
Abstract
Background and Objectives:
Salvage prostate cryoablation is an effective treatment for patients with localized prostate cancer relapse following primary radiotherapy. The postsalvage prostate-specific antigen (PSA) nadir that best predicts long-term biochemical progression-free survival (bPFS) is not yet defined. We sought to determine what nadir PSA best predicted success following salvage whole-gland cryoablation.
Patients and Methods:
We retrospectively reviewed a cohort of 486 hormone-naive patients who underwent salvage whole-gland cryoablation from the Cryo On-Line Database (COLD). Studied variables were age, race, initial PSA, presalvage prostate-specific antigen (psPSA), initial Gleason score, Gleason score at presalvage biopsy, clinical stage, and follow-up PSA values. Kaplan–Meier (KM) analysis was used to calculate 5-year bPFS using the Phoenix criteria. Hazard ratio and relative risk were also analyzed. Differences among the KM estimates, at 5 years, were calculated using the log-rank test.
Results:
Using group thresholds, KM analysis identified nadir PSA less than or greater than 0.4 ng/mL as the nadir PSA threshold, with the greatest difference in bPFS. The KM estimated 5-year bPFS was 75.5% and 22.1% for nadir PSA <0.4 and ≥0.4 ng/mL, respectively. Stratified by psPSA, the KM estimated 5-year bPFS comparing patients with PSA nadir <0.4 vs ≥0.4 ng/mL was 78.5% and 17.9% (p < 0.0001) for psPSA <4 ng/mL, 77.1% and 15.7% (p < 0.0001) for psPSA 4–10 ng/mL, and 77.8% and 16.8% (p < 0.0001) for psPSA >10 ng/mL, respectively.
Conclusion:
The best objective indicator of biochemical success following whole-gland salvage cryoablation of the prostate is PSA nadir <0.4 ng/mL.
Introduction
U
In the last decade, prostate cryotherapy has emerged as a reasonable salvage option for recurrent localized prostate cancer. 3 –8 Salvage cryotherapy is minimally invasive and is an attractive option for patients with BR and who either wish to avoid or are not candidates for RP.
However, while multiple models based on prostate-specific antigen (PSA) nadir and other kinetics have been extensively validated for prediction of long-term success after both salvage external beam radiotherapy and brachytherapy for recurrent prostate cancer, 9,10 models for modern salvage prostate cryoablation remain hampered by modest follow-up even in large cohorts. We previously reported on the prognostic value of the first PSA level <0.6 ng/mL following salvage cryoablation of the prostate for recurrent prostate cancer. 11 However, follow-up was limited to 36 months, and longitudinal PSA testing was not analyzed. Subsequently, we demonstrated that a first postcryo PSA of <0.4 ng/mL predicts improved BR rates in a primary cryotherapy setting for localized prostate cancer. 12 The discrepancy between ideal initial PSA values following primary and salvage prostate cryoablation has not yet been explained. In this article, with a larger cohort and longer follow-up, we sought to identify the best PSA nadir cut point to predict future BR in a salvage prostate cryotherapy cohort.
Patients and Methods
The Cryo On-Line Database (COLD) was used to identify patients who were referred for salvage, full-gland cryotherapy of the prostate following primary radiotherapy of localized prostate cancer. The Institutional Review Board approval was granted for the purposes of the analysis. The majority of patients (94%) had biopsy-proven prostate cancer recurrence before undergoing salvage cryotherapy, with the remainder (6%) having missing data from the registry (Table 1). Patients with salvage partial-gland or primary whole-gland cryotherapy were excluded, as well as those with incomplete follow-up. Patient serum testosterone (T) levels were not captured in COLD, and thus, patients with prior ADT were excluded from the final analysis as return to precastrate T levels could not be determined, even in patients with an adequate washout period. All patients received a metastatic evaluation in the form of, at minimum, a bone scan and chest X-ray. Patients with evidence of locally advanced or metastatic disease at the time of salvage cryotherapy were excluded from the analysis.
PSA = prostate-specific antigen; SD = standard deviation.
We collected and analyzed baseline patient characteristics, including patient age, race, initial PSA, pre-RT Gleason score, total prostate volume, clinical T stage, PSA at diagnosis of recurrence, and postsalvage cryotherapy PSA values. The main endpoint measured was postsalvage cryotherapy BR, defined using the Phoenix criteria (PSA nadir +2) and in line with previous reports from the COLD registry. 11 –13
Statistical analysis
The Kaplan–Meier (KM) method was used to calculate the 5-year biochemical progression-free survival (bPFS) after salvage cryotherapy. The log-rank test was used to calculate differences among KM estimates at 5-year follow-up between patients who reached various PSA nadir values and between subgroups of patients with various presalvage prostate-specific antigen (psPSA) values (<4, 4–10, and >10 ng/mL). The statistical method for identifying PSA cut point with the greatest difference in bPFS has been previously described. 12 Briefly, to identify the postsalvage PSA nadir cut point that best predicts bPFS, we analyzed increasing PSA nadir thresholds, beginning at 0.1 ng/mL and repeated at increments of 0.1 ng/mL until 10 ng/mL. At each threshold, a Kaplan–Meier curve was calculated, and BR was analyzed for those with PSA nadir above and below the threshold, and p-values were calculated for the difference. The best cut point was identified when the rates of patients at risk of BR above and below the incremental threshold was largest. All statistical calculations were performed using R-3.0.1.
Results
We identified 998 patients who were referred for salvage cryoablation of the prostate from the COLD registry. Of these, 512 were excluded (105 patients received partial-gland salvage cryotherapy, 325 patients received prior ADT, and 82 patients had incomplete or missing follow-up PSA information) (Fig. 1). In total, 486 patients were identified for the final analysis. Median patient age was 72 years. Mean and median psPSA was 6.09 and 4.7, respectively. The remaining baseline characteristics of our patient cohort are represented in Table 1. Median follow-up was 18.2 months (interquartile range: 6.4–45.2 months).

Breakdown of excluded patients for final analysis. ADT = androgen deprivation therapy.
After systematically analyzing all possible thresholds for the greatest discrimination between bPFS time, we have identified the best PSA nadir cut point to be 0.4 ng/mL. Comparing the discrimination between, for example, using cut points 0.4 and 1.0 ng/mL, 0.4 ng/mL had a sensitivity and specificity of 0.47 and 0.78, respectively, while a cut point 1.0 ng/mL had a sensitivity and specificity of 0.31 and 0.85, respectively. Therefore, using a cut point 0.4 ng/mL correctly identified those who experienced BR better than using a cut point 1.0 ng/mL. The calculated concordance statistics using cut points 0.4 and 1.0 ng/mL were 0.72 and 0.66, respectively (p-value <0.0001).
Figure 2 represents the KM estimated 5-year bPFS for patients who achieved a PSA nadir less than or greater than 0.4 ng/mL following salvage prostate cryotherapy. For patients who achieved a PSA nadir <0.4 ng/mL, 2- and 5-year estimated bPFS rates were 91.7% and 75.5%, respectively. Patients who achieved a PSA nadir ≥0.4 ng/mL had 2- and 5-year estimated bPFS rates of 50.8% and 22.1%, respectively. Our statistical analysis failed to identify a better or more reliable PSA nadir endpoint than 0.4 ng/mL.
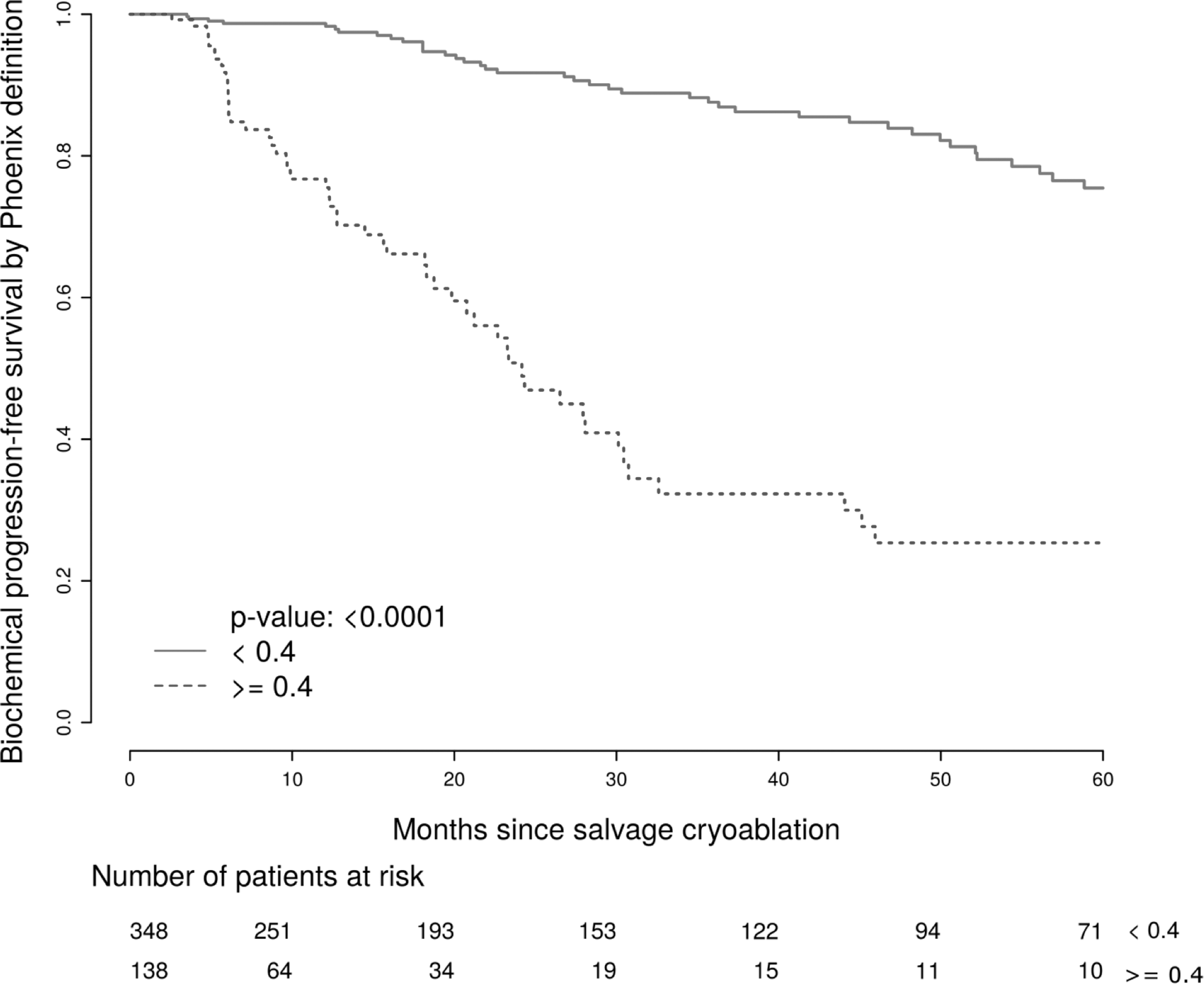
Kaplan–Meier estimated 5-year biochemical progression-free survival comparing PSA nadir <0.4 and ≥0.4 ng/mL. PSA = prostate-specific antigen.
Figures 3 –5 represent KM estimated bPFS curves for patients with psPSA values <4, 4–10, and >10 ng/mL, respectively, based on a PSA nadir cut point 0.4 ng/mL. We found significantly improved 5-year bPFS rates among patients who achieved a nadir PSA <0.4 ng/mL, regardless of psPSA level, and the results of this analysis are summarized in Table 2.
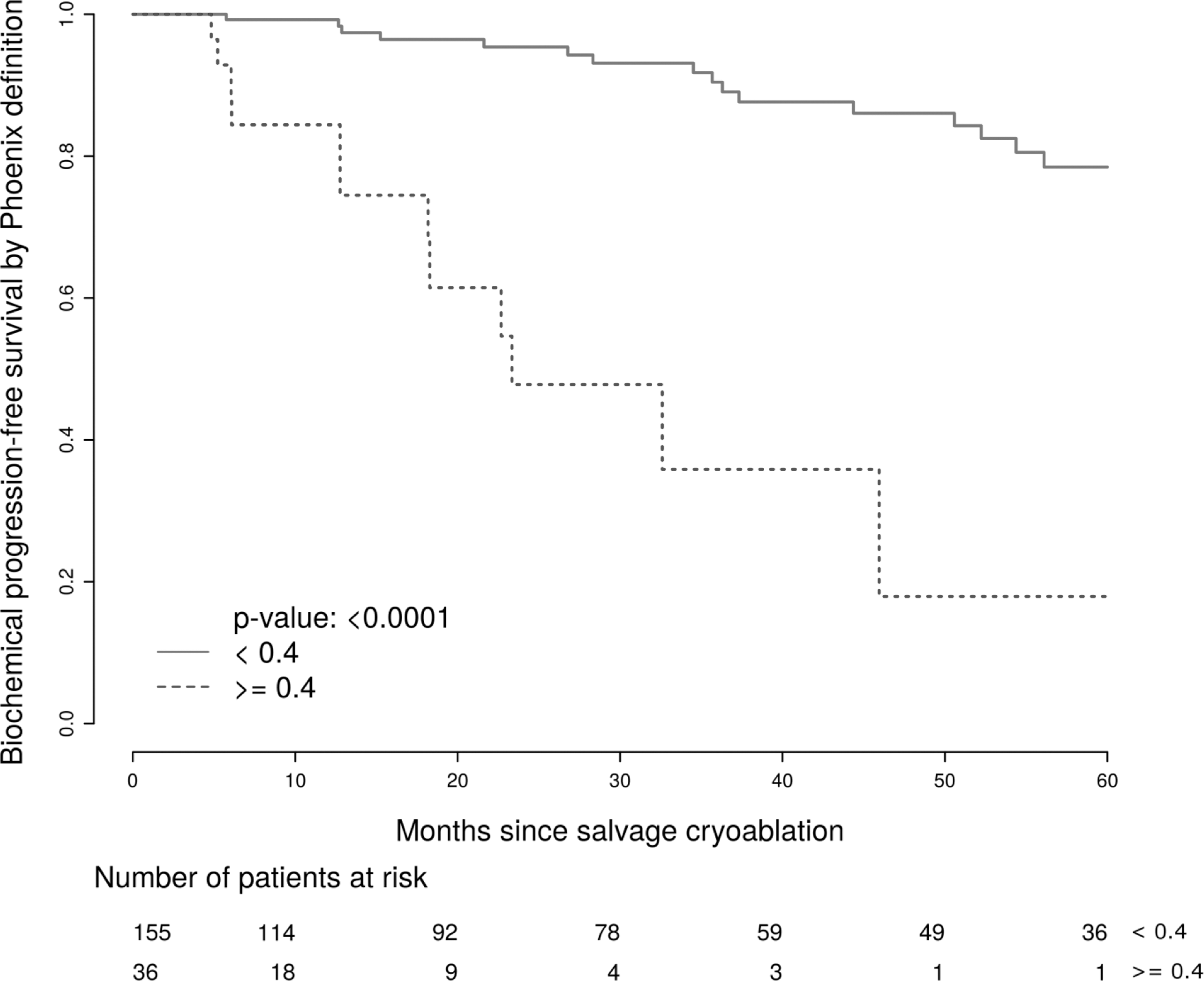
Kaplan–Meier plot stratified by PSA nadir 0.4 ng/mL for patients with a psPSA <4 ng/mL. psPSA = presalvage prostate-specific antigen.
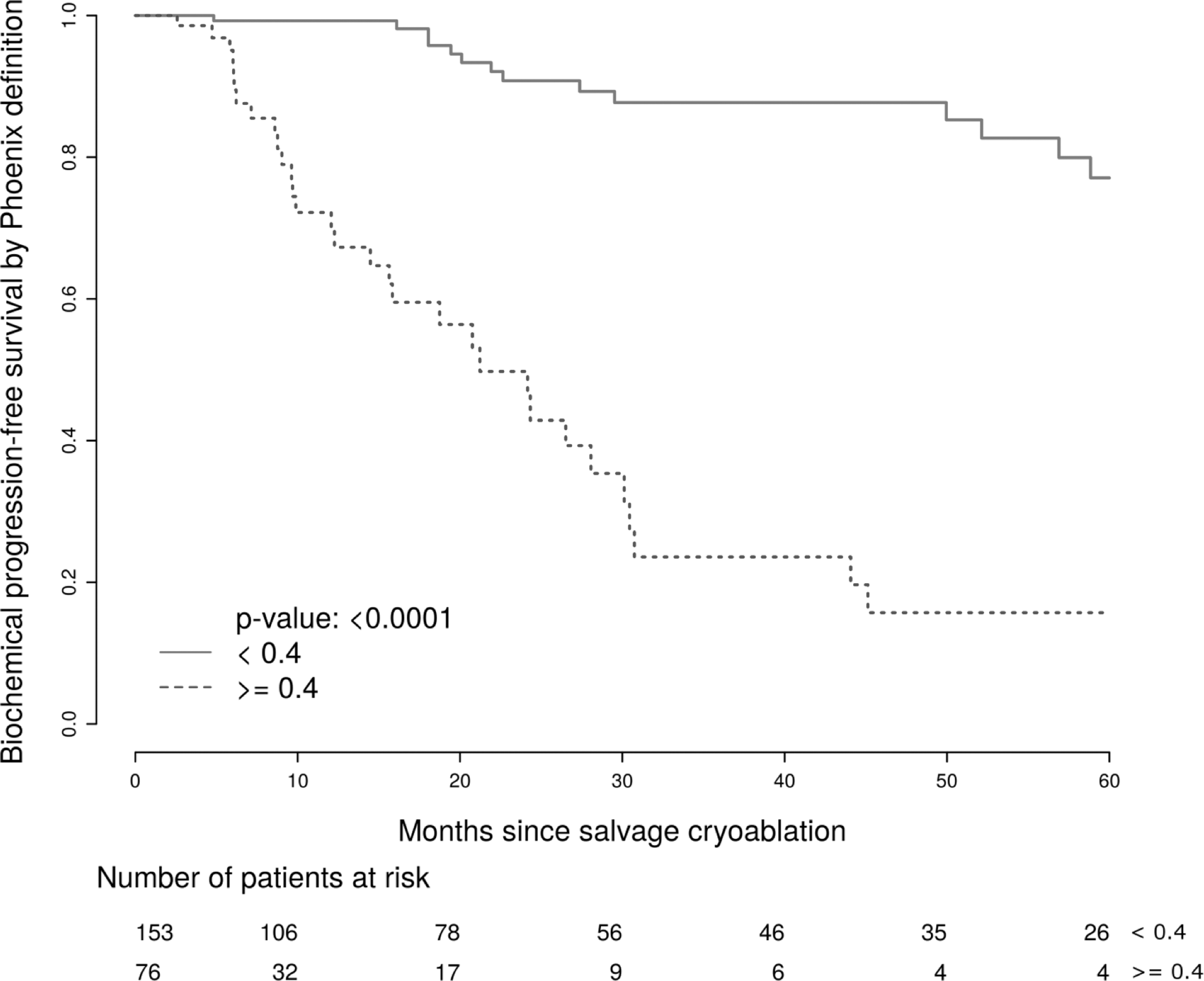
Kaplan–Meier plot stratified by PSA nadir 0.4 ng/mL for patients with a psPSA 4–10 ng/mL.
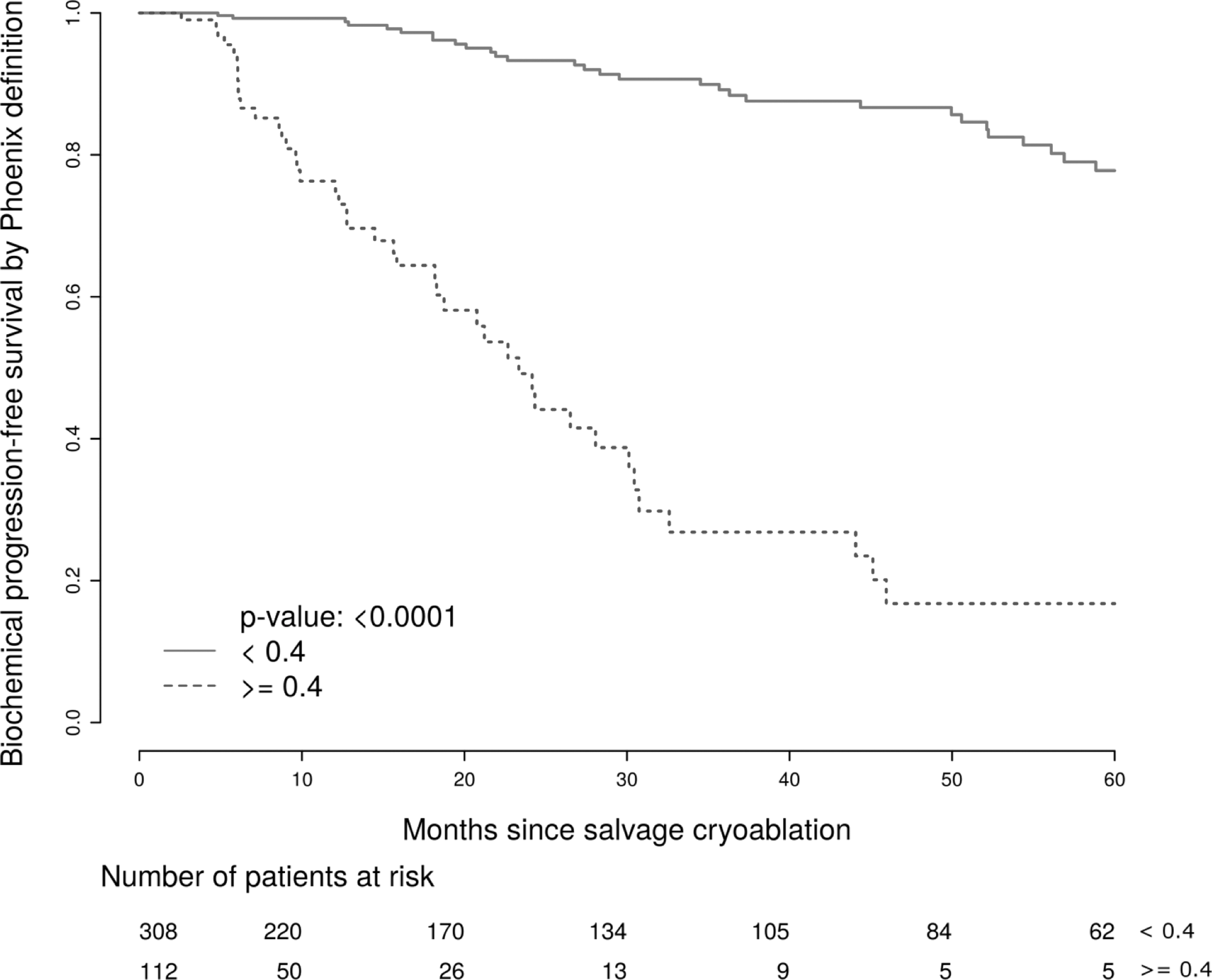
Kaplan–Meier plot stratified by PSA nadir 0.4 ng/mL for patients with a psPSA >10 ng/mL.
psPSA = presalvage prostate-specific antigen.
Discussion
Whole-gland cryotherapy of the prostate represents another potentially curative weapon in the urologist's armament for patients with biochemically recurrent localized prostate cancer following nonsurgical primary therapies, such as external beam radiotherapy, brachytherapy, high-intensity focused ultrasound, and primary partial- or whole-gland cryotherapy.
In this study, we demonstrate that patients who undergo salvage cryotherapy can expect long-term bPFS if their postsalvage PSA nadir is <0.4 ng/mL. In addition, the significant improvement in bPFS was seen across all psPSA subgroups. To standardize the outcome analysis, we used the Phoenix definition to define BR. While originally validated to define BR in a postradiotherapy population, Pitman et al. demonstrated that nadir plus 2 ng/mL outperformed all other definitions of BR in a postcryoablation cohort with biopsy-proven prostate cancer recurrence. 14
Our analyses stem from data collected through the COLD registry. While COLD data collection and reporting is voluntary, is variable from institution to institution, and represents heterogeneous operative techniques among reporting clinicians, it nevertheless represents an invaluable, multi-institutional resource that has gathered pre- and posttreatment information on more than 6000 patients who have undergone partial- and whole-gland primary and salvage cryotherapy of the prostate.
An important consideration for patients with biochemically recurrent prostate cancer following primary radiotherapy remains whether to undergo local salvage treatment versus systemic ADT. For patients with life expectancies >10 years and without radiographic evidence of metastases, long-term cure rates are often attained with salvage RP. 1 We believe that salvage prostate cryoablation represents a viable alternative to salvage RP, and previous studies have reported similar disease-specific survival rates following salvage RP and salvage cryotherapy. 15 The results of our analysis suggest that salvage cryoablation may be beneficial to patients with a wide range of psPSA values and who reach a postsalvage PSA nadir <0.4 ng/mL.
Indeed, previous work on salvage cryotherapy has mainly focused on pretreatment predictors of success. Using the COLD registry, Spiess et al. constructed a predictive nomogram for biochemical failure in patients undergoing salvage cryotherapy based on several diagnostic variables, including serum PSA level at diagnosis, biopsy Gleason grade, and initial clinical T stage. 16 Later, Spiess et al. developed a risk stratification model for biochemical failure based on both pre- and postsalvage patient characteristics. That retrospective analysis, which comprised 132 patients, found that a PSA nadir >2.5 ng/mL significantly predicted postsalvage biochemical failure. 17 Our cohort comprised 486 patients and represents the largest cohort to date for the purposes of analyzing postsalvage cryotherapy bPFS. Thus, using predictive nomograms of success after salvage cryoablation will aid clinicians in selecting patients who are most likely to attain a postsalvage PSA nadir <0.4 ng/mL.
We previously examined the prognostic importance of the initial posttreatment PSA value in a salvage cryotherapy setting for biochemically recurrent prostate cancer and showed that an initial postsalvage cryoablation PSA <0.6 ng/mL was also associated with improved bPFS rates at 36-month follow-up. 11 Later, however, we reported on prognostic implications of PSA nadir following primary, whole-gland prostate cryoablation and found a PSA nadir <0.4 ng/mL to be both attainable (891 of 1111 [80%] patients) and predictive of excellent bPFS rates. 12 In the current study, we endeavored to expand on this finding by examining multiple PSA follow-up values over a longer time in a larger cohort following salvage prostate cryoablation and, again, found no better PSA nadir cut point than 0.4 ng/mL at a follow-up of 60 months. Thus, the results of the current study strengthen our previous findings in a primary cryoablation setting and reiterate the importance of reaching a postsalvage PSA nadir <0.4 ng/mL by demonstrating substantially improved bPFS rates at 5-year follow-up.
In a subanalysis, we stratified patients by psPSA and found significantly better bPFS rates for patients who reached a postsalvage PSA nadir <0.4 ng/mL, regardless of psPSA. Patients with psPSA values <4, 4–10, and >10 ng/mL can expect 5-year bPFS rates of 78.5%, 77.1%, and 77.8%, respectively. The COLD registry-derived analyses of salvage cryotherapy outcomes based on psPSA are not without precedent. A previous report on outcomes after salvage prostate cryoablation stratified patients based on psPSA values less than and greater than 5.0 ng/mL. 18
Historically, the preferred salvage treatment for men with an intact prostate gland has been RP, and reports on salvage RP have demonstrated improved bPFS rates with psPSA levels below 10 ng/mL. 1,19 –23 In many of these series, the psPSA level was the only significant pretreatment predictor of postsalvage disease progression. We believe that investigators of salvage RP have stratified biochemical outcomes by psPSA levels above or below 10 ng/mL due to the historical value at which PSA was regarded as abnormal. Even though such stratification is artificial, PSA values at or below this range, combined with other classifiers, such as Gleason score at recurrence, ostensibly represent recurrent, organ-confined disease. In this sense, psPSA can be used as a surrogate for organ-confined disease. We sought to present a similar stratification model, based on three different psPSA subgroups (<4.0, 4–10, and >10 ng/mL), and found significantly better bPFS for patients reaching a PSA nadir <0.4 ng/mL across all psPSA subgroups.
As a salvage option, whole-gland cryotherapy is a relatively novel technology. Radiation, by comparison, is a much more established method of salvage for men who experience biochemical failure after primary surgical treatment of prostate cancer. For focal treatments to be widely accepted as a method of prostate cancer salvage, they must show comparable results compared with well-established salvage modalities. In a cohort of 448 men who received salvage radiation therapy without androgen deprivation for BR following RP, Jackson et al. demonstrated significantly improved distant metastases rates, cancer-specific survival, and overall survival with an undetectable postsalvage PSA nadir, whereas our cut point for significantly improved bPFS was 0.4 ng/mL. 24
Botticella et al. showed that PSA nadir was the only independent predictor of biochemical and clinical outcomes in a cohort of patients who underwent monotherapy salvage prostate radiotherapy for postprostatectomy BR. 25
Our results are consistent with salvage radiotherapy literature with regard to the importance of PSA nadir as a strong predictor of bPFS. In one of the largest meta-analyses of salvage prostate radiotherapy, 5-year bPFS rates ranged from 20% to 70%. 26 Based on our results, whole-gland salvage cryotherapy achieves equal, if not better, bPFS rates. However, BR is only one aspect of progression. This study establishes the starting point by defining short-term success with a nadir PSA cut point 0.4 ng/mL, but further studies are required to confirm whether this translates to improved metastasis-free, disease-specific, and overall survival rates.
We believe it is important for clinicians to be able to offer patients an accurate estimation of future BR risk based on posttreatment PSA trends. In prostate cancer, an undetectable PSA post-RP is the best indicator of cure. Meanwhile, with radiation therapies (external beam, brachytherapy, etc.), an inverse relationship exists between PSA nadir and the chance of long-term cure, with no defined absolute cut point. We sought to identify a meaningful PSA nadir level postsalvage, whole-gland cryotherapy of the prostate at which the patient can expect a reasonable long-term BR-free state. To our knowledge, this is the largest study to identify an ideal target PSA nadir postsalvage cryotherapy, and that PSA value is 0.4 ng/mL, and translates to an overall, 5-year bPFS of 75.5%.
Our study carries several limitations. First, the retrospective nature of our analysis lends itself to inherent biases. Second, postsalvage cryotherapy biopsy would be a more definitive proof of treatment success; however, this information is not reported in COLD. In addition, metastases rates, disease-specific survival rates, and overall survival rates were not included in the analysis. We believe that these endpoints are more meaningful and impactful to the patient and should be the focus of future studies. Statistically speaking, we performed a univariate analysis using the KM method to predict bPFS based on a PSA cut point 0.4 ng/mL but refrained from performing a multivariate Cox model based on additional factors, such as psPSA, presalvage Gleason score, prostate volume, age, race, and initial clinical T-stage. We believe that it is difficult to compare postsalvage PSA nadir with presalvage factors head-to-head as they are taken at two different time points. Therefore, adding postsalvage cryotherapy PSA nadir into a predictive model using the same follow-up time as psPSA would bias the results to the longer surviving patients. Furthermore, we limited the number of patients in our cohort by excluding 254 non-ADT-naive patients. In a recent study of patients with BR after pelvic radiation on intermittent ADT, full T recovery during nontreatment cycles occurred in only 35% of patients. 27 Since patient serum T levels are not recorded in COLD, T recovery could not be proven, even if a proportion of these patients experienced a significant washout period from ADT. Median follow-up following salvage cryotherapy was limited, at 18.2 months. Thus, the KM estimated bPFS data should be interpreted with caution. Finally, we did not stratify patients based on initial radiation dose. Due to improved biochemical failure rates with dose escalation regimens, 28 patients with BR after high-dose external beam radiotherapy might harbor more biologically aggressive disease than those who biochemically failed after conventional dose radiotherapy. Concordantly, bPFS rates for patients who achieve a PSA nadir <0.4 ng/mL may differ between these two relapsing groups. Nevertheless, the ability to reassure patients who reach a postsalvage cryotherapy nadir <0.4 ng/mL that their chances of remaining biochemically free of disease at 5 years range between 65% and 75% is meaningful to both urologist and patient.
Conclusion
Our analysis of the COLD registry patients who underwent whole-gland salvage cryotherapy of the prostate following primary radiotherapy for adenocarcinoma of the prostate demonstrates that patients who reach a postsalvage PSA nadir <0.4 ng/mL have significantly improved bPFS rates compared with those who reach a PSA nadir >0.4 ng/mL. Additionally, using a PSA nadir cut point 0.4 ng/mL significantly improved bPFS rates that were seen across all psPSA groups.
Footnotes
Author Disclosure Statement
Dr. J.S.J. is a consultant for Healthtronics. Dr. T.J.P. is a consultant and educator and has investment interests in Endocare. All other authors have no relevant conflicts of interest.