
Abstract
Introduction:
The improvements in flexible ureteroscopes provide efficient access to the upper urinary tract and advancements in laser technology strengthens the endourologists' armamentarium. The endourologists must be aware of the advantages and the potential complications of these powerful technological equipments. Our aim is to demonstrate temperature evolution during laser use inside an artificial kidney model.
Materials and Methods:
We created a bench model using K-Box® immersed into a saline-filled heating tank, which was used to obtain the needed temperature inside the cavity to provide different real-time situations. An endotracheal thermometer was placed inside. We used Olympus URF-P6 ureteroscope and Rocamed Holmium:yttrium-aluminium-garnet laser with two different fibers; 200 and 272 μm, at five different settings. Irrigation at room (24.5°C) and body (36.5°C) temperatures was used. We measured temperatures at 15th, 30th, and 45th seconds and 1st, 2nd, and 5th minutes of laser use with and without irrigation. We stopped measurements when temperature reached the upper limit of the endotracheal thermometer.
Results:
When irrigation was closed, with 272-μm laser fiber, we reached the temperature limit more rapidly with saline tank at 36.5°C than the tank at 24.5°C. When irrigation was closed, with both fibers and regardless of tank temperature and laser settings, the system surpassed the maximum temperature limit. With 272-μm laser fiber, the limit was reached as early as the 30th second. When the irrigation was open, we did not reach the maximum temperature limit regardless of tank temperature and laser setting. When two laser fibers were compared, the temperature increase was more pronounced with 272-μm fiber, but the difference was not statistically significant.
Conclusion:
Laser use during flexible ureteroscopy may cause increased intrarenal temperatures. Rapid increases should be kept in mind when irrigation is closed. The irrigation seems to limit the temperature increase when used with any laser setting.
Introduction
S
Holmium:YAG lasers use thermomechanical action and cause immediate temperature increase, which can affect kidney tissue in various manners. 4 The temperatures reached during Holmium:YAG laser usage are not commonly adressed in literature. In this study, we evaluated the temperature changes in an experimental model simulating the renal cavities using different laser settings and states of irrigation.
Materials and Methods
This study was conducted in a laboratory setting with objective evaluation. The model used to reproduce the renal cavities was the Kidney-Box (K-Box®; Porgès-Coloplast), which is a new F-URS training kit from Coloplast, made of polyurethane. We chose a 10 mL K-Box cavity to perform the measurements. We used Olympus URF-P6 flexible ureteroscope, Rocamed 20 W Holmium:YAG laser, and two different laser fiber diameters: 200 and 272 μm. Smith Medical endotracheal thermometer (ER400-9 9FR) was connected to Philips Intellivue anesthesiology monitor to measure intracavitary temperatures.
For irrigation, we used TraxerFlow irrigation line from Rocamed, connected to either Rocamed Endoflow pump at 50 cm H2O pressure to obtain a constant irrigational temperature of 36.5°C or to a suspended saline bag at 50 cm for gravitational irrigation to obtain a temperature of 24.5°C. The room temperature in our laboratory was constantly at 24.5°C, so the irrigation bag temperatures were always the same and not affected by any external influence. The velocity of the irrigation is another variable that can influence the temperatures. With an endoflow pump, the pressures and the velocity are easier to keep at a steady level and with a suspended irrigation bag there may be slight changes when the bag empties. To avoid even the slightest changes, we performed every measurement with an unused, full irrigation bag. With this setting, the irrigational pressures are constant at 50 cm H2O, so there is no difference of velocity between the suspended bag and the irrigational pump. To reach the desired temperature inside the artificial renal cavity, we immersed the K-Box into a saline-filled Jouan (J30 bain universel 41093016) heating tank. The endotracheal thermometer was fixed inside and we used the ureteroscope for placing the laser fiber at the center of the cavity. The distance of the endotracheal thermometer to the fiber tip was 10 mm. The study setting is shown in Figure 1. We used five different laser settings. For dusting, we used 0.5 J at 20 Hz and 1 J at 10 Hz, whereas the fragmentation settings were 2, 3, and 4 J at 5 Hz each. Before each measurement, we cut the tip of the laser fiber for 1 cm to avoid bias due to measurements with fibers at different conditions. For each setting, we performed the measurements when the irrigation was open and closed seperately. We also created two real-time situations concerning the temperature of the irrigation; saline at room temperature and saline preheated to body temperature. In the first setting, we heated the saline inside the K-Box to 24.5°C as this temperature was considered the temperature that we have while using a room-air temperature irrigation fluid, and in the second, to mimic the use of body temperature irrigation we heated the saline inside the K-Box to 36.5°C before the begining of experiments.
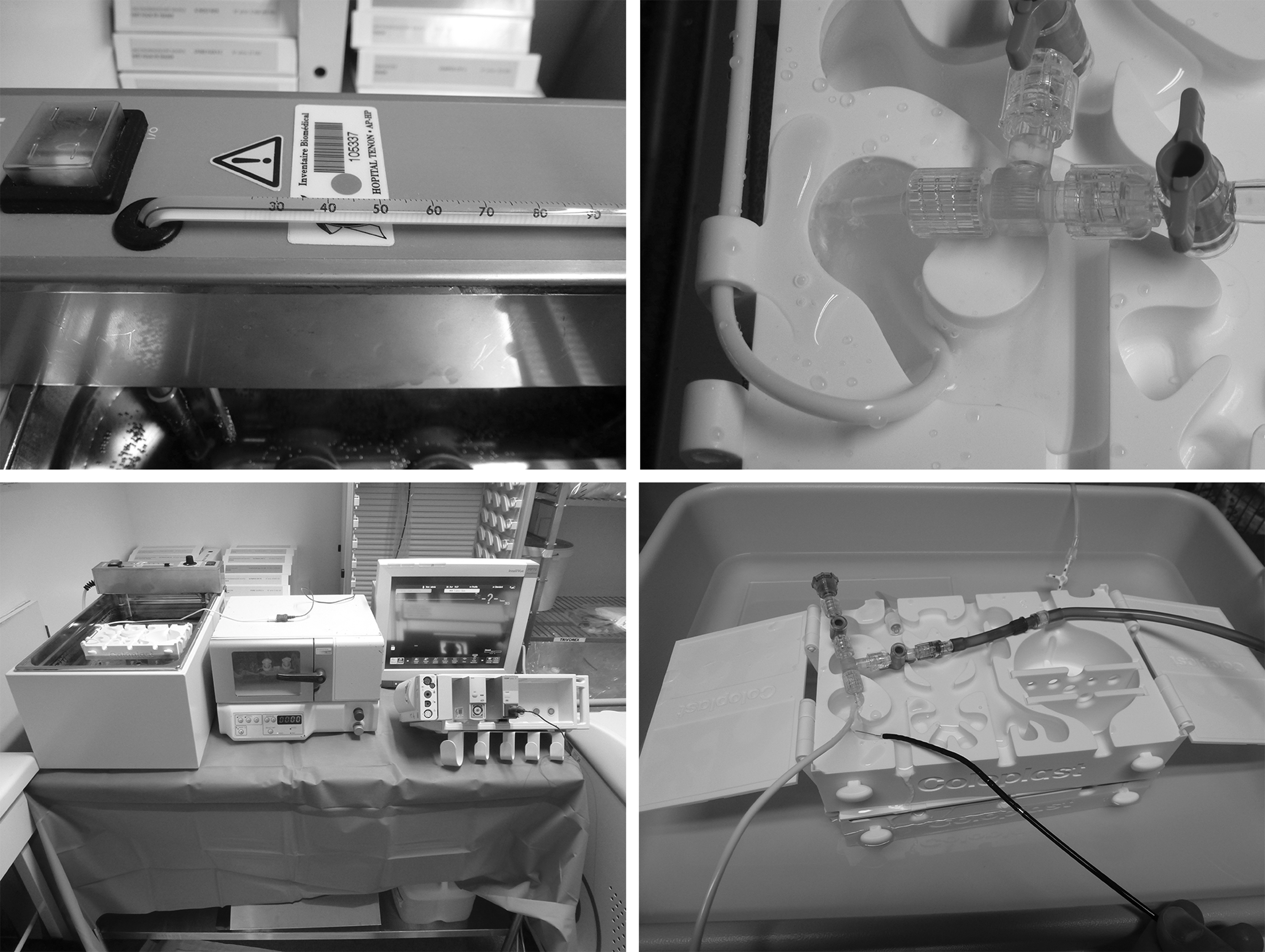
The study setting and the bench model. (upper left: the thermometer on the heating tank showing the temperature inside which the K-Box® is situated; upper right: the K-Box cavity inside which the irrigation is perfomed and the endotracheal thermometer is situated; lower left: the study setting seen as a whole; lower right: the K-Box during the laser activation and the measurement by the endotracheal thermometer).
We started the laser and measured temperatures at 15th, 30th, and 45th seconds and 1st, 2nd, and 5th minutes. We stopped the measurements when the temperature reached 45°C, which was the upper limit for the endotracheal thermometer. We limited the experiment to 5 minutes because within this time period, we were able to reach a desired conclusion. Also, during this time period, the temperatures reached the upper limit of our endotracheal thermometer. We recorded all the data and the statistical analyses were performed.
The data are presented as mean values and analyzed with IBM SPSS Statistics Vesion 22. Mann–Whitney U test was used to compare the values and provide statistical information between each combination.
Results
When the saline tank was at 24.5°C, the intracavitary temperatures with 200- and 272-μm fibers were similar when used at different laser settings at the 15th second with both closed and open irrigation. When the irrigation was closed, at every laser setting, the temperatures gradually increased and exceeded the upper limit of the endotracheal thermometer at the fifth minute. In this situation, when the two laser fiber diameters were compared, there was no significant difference in terms of temperature and also time elapsed to exceed 45°C. The time elapsed to exceed the upper limit decreased when laser energy was increased as 0.5 J at 20 Hz being the longest for both fibers, 2 J at 5 Hz being the shortest for 200-μm fiber, and 4 J at 5 Hz being the shortest for 272-μm fiber.
However, when the irrigation was open, with different laser settings, the temperatures did not exceed 45°C with the maximum temperature being 26.2°C and 25.5°C for 200- and 272-μm fibers, respectively. Also, the temperatures at different time periods were not statistically different from one another.
In the 24.5°C saline tank, with both 200- and 272-μm fibers, the temperatures were significantly higher at all different time periods when the irrigation was closed regardless of the laser settings when compared with open irrigation (p < 0.05).
When the saline tank was at 36.5°C to mimic the real-time kidney during an F-URS and irrigation was closed, the intrarenal temperatures gradually increased and for 200-μm laser fiber, they exceeded the upper limit of 45°C at the 1st minute with 3 and 4 J at 5 Hz laser settings and for the 272-μm laser fiber, they exceeded the upper limit at the 30th second with 2 J at 5 Hz energy setting. While there was a difference in time elapsed to exceed the limit, this difference was not statistically significant.
At the same situation, when the irrigation at 36.5°C was opened, the intrarenal temperatures did not increase throughout the experiment with the highest being 38°C for the 200-μm laser fiber at 4 J at 5 Hz and 38.5°C for the 272-μm laser fiber at 2 J at 5 Hz. Similar to the situation where the saline tank was at 24.5°C, the temperatures at different time periods are not statistically significant from one another.
In the 36.5°C saline tank, with the 200-μm laser fiber, regardless of the laser setting used, the temperatures were significantly higher at the 45th second and at the 1st and 5th minutes when irrigation was closed, when compared with the open irrigation situation. At the 15th and 30th seconds, the differences in temperatures were not statistically significant between open and closed irrigation situations. With 272-μm fiber, the temperature difference was statistically significant between open and closed irrigation situations with every laser setting (Table 1).
p < 0.05: comparison between open and closed irrigation.
Tmin = time in seconds after which the known temperature of 45°C was reached and the experiment stopped.
Discussion
There has been more than 50 years since the construction of the first working laser emitter and ∼40 years since the world's first endourologic surgery with laser. 5,6 Since then, laser technology has improved to a great extent and lasers are currently used for great variety of endourologic surgeries. 7
The holmium laser uses YAG as crystalline matrix. Chromium, thulium, and holmium are mixed with YAG melt to prevent overheating inside the crystal. However, the laser crystals deposit heat and subsequently restrict the holmium laser to pulsed operation at room temperatures with limited repetition rates. The holmium laser radiation is strongly absorbed by the water molecule and has short extinction length in tissue. This phenomenon results in a depth of penetration around 400 μm. 8,9 Besides, the high density of power absorbed in irrigation solution and tissue results in an abrupt overheating above the boiling point. 10,11
During pulsed usage of holmium:YAG laser, a steam bubble with a diameter of a few millimeters wide is generated next to the fiber tip. The steam bubble persists the same amount of time as the laser pulse, which is about 500 μs, meaning that it vanishes in such short time that it is invisible to human perception. 8,9
The expanding and recollapsing cavitation bubble generates heated propagation waves and has an erosion effect on nearby environment. Due to this instant thermal increase, many of the normal cellular functions may be altered as a consequence of protein denaturation. An abnormal pattern of genetic expression in all levels of transcription, splicing, and translation; DNA synthesis and cell division inhibition; and cell adhesion abnormalities can be encountered and may subsequently lead to cell death due to loss of cellular functions and disturbed integrity of cellular composition. 12
Understanding the basic principles of functioning of holmium:YAG laser is essential to conduct research and improve clinical practice. Various aspects of F-URS and laser lithotripsy or tissue ablation have been studied such as maneuverability, visual aspects, irrigation flow rates, access sheath insertion force, intrarenal pressures etc.
13
–21
A small pilot study evaluating the changes in urinary markers before and after extracorporeal shockwave lithotripsy and F-URS found out that the kidney injury markers, kidney injury molecule-1 and N-acetyl-β-
The low morbitidy profile of F-URS is demonstrated in several studies. 23 In fact, during F-URS the laser remains activated for most of the time, thus increasing temperatures. However, the temperature changes during active laser usage are not commonly addressed, which may also be hypothesized to affect normal kidney functions. 4
The major safety factor during laser usage is the accurate fiber contact with the target, provided the distance between tip of the fiber and kidney tissue >1 mm, since the depth of thermal injury is 0.5 to 1 mm. It is hypothesized that when applied in saline irrigation, there is minimal risk of surrounding tissue injury. 24 –26 However, it should be kept in mind that the surrounding environment temperature, which is the irrigant solution, may rise and elevated temperatures can result in previously mentioned cellular dysfunction indirectly related to laser use.
In this study, we demonstrated the temperature evolution inside a bench model with different laser settings and irrigation systems. Actually there are no studies in literature about F-URS performed without irrigation. While F-URS without irrigation can be practically impossible due to stone fragments blurring the vision, this situation is theoretically possible. In cases where a relatively larger sized laser fiber is inside the working channel of a flexible ureteroscope, the irrigation can be compromised to a great extent and flow rates can be low and may fail to provide the cooling effect of the surrounding environment. 27
When the irrigation is closed, activation of the laser fiber results in a more abrupt increase of temperature. Especially when warm saline at 36.5°C is used, the temperature inside the K-Box reaches rapidly 45°C, which is the upper limit of the endotracheal thermometer used and is considered to be a temperature that can influence the normal functioning of cells. Bettaieb and Averill-Bates demonstrated in their study that hyperthermia causes distruption of calcium homeostasis, activates calpain–calpastatin proteolysis, induces endoplasmic reticulum stress, and causes apoptosis. 28 Also, Vazquez and Larson showed that between 43°C and 45°C, protein degradation occurs. 29 So beyond 45°C, we assumed that the cellular functions are compromised and accepted this temperature as the upper limit for our measurements.
When irrigation is open, with saline at room and body temperature, there seems to be no significant changes in temperature. The system in both situations reaches a constant level in about 1 minute after laser activation, with a thermal increase of about 1°C that is not significant.
In endourological surgeries, it is generally advised to use warm irrigation because the use of irrigation at room temperature is believed to result in hypothermia, which is defined as a decrease in core body temperature below 36°C during or immediately following a surgery. 30 Even mild hypothermia, a 1°C to 3°C decrease in core temperature, has adverse effects like shivering, which in turn increases total body oxygen consumption and may cause hypoxemia especially in elderly with cardiovascular risk factors. Singh et al. demonstrated that the use of warm irrigation during transurethral resection of the prostate (TURP) decreased perioperative hypothermia and shivering. 30 Since the temperature of the irrigation solution, when irrigation is open, does not seem to be a contributor to the thermal increase in our model, we believe that the use of body temperature irrigation should be recommended to prevent hypothermia and related complications.
Nowadays different sizes of laser fibres are used, differing from 200 to 500 μm. Experience revealed that best results are obtained in F-URS with small-sized fibers, ranging from 200 to 272 μm, due to their flexibilities. 20,31 In our study, use of different sized fibers does not seem to have significant impact on temperature uprise inside the cavity when the irrigation system is open. With both fiber sizes, the temperature inside the model did not exceed 40°C and exhibited only a change of about 1°C after 5 minutes of laser activation. In contrast, when the irrigation is closed, 272-μm laser fiber caused a significantly rapid increase in temperature when compared with 200-μm fiber, with both fibers causing an increase in temperature above 45°C. With this information, we can suggest that thinner fibers may be considered safer in terms of intrarenal temperatures, when working without irrigation.
In this study, we aimed to establish a pattern for temperature behavior in the model cavity during the laser activation. It is highly probable that the in vivo temperatures are different, but in each case the dynamics should be similar. Temperature exchanges between the fiber, the irrigation system and the renal cavities should behave in the same manner. In laser lithotripsy, we should also take into account the energy absorbed by the stone, which can probably lead to a less increase of intracavitary fluid temperature. 9
This study is the second study that evaluates the temperature profile during laser activation. The first laser lithotripsy thermography was performed by Molina et al. using two ex vivo models of Ovis aries urinary tract and human calcium oxalate calculi. 32
Temperatures were measured on the external portion of the ureter and urothelium during lithotripsy and intentional perforation. They concluded that there is an increase in external ureteral temperature during laser activation, but temperatures decreased when saline flow was applied. While our study is conceptually different and investigates the temperature evolution in a cavity similar to the renal pelvis, same conclusion was obtained. In both studies, when the irrigation is closed, authors reported such temperatures that could create denaturation of the proteins or in some cases real burns of surrounding tissues. When the irrigation is open, both studies measured temperatures arguably not harmful to kidney cell functioning.
Another finding emphasized by our results is that the irrigation provides a steady temperature inside the model. When the irrigation is closed, temperatures gradually rise with both fibers at different laser settings. Inside the 36.5°C saline tank, while the difference in temperatures seems to be obvious at the 45th second and thereafter, when the irrigation is closed, this difference might not have an impact on clinical practice because laser time is generally more than 45 seconds and the fact that temperatures do not increase significantly before the 45th second loses importance. In addition, most of the endourologists prefer to use irrigation to provide a clearer vision, so this situation is not frequently encountered during daily practice.
Our study has limitations. First of all, while the dynamics are similar with real-time situation, this is an in-vitro study and the bench model lacks the physiological properties of a real kidney. The vascularity of the kidney itself and the changes in the rate of blood flow, the continuous production of urine, and the expandability due to elasticity of the kidney tissue compared to an inanimate model may all influence temperature changes. Secondly, during F-URS, continuous flow of irrigation from the endoscope into the kidney and through the ureter to outside may further decrease temperatures.
Also, inside the kidney, continuous backflow of irrigation solution into the venosinusoidal system may also affect temperatures. In addition, it is a general practice to use irrigation along with laser during F-URS, so our data about the temperatures with laser use without irrigation may be considered a limitation of the study due to being rather clinically insignificant, but it should be noted that it provides valuable information to support the use of irrigation and understand the dynamics of the temperature changes. The last point as a limitation is that our endotracheal thermometer has a maximum limit point, so we could not measure the temperatures that we reach above 45°C, which could have been an interesting and important finding.
Conclusion
Even though this is an in-vitro study, it clearly demonstrates the temperature evolution inside the bench model mimicking a real-time F-URS. The similarity of thermodynamic properties with in-vivo situations and the variety of different situations created for the experiment can supply valuable information.
Laser technology is a powerful tool with which we can succeed, but we should also be aware of potential harmful effects and provide a balance in between.
We can conclude that laser use, when irrigation is open, is safe in terms of temperatures. Because use of warm irrigation solution has benefits, we recommend its use during F-URS and laser activation. Further in-vivo studies are needed to support our findings.
Footnotes
Author Disclosure Statement
Professor Olivier Traxer is a consultant for Olympus, Rocamed, and Coloplast in research and development. For the remaining authors, no competing financial interests exist.