
Abstract
Objectives:
Open nephroureterectomy (ONU) is the current standard for muscle-invasive upper tract urothelial carcinoma (UTUC) in the European Association of Urology/Japanese Urological Association (JUA) guidelines. In this study, we compared the postsurgical survival of muscle-invasive UTUC patients treated with ONU or with laparoscopic nephroureterectomy (LNU), using the multi-institutional national database of the JUA.
Methods:
The 1509 patients with UTUC who were diagnosed at 348 Japanese institutions in 2005 were registered. We collected the clinical data of the patients in 2011. The muscle-invasive UTUC patients who underwent ONU or LNU were identified, and survival curves were estimated using the Kaplan–Meier method.
Results:
Overall, 749 pT2≥cNxM0 patients underwent a nephroureterectomy (ONU, n = 527 and LNU, n = 222). The overall survival and cause-specific survival rates were not significantly different between the ONU and LNU groups (p = 0.1263 and p = 0.0893, respectively). In addition, 459 of the 749 (61.3%) patients experienced disease recurrence (bladder recurrence, local recurrence, or distant metastasis), with no significant difference between the ONU and LNU groups. Even when patients were stratified by pT3/pT4 and/or pN+, overall survival was not significantly different between the ONU and LNU groups (p = 0.2876). The results of a univariate analysis showed that lymphovascular invasion was an independent prognostic factor for overall survival, but the surgical approaches were not found to be associated with overall survival.
Conclusions:
Our data suggest that there is no evidence that the oncologic outcome of LNU is inferior to that of ONU in muscle-invasive UTUC, when the appropriate patients are selected.
Introduction
U
LNU is probably as effective as ONU regarding overall survival of patients with low-grade tumors, but not for the high-risk patients with high-grade tumors and advanced localized disease who require a lymphadenectomy, or patients who have indications for adjuvant chemotherapy after surgery. The European Association of Urology (EAU) guidelines still recommend that invasive, large (T3/T4 and/or N+/M+) or multifocal tumors should be considered contraindications to LNU, despite the preference of patients for minimally invasive surgery. 4 To better understand the oncologic efficacy of LNU for muscle-invasive nonmetastatic UTUC, we analyzed additional data that compare oncologic outcomes after ONU and LNU procedures, using the nationwide database of the Japanese Urological Association (JUA).
Patients and Methods
We performed a retrospective cohort study using data from the JUA multi-institutional national database: the 1538 patients from 348 Japanese institutions who were diagnosed in 2005 were registered in the present study in 2011. Generally, secondary (after bladder cancer) UTUC patients are excluded from this registry, but the cases of 29 patients with secondary UTUC after bladder cancer were contaminated. Thus, the records of 1509 patients were analyzed in the present study, excluding these 29 patients. 5
We selected the pT2≤cNxM0 patients from among the 1509 patients, resulting in a series of 749 patients for the study. We reported the operative trend in UTUC in an earlier study. 5 Due to the multiple centers and the study's retrospective design, there was variation among the surgical techniques of transperitoneal or retroperitoneal approaches and removal of the distal ureteral end, including open or laparoscopic techniques for approach, intravesical irrigation to prevent bladder recurrence, the indications for lymphadenectomy, and the extent of lymph node dissection (LND), and standardization for the present analyses was not possible. The preoperative chemotherapy and radiotherapy were selected depending on each institution or each physician. Follow-up was performed according to each institution's protocol.
The second edition of the General Rule for Clinical and Pathological Studies on Renal Pelvic and Ureteral Tumors, 6 edited by the JUA and The Japanese Society of Pathology based on Union International Contre le Cancer (UICC) 2002, was referenced for clinical information. The overall survival and cause-specific survival were defined as the period between the date of diagnosis and the date of all-cause death and death from UTUC, respectively.
Statistical analyses
We estimated the overall and cause-specific survival rates using the Kaplan–Meier method. The chi-square test was used to evaluate the association between variables in comparisons of the two procedures (ONU vs LNU). The log-rank test was used for the comparison of survival between the patient groups. Potential prognostic factors were established by a univariate analysis. Information on age, sex, operative procedure, approach method, perioperative chemotherapy, tumor location, and lymphovascular invasion was included as variables. All reported p-values were two sided, and p-values <0.05 were considered significant. All statistical analyses were carried out using the JMP Pro version 10.0.0 (SAS Institute, Cary, NC).
Results
Clinicopathologic characteristics
Table 1 summarizes the patients' characteristics. Data were stratified according to the procedure type (ONU vs LNU). There was no significant difference in the distribution of age, clinical stage, tumor location, the route of approach, perioperative therapy, or LND between the two groups. Perioperative therapy was performed in almost 25% of the 527 ONU patients and 23% of the 222 LNU patients, with no significant difference between the groups. LND was carried out in approximately one-third of the ONU and LNU patients, respectively.
LNU = laparoscopic nephroureterectomy; ONU = open nephroureterectomy; UTUC = upper tract urothelial carcinoma.
The pathologic results are summarized in Table 2. The pathologic stage, tumor grade, and lymphovascular invasion were not significantly different between the ONU and LNU groups. The proportion of pN+ patients was slightly higher in the ONU group, but not significantly so.
Recurrence pattern
Overall, 459 of the 749 patients experienced disease recurrence of any type as follows: 323 (61.3%) in the ONU group and 136 (61.3%) in the LNU group. The most common type of disease recurrence was distant metastasis: 186 (35.3%) in the ONU group and 75 (33.8%) in the LNU group. During follow-up, 174 (33.0%) of the ONU patients and 69 (31.1%) of the LNU patients experienced bladder recurrence, and 64 (12.1%) ONU patients and 27 (12.2%) LNU patients experienced local recurrences. We were unable to obtain data about the port site or regarding wound site metastasis (Table 2).
Survival
The median follow-up was 39.0 months (range 0.1–79.3 months). The 3-year overall survival estimates and the 3-year cause-specific survival estimates were 69.5% and 73.0% for the patients treated with ONU vs 72.4% and 76.0% for the patients treated with LNU, respectively, with no significant differences (p = 0.1263 and p = 0.0893; Fig. 1).
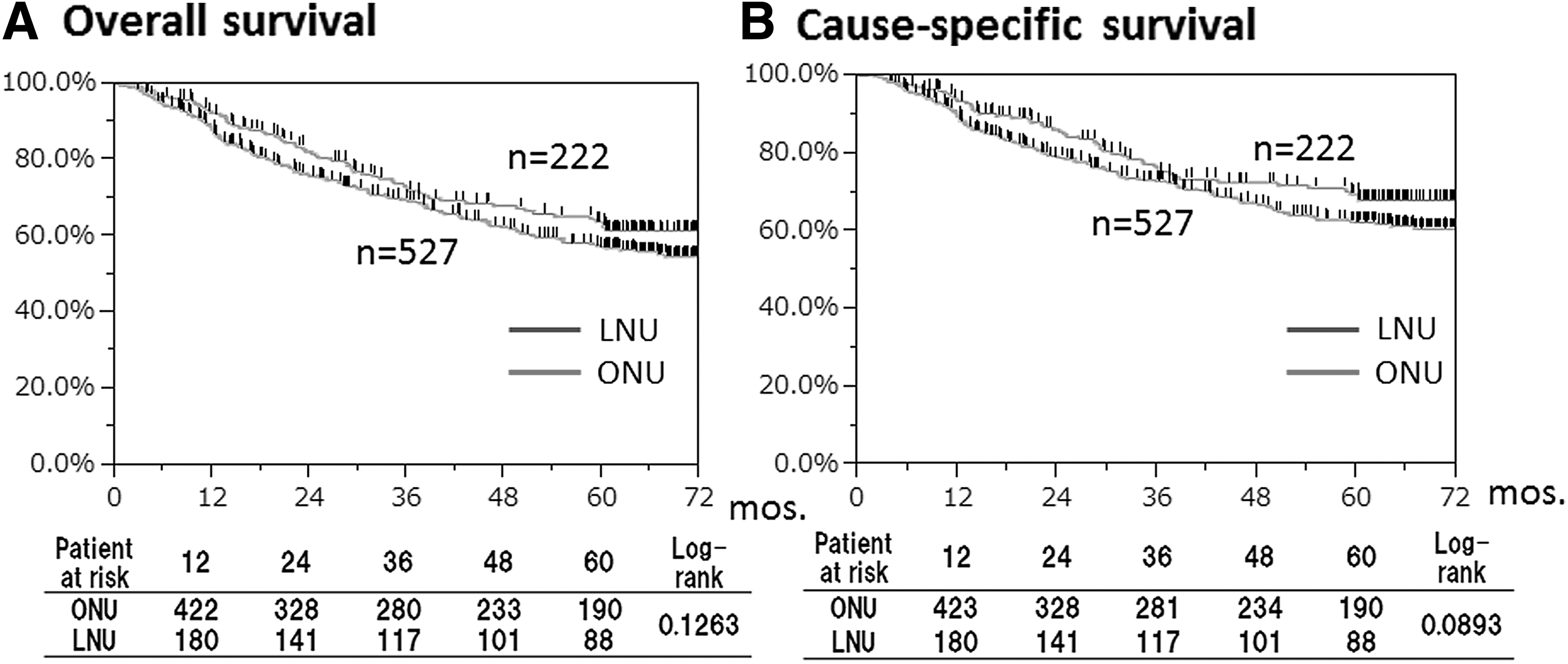
Kaplan–Meier estimates of overall survival and recurrence-free survival following nephroureterectomy, stratified by surgical approach. LNU, laparoscopic nephroureterectomy; ONU, open nephroureterectomy.
As shown in Figure 2, in the stratification by advanced disease (pT3/T4 and/or pN+), there was no significant difference between the ONU and LNU groups regarding overall survival (p = 0.2876).
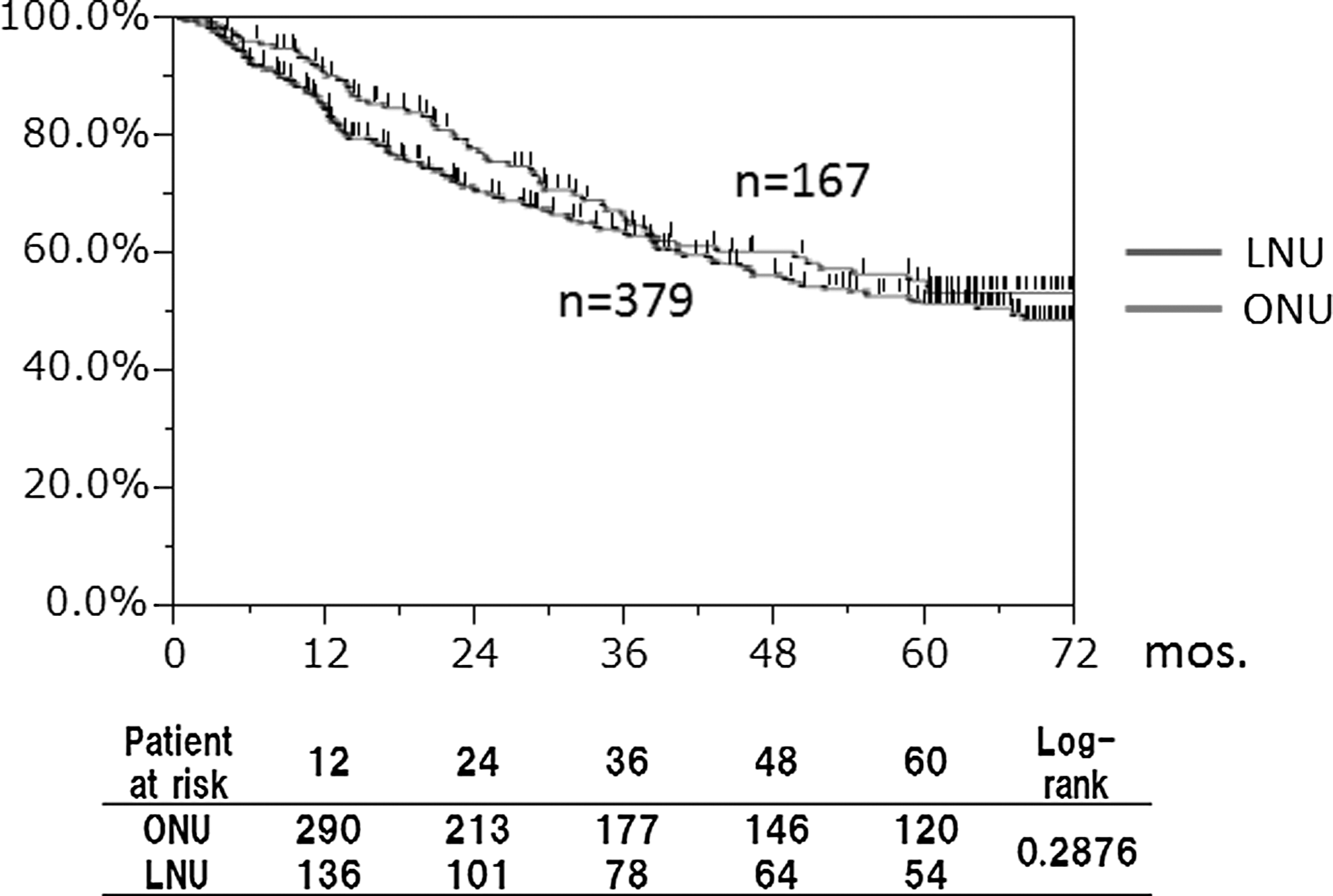
Kaplan–Meier estimates of overall survival following nephroureterectomy comparing ONU and LNU stratified by pT3/T4 and/or pN+.
The results of the univariate analysis are shown in Table 3. Lymphovascular invasion was revealed as an independent prognostic factor for overall survival, but the surgical approaches were not found to be associated with overall survival.
Discussion
During the 10-year period from 1995 to 2005, a total of 2431 patients underwent LNU (with or without a hand-assisted approach) and extracorporeal shockwave lithotripsy in Japan, according to a survey conducted by the Japanese Society of Endourology (JSEE), 7 and 51% of the patients in the survey who underwent LNU had invasive UTUC. LNU for invasive UTUC was thus widely performed in Japan at that time. In a randomized prospective study, however, when matched for pT3 and high-grade tumors, the cancer-specific survival (CSS) and metastasis-free survival rates were significantly different between the LNU and ONU groups, in favor of ONU. 8
In the EAU guidelines, invasive or large (T3/T4 and/or N+/M+) tumors are contraindications for LNU. 4 There are thus negative opinions about LNU in the guidelines, but the evidence on the oncologic outcomes of LNU among high-stage UTUCs is scarce. 9 In the present study, we report the oncologic outcomes of LNU for muscle-invasive UTUC among patients in the JUA database. Our results demonstrated that the overall survival and cause-specific survival were not significantly different between the patients who underwent ONU and those who underwent LNU. Even when the patients were stratified by pT3/pT4 and/or pN+, the overall survival was not significantly different between the two groups. Our data thus suggest that there is no evidence that the oncologic outcomes for LNU are inferior to those for ONU in muscle-invasive UTUC, if the appropriate patients are selected.
Metastasis of a UTUC to regional lymph nodes is a common occurrence and is also a significant predictor of oncologic outcomes. LND associated with nephroureterectomy is of therapeutic value and allows for the optimal staging of UTUC. 10,11 In a study of 109 patients, Kondo and colleagues suggested that the extent of lymphadenectomy improves survival in patients with advanced-stage UTUC. 12 Moreover, Brausi and colleagues demonstrated that LND improves disease-free survival and CSS in patients with muscle-invasive UTUC. 13 Burger and colleagues 14 also observed that positive lymph node status was independently associated with disease recurrence and cancer-specific mortality rate in the overall population of UTUC patients.
Taking these past findings into account, LND appears to be an important procedure in nephroureterectomy, and the template of LND is likely to have a greater impact on patient survival. 12,15 However, the anatomic sites of lymph nodes have not yet been clearly defined. Based on the pathologic findings regarding lymph node metastasis, it is appropriate for patients to select adjuvant chemotherapy. In the present study, we found that in 2005, the frequency of the use of LND in both the ONU and LNU groups was similarly low. In other words, it appears that there is no difference in the outcomes of ONU and LNU when LND is not performed in ONU.
LND can now be performed safely and effectively during LNU, 16 and it may be necessary to consider standard LND in cases of muscle-invasive UTUC. Further studies of routine LND in high-stage UTUC cases are required to improve the outcomes of both ONU and LNU.
In our study, it is difficult to clearly explain the unfavorable impact of LNU on the overall survival in the patients with invasive UTUC, because there were no significant differences in the characteristics of the patients who underwent ONU and those who underwent LNU, and the patients in both groups were treated under equivalent therapeutic strategies, including the number of patients with LND. In addition, the univariate analysis indicated that the surgical procedure was not an independent prognostic predictor, even in the patients with invasive UTUC. For overall survival, many articles have reported tumor stage and lymph node metastasis as prognostic factors. 17 Our group observed a 5-year earlier onset of UTUC among current smokers. 18 There is no clear explanation regarding why the results concerning the association between smoking and histologic grade have been inconsistent among UTUC studies. However, accumulating evidence suggests that a dose escalation and a longer duration of smoking might increase not only the risk of the development of urothelial carcinoma but also its aggressiveness. 19 –21
We would like to emphasize several limitations of this study. First, although this study may have examined the greatest number of invasive UTUC patients among the existing studies comparing ONU and LNU, the indications for the personal choice of laparoscopic technique and the indications for regional LND varied according to each institution. Second, since the adaptation of adjuvant chemotherapy also varied among the 348 institutions, the indications for adjuvant chemotherapy were not strictly determined. These two aspects may have affected the prognoses of the patients undergoing nephroureterectomy. Nevertheless, the results of this study should be considered significant and useful data since the outcomes of LNU were shown to not be inferior to those of ONU in muscle-invasive UTUC, when the patients are selected carefully.
Conclusions
Despite the limitations of this retrospective study, we found that oncologic control is not compromised with the use of LNU. Even in high-grade locally advanced tumors, LNU can achieve oncologic results comparable to those of ONU when the appropriate patients are selected. There is no evidence from our data that LNU is inferior to ONU with regard to oncologic outcomes.
Footnotes
Acknowledgments
The clinicopathologic statistics are the result of contributions from 348 institutions in Japan, and the authors are thus grateful for the cooperation of many Japanese urologists. This document was created by the Cancer Registration Committee of the Japanese Urological Association. Members of the Cancer Registration Committee of the Japanese Urological Association are as follows: Chikara Ohyama, Department of Urology, Hirosaki University Graduate School of Medicine; Hiroyuki Nishiyama, Department of Urology, Faculty of Medicine, University of Tsukuba; Masato Fujisawa, Division of Urology, Kobe University Graduate School of Medicine; Hirotsugu Uemura, Department of Urology, Kinki University Faculty of Medicine; Hiroyuki Fujimoto, Urology Division, National Cancer Center Hospital; Kazuhiro Suzuki, Department of Urology, Gunma University Graduate School of Medicine; Masatoshi Eto, Department of Urology, Graduate School of Medical Sciences, Kyushu University; Isao Hara, Department of Urology, Wakayama Medical University; Akio Matsubara, Department of Urology, Institute of Biomedical and Health Sciences, Integrated Health Sciences, Hiroshima University; Norio Nonomura, Department of Urology, Osaka University Graduate School of Medicine; Hiroyuki Nakanishi, Department of Urology, Graduate School of Medical Sciences, Kyoto Prefectural University of Medicine; Takuya Koie, Department of Urology, Hirosaki University Graduate School of Medicine; Hiroomi Kanayama, Department of Urology, Institute of Health Biosciences, The University of Tokushima Graduate School; Tsuneharu Miki, Department of Urology, Graduate School of Medical Science, Kyoto Prefectural University of Medicine; Tomoharu Fukumori, Department of Urology, Institute of Health Biosciences, The University of Tokushima Graduate School; and Seiji Naito, Department of Urology, Graduate School of Medical Sciences, Kyushu University.
Disclosure Statement
No competing financial interests exist.