by the international review board of animal experiments of the Pusan National University Yangsan Hospital (approval number: PNUYH-2014-027).
In vitro study: flap valve durability test
The in vitro durability test of the flap valve-attached ureteral stent was performed for 24 h. Hydrostatic pressure was continuously applied using DI water at 50 and 20 cm H2O to the distal (valve side) and proximal parts of the stent, respectively, with pressure applied to each part in sequence for 1 min each. A pressure of 50 cm H2O is similar to the increased intravesical pressure during micturition, and a pressure of 20 cm H2O is similar to the normal anterograde urinary flow pressure from the renal pelvis to the bladder. 21 A commercial pressure transducer (ADT 672; Additel) was used to confirm the hydrostatic pressure, and an electronic balance (PAG214; PRESTO Testing Instrument) was used to measure the retrograde and anterograde intraluminal DI water flow rates of the stent. The details of the experimental setup and procedure were identical as those in our prior published in vitro study. 19
Statistical analysis
Fisher's exact test was used to analyze the differences in VUR findings depending on the type of ureteral stent. The pressure at which VUR occurred in the simulated VCUG trials that showed bilateral VUR was compared between the ureters using the Mann–Whitney U test. A p-value < 0.05 was considered statistically significant. All statistical calculations were computed using PASW Statistics 18 (SPSS, Inc.).
Results
In vivo study: flap valve evaluation in a porcine model
Urinary tract anomalies were not observed in the IVP and simulated VCUG experiments before ureteral stent insertion. The volume of contrast medium needed to achieve an intravesical pressure of 20 cm H2O was 1740 mL, and no VUR was observed at this volume in either ureter.
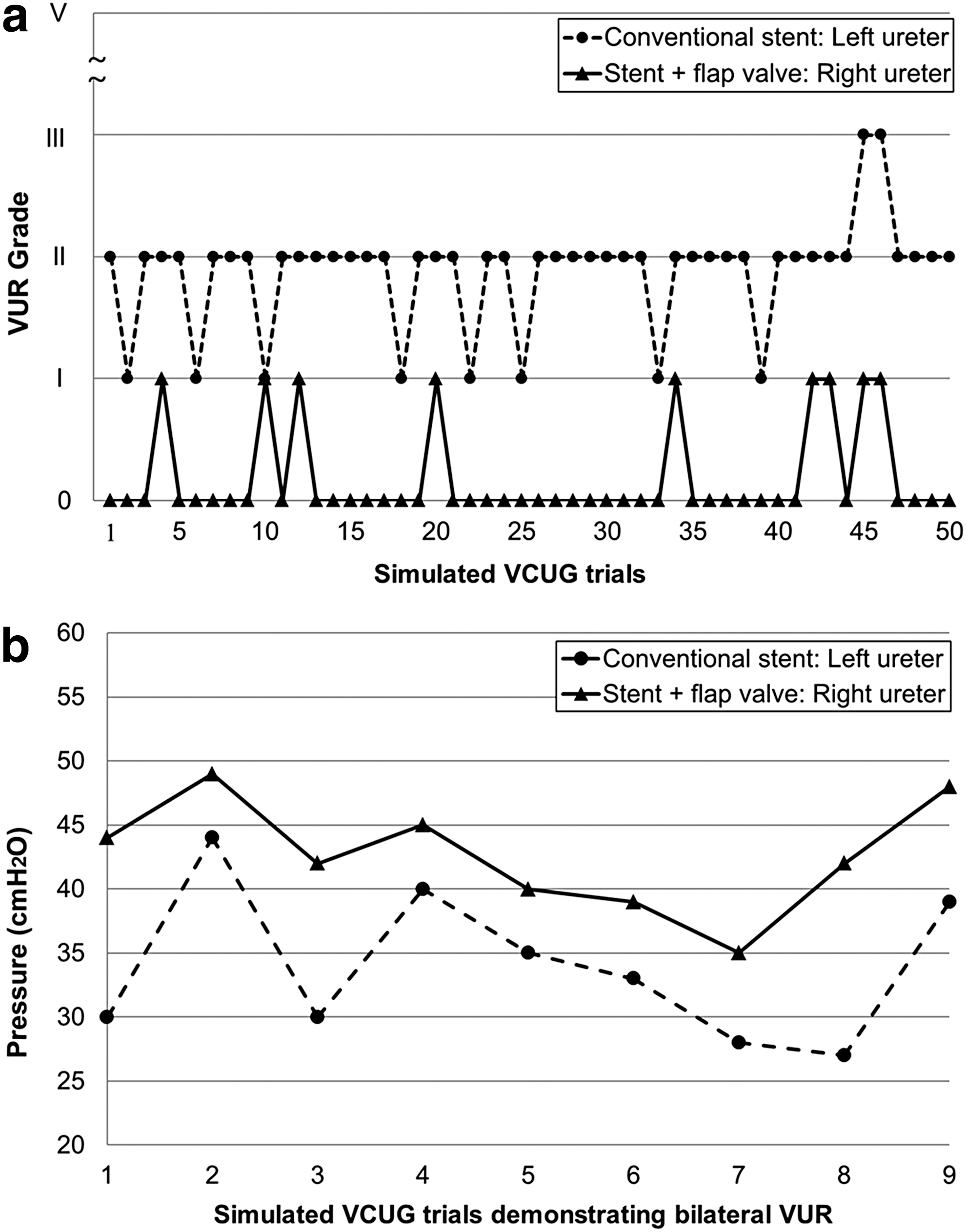
The 50 repeated simulated VCUG trials revealed the following findings: On the right ureter, which had an inserted flap valve-attached stent, VUR grades of 0 and I were recorded in 82.0 (n = 41) and 18.0% (n = 9), respectively; on the left ureter, which had an inserted conventional ureteral stent, VUR grades of I, II, and III were recorded in 14.0 (n = 7), 82.0 (n = 41), and 4.0% (n = 2), respectively (Table 1). These VUR findings were significantly different depending on the type of ureteral stent (p < 0.001); specifically, a lower VUR grade was obtained in most of the VCUG trials for the right ureter than that obtained for the left ureter (Table 1). The VUR findings for both ureters in all 50 simulated VCUG trials are plotted in Figure 2a.
VUR = vesicoureteral reflux.
The pressures at which VUR occurred in each ureter in the nine experiments that showed bilateral VUR are plotted in Figure 2b. Significantly higher pressure tended to be required to cause VUR in the right ureter than that required to cause VUR in the left ureter (mean: 42.67 ± 4.42 vs 34.01 ± 5.92 cm H2O; p = 0.007). In addition, the mean pressure at which VUR occurred in the left ureter during the 50 repeated simulated VCUG trials was 34.16 ± 4.64 cm H2O. The IVP findings after the simulated VCUG demonstrated proper urinary drainage in the right ureter, indicating that the flap valve-attached ureteral stent does not inhibit urinary drainage.
We had no difficulties during the insertion and removal of the flap valve-attached ureteral stent in the present porcine model. The condition of the flap valve was checked immediately after removal from the porcine ureter at the end of the in vivo study, and no grossly damaged region was found.
In vitro study: flap valve durability test
The experimental results of the 24-h durability test for the flap valve-attached ureteral stent indicated that the retrograde and anterograde intraluminal flow rates of DI water decreased slightly over the initial 12 h of the study (from 15.42 to 12.54 mL/min and from 27.65 to 26.38 mL/min, respectively), and the flow rates were sustained without further decrease for the remainder of the test (Fig. 3). The declines of the retrograde and anterograde flow rates of DI water through the stent over the initial 12 h were approximately −14.38 and −6.35 mL/h 2 , respectively. No grossly damaged region in the flap valve was found after the in vitro study.

The 24-h durability test of the flap valve-attached ureteral stent using deionized water; the retrograde and anterograde pressures applied during the test are 50 and 20 cm H2O, respectively.
Discussion
The flap valve used in the present study functions because of the applied hydrostatic pressure difference. 19 In an empty bladder state, the anterograde pressure applied from the renal pelvis is higher than the retrograde pressure applied from the bladder. This pressure difference causes the flexible flap valve to open and enables urine to flow in an anterograde direction from the renal pelvis to the empty bladder. During micturition, however, the intravesical pressure is higher than the anterograde pressure applied from the renal pelvis. This causes the flap valve to be closed and sealed, preventing urinary reflux induced by the channel of the indwelled ureteral stent. 19
As observed in most of the simulated VCUG trials in the present study, the flap valve-attached ureteral stent effectively prevented VUR, excluding the nine trials in which grade I VUR was observed in the right ureter. Despite the presence of VUR in nine trials, the results in these trials revealed lower VUR grades (Fig. 2a) and a significantly higher pressure required to induce VUR (Fig. 2b) in the right ureter with the flap valve-attached ureteral stent compared to the findings in the left ureter, in which a conventional ureteral stent was inserted. These results imply that under the conditions of elevated intravesical pressure, the polymeric flap valve can suppress the VUR-inducing nature of ureteral stents to a certain extent.
Other studies introducing antireflux valves attached to the distal orifice of ureteral stents have also reported successful VUR prevention. An ex vivo study conducted in 199316 evaluated the antireflux function of a ureteral stent with a wiruthane membrane valve. The valve consisted of two membranes that compressed under elevated intravesical pressure. The ureteral stent with a wiruthane membrane valve was inserted into a canine urinary system, and micturition was simulated by applying manual pressure of 50 cm H2O at the bladder. The renal pelvic pressure was measured during the simulated micturition by a nephrostomy tube that was placed in the renal pelvis. The results demonstrated lower pressure peaks and a significantly delayed increase in renal pressure for the ureteral stent with a wiruthane membrane valve compared to the findings for the conventional stent. This finding implies that the membrane valve reduced and delayed pressure transmission from the bladder to the renal pelvis, thereby reducing urinary reflux during micturition.
Another study using a membrane valve coupled to a ureteral stent was reported in 2010. 17 According to the study, significantly greater numbers of patients who received a ureteral stent with a membrane valve exhibited a lower grade of hydronephrosis and lesser flank pain during micturition than those who received a normal stent.
A study reported in 201218 assessed the functional efficacy and stent-related symptoms of an antireflux ureteral stent by performing poststenting cystography and asking patients to complete a ureteral stent symptoms questionnaire (USSQ), respectively. The new stent had a synthetic cone-shaped valve around the distal tip, which collapsed and occluded the stent channel under elevated intravesical pressure during micturition. The patients who received a ureteral stent with a cone-shaped valve displayed less reflux in the cystography findings and a lower mean USSQ score than those who received the conventional stents. These studies support our findings that VUR in the ureteral stent-inserted condition can effectively be reduced using antireflux valves.
According to the in vitro durability test results of the present study, the flap valve-attached ureteral stent was associated with slightly decreased retrograde and anterograde flow rates for intraluminal DI water after the first 12 h of the test (Fig. 3). Assuming that these results are also observed in the stent-inserted state in patients, the antireflux function of the stent should be slightly enhanced, whereas the intraluminal urinary drainage from the renal pelvis to the bladder should be very slightly inhibited 12 h after stent insertion. Although the anterograde drainage function of the stent may be slightly decreased, the anterograde intraluminal flow rate of DI water after 12 h of the test was sufficiently high to overwhelm the normal anterograde urinary flow rate from the renal pelvis to the bladder through the ureter (0.5 mL/min at 15–18 cm H2O).
Decreased flow rates of DI water are expected to be induced by the micropores of the polymeric flap valve. The micropores may absorb water in an aqueous environment, leading to a slight swelling of the polymers and, consequently decreasing the flexibility of the polymeric flap valve.
The present study has a few limitations. First, we used only a single porcine model and flap valve-attached ureteral stent in this study. It is obvious that larger numbers of animal models are necessary for more precise and reliable results to evaluate the efficacy of flap valve-attached ureteral stents. To compensate for the small sample size to a certain extent, the simulated VCUG test was repeated 50 times in this study. Although repeating the test alone may not be sufficient to ensure robustness of the results, we could at least verify the repeatability and enhance the reliability of the flap valve function.
Second, although ureteral stents are placed in patients for weeks in practice, the present in vitro durability test was performed for only 24 h. In other words, the duration of in vitro durability test was short compared with the ureteral stent insertion period in actual practice. However, sustained DI water flow rates were observed over the last 12-h duration of the test (Fig. 3), and this result contributed to the decision that extension of the in vitro test beyond 24 h may be pointless. In addition, retrograde pressure was applied to the flap valve over 700 times during the 24-h period. If retrograde pressurization for 1 min is considered one micturition event, more than 700 micturition events were simulated during the in vitro study. Regarding the mechanical function of flap valve, more than 700 simulated micturition events are believed to be a substitute for long-term durability testing to a certain degree. Nevertheless, a long-term in vivo test for the precise durability evaluation of the flap valve remains necessary.
Conclusions
In the present study, the flap valve-attached ureteral stent effectively prevented VUR under the conditions of elevated intravesical pressure in a porcine model. In addition, the urinary drainage of the stent-inserted ureter was unobstructed by the presence of the flap valve. However, the present pilot study requires supplementations, especially considering the aforementioned limitations. For further studies, long-term evaluations on a larger number of animal models with flap valve-attached ureteral stents inserted are necessary to obtain more reliable and precise results. Additional in vivo evaluations of valve obstruction by biofilm and sticky obstruction by the flap will also be useful.
Footnotes
Acknowledgments
This work was supported by the Basic Research Projects in High-tech Industrial Technology by a grant provided by GIST in 2015 and a 2-year research grant from Pusan National University.
Author Disclosure Statement
No competing financial interests exist.