
Abstract
Background:
Flexible ureteroscopic lithotripsy (URS) is rapidly becoming a first-line therapy for patients with renal and ureteral calculi. Most current medical infusion devices can only monitor infusion flow and pressure, but not renal pelvic pressure (RPP).
Patients and Methods:
We designed a patented intelligent system to facilitate flexible URS that included an irrigation and suctioning platform and a ureteral access sheath (UAS) with a pressure-sensitive tip, enabling regulation of the infusion flow precisely and control of the vacuum suctioning by computerized real-time recording and monitoring of RPP. A stable RPP was ensured by pressure feedback technology. Ninety-three patients with renal or ureteral calculi participated in the study and received flexible URS. Gravel particles were sucked out automatically during the flexible URS. Patients were evaluated on postoperative days 1 and 30 by X-ray of kidneys, ureters, and bladder to assess stone-free status.
Results:
In 81 of the 93 patients, only one surgery was needed to remove the stone. There were nine cases who failed the first surgery due to difficulty in placing the UAS, but flexible URS was performed in these patients after indwelling a Double-J stent to the ureter with the calculus for 2 weeks. Three cases were converted to percutaneous nephrolithotomy due to significant ureteral stenosis. For the 90 patients who underwent flexible URS, the actual RPP was controlled under 20 mmHg with clear operative visualization. The stone-free rates at postoperative days 1 and 30 were 90.0% (81/90) and 95.6% (86/90), respectively. Clavien I complications were noted in 13 cases, while Clavien II complications were noted in two cases. No major complications (Clavien III–V) were noted.
Conclusions:
Our patented system is technically feasible, safe, and efficient for treating upper urinary calculi. The advantages include breaking stones effectively and low complication rates because of its automatic control of RPP.
Introduction
S
To directly address the issue of high RPP and improve lithotripsy efficiency, we have developed a novel technique of flexible URS with a patented suctioning system that includes an irrigation and suctioning platform and a UAS with a pressure-sensitive tip, to control RPP automatically and treat upper urinary calculi efficiently. We reviewed our experience of this novel technique in managing renal caliceal and ureteral calculi for 93 cases and its safety and practicability were reported as below.
Patients and Methods
Patented irrigation and suctioning platform and UAS
As previously described, 11 this system included a patented irrigation and suctioning platform (Patent No. ZL201420055766.5, Fig. 1 A) and a patented UAS (Fig. 1B, C, patent No. 201420055134.9). The irrigation and suctioning platform comprised the main control unit, infusion device, suctioning device, and pressure feedback unit. On the platform, the perfusion flow, pressure control value, pressure warning value (20 mmHg), and pressure limit value (30 mmHg) could be preset. Vacuum suctioning pressure was adjusted by the main control unit through pressure feedback. There were four models to operate the platform, including automatic (perfusion, suctioning, pressure monitoring, and pressure feedback control), semiautomatic (pressure monitoring, perfusion), pure perfusion, and pure suctioning modes, respectively, allowing real-time display-monitored actual renal pelvic suctioning pressure and RPP. There were two connecting channels on the back end of the UAS, which were connected to the suction vacuum device and pressure monitoring feedback devices, respectively, wherein the suctioning channel can automatically suck out the stones, while the pressure monitoring feedback channel can monitor and automatically feedback to regulate RPP. The newly designed UAS with a pressure-sensitive tip was transparent. Its outer body diameter was 15F and working channel diameter was 11.55F; the length of the UAS was 20 to 45 cm. This system could precisely regulate the infusion flow and control the suctioning power by computerized real-time recording and monitoring of the RPP with the pressure feedback system, ensuring a stable RPP. 11

Clinical data
We retrospectively reviewed 93 patients with renal or ureteral calculus who received flexible URS using a holmium laser from November 2014 to September 2015. All the patients were diagnosed with upper urinary tract calculi by preoperative imaging studies, including color Doppler, intravenous urography, and CT. The size of stone was calculated by CT or X-ray of kidneys, ureters, and bladder (KUB). Ages of the patients ranged from 19 to 68 years with a mean age of 41 years. There were 69 patients with renal calculi only (renal pelvic calculus, 17; upper caliceal calculus, 9; middle caliceal calculus, 4; lower caliceal calculus, 18; mixed type, 21) and 17 cases with ureteral calculi only. The other seven cases were diagnosed with concomitant renal and ureteral calculi. There were 17 cases with a solitary kidney, 12 cases with renal insufficiency, 21 cases with a history of percutaneous nephrolithotomy, and 13 cases with a history of stone removal by open surgery. Preoperative urinary tract infection, renal insufficiency, hypertension, and pulmonary dysfunction were treated, and the operation was planned after all the indexes were improved. 11,12
Flexible URS procedure
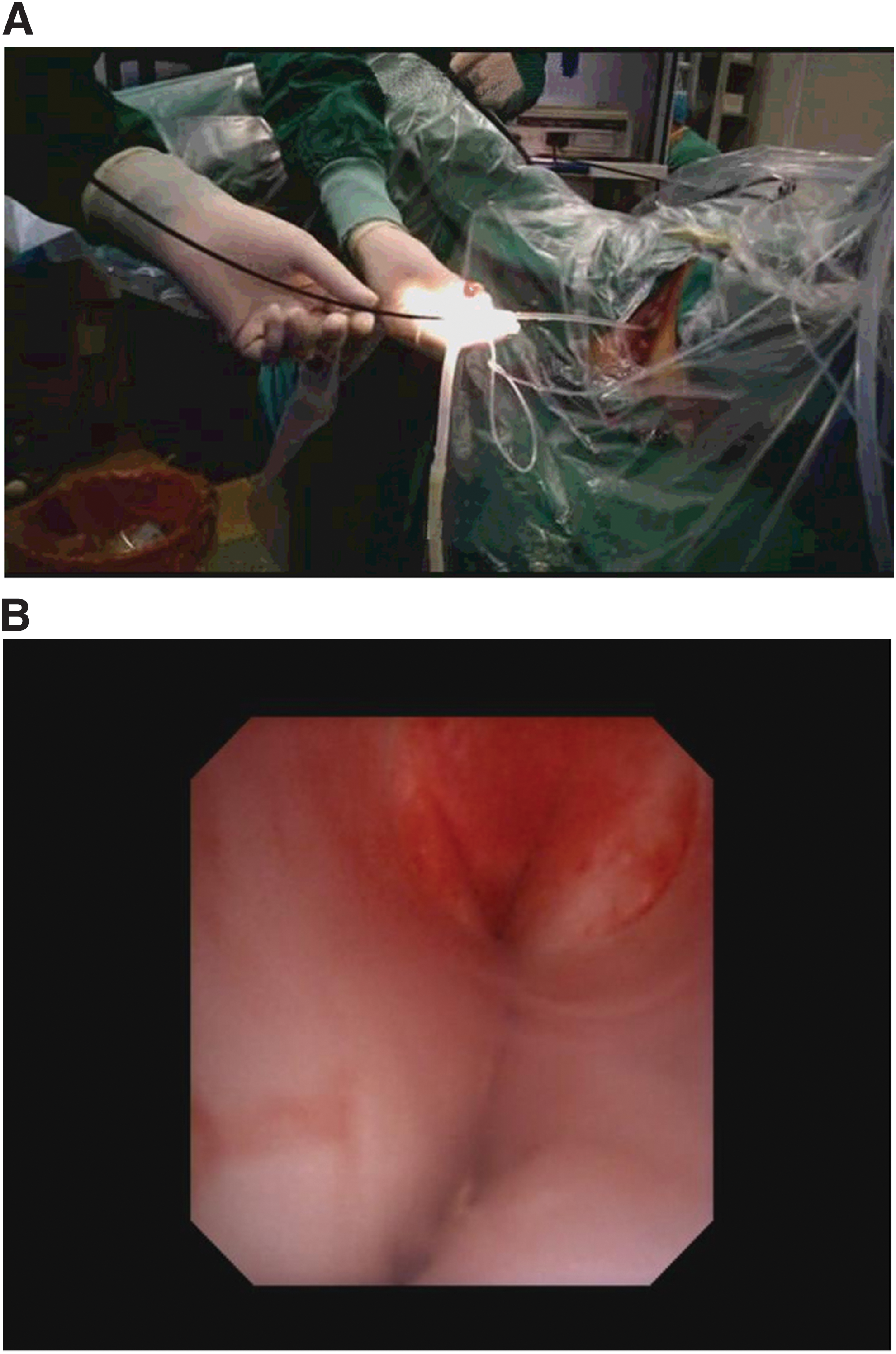
As we described previously, 11 all flexible URS procedures were performed under general anesthesia in low lithotomy position. Initially, a preliminary ureteroscopy was performed with a semirigid 8/9.8F ureteroscope (Richard Wolf, Germany) and a flexible 0.032-inch guidewire was inserted into the renal collecting system. Next, the patented UAS was inserted into the proximal ureter along the guidewire without the need of fluoroscopic guidance. A flexible ureteroscope (STORZ, Germany) was then inserted into the sheath to do a comprehensive inspection of the delivery location of the UAS (Fig. 2A), and mucosa of renal pelvis and ureter. After confirming that the transparent UAS was on the target position, the pressure sensory and suctioning channels were connected to the irrigation and suctioning platform. After being injected with water, a zero calibration was performed for the pressure sensory system. The fully automatic mode was chosen to operate the platform. Perfusion flow was then set at 100 mL/min; RPP control value was set at −2 mmHg; RPP warning value was set at 20 mmHg; and RPP maximum (limit) value was set at 30 mmHg. Intraoperatively, Holmium laser was used to crush the stone at 0.8 J/pulse with a frequency of 20 pulses/seconds (Lumenis, fiber diameter 200 μm). In the process of crushing the stone, the scope body was moved back and forth slightly in an uninterrupted manner inside the sheath distancing about 2 to 3 mm, to facilitate the small gravel particles inside the sheath gap to be sucked out. Gravel particles larger than the sheath gap, but less than the UAS in diameter were sucked out by withdrawing the scope intermittently without a need of stone basketing (Fig. 2B). At the end of the procedure, a 4.0F Double-J ureteral stent was placed, but will be removed 4 weeks after the surgery. 11 –14
Evaluation and statistics
All the surgeries were performed by one single expert surgeon. RPP was monitored closely during the surgery. Vital signs were closely monitored perioperatively. The complete blood count, serum electrolytes, nonreciprocal, and KUB were checked. Patients were evaluated on postoperative days 1 and 30 by KUB to assess stone-free status (Fig. 3). 13,14 Complications were evaluated according to Clavien classification. 15 CT scan was carried out for patients with radiolucent stones or residual stones. Stone free was defined as no residual stone or residual stone <4 mm in size. The operative time was counted from the beginning of lithotripsy to the end of the surgery. LIIR-20 automatic analysis system of infrared spectrum was used to analyze stone composition. 13,14

Comparison of pre- and postoperative KUBs. KUB, X-ray of kidneys, ureters, and bladder.
Statistical analyses were performed using SPSS 16.0. Descriptive analysis was performed to evaluate distribution patterns of patients' demographics, stone characteristics, and operation findings. Data with normal distribution were recorded as mean ± standard deviation. 11
Results
In 81 of the 93 patients, only one surgery was needed to remove the stone. There were nine cases who failed the first surgery due to difficulty in placing the UAS, but flexible URS was successfully performed in these patients after indwelling a Double-J stent to the ureter with the stone for 2 weeks. Three of the 93 cases were converted to percutaneous nephrolithotomy due to significant ureteral stenosis. For the 90 cases that the flexible URS was successfully performed, actual RPP was controlled under 20 mmHg with clear operative visualization and gravel particles were sucked out without the need of stone basketing.
As shown in Table 1, the mean stone size was 15.9 ± 5.2 mm (range: 8–35 mm). The mean operative time was 24.8 ± 15.9 (13–49) minutes. The stone-free rates (SFR) at postoperative days 1 and 30 were 90.0% (81/90) and 95.6% (86/90), respectively. There were four patients who had residual stone >4 mm in size requiring subsequent shockwave lithotripsy (two cases) or other managements (second ureteroscopy, one case; medication, one case). Clavien I complications were noted in 13 cases, including pain in 5 cases, fever in 4 cases, nausea/vomiting in 3 cases, and tachycardia in 1 case. Clavien II complications were noted in two cases with hypertension and infection, respectively. No Clavien III-V complications were noted.
Discussion
RPP usually remains lower than the backflow level (30 mmHg) during minimally invasive percutaneous nephrolithotomy. However, the probability of intraoperative RPP increase is higher in flexible URS due to the fact that the outflow channel is smaller and longer. Any factors that brought about poor drainage would result in temporarily elevated RPP greater than 30 mmHg, and many such occurrences of high RPP would have an accumulating effect creating enough backflow to cause bacteremia and postoperative fever. 3,16 High RPP is the risk factor for SIRS. 4 Fluid absorption can occur through pyelovenous-lymphatic backflow and pyelotubular backflow. Pyelovenous backflow usually occurred when RPP was above 30 to 35 mmHg. Also, as a result of high RPP, forniceal rupture could occur. 17 The absorption of perfusion fluid is also a high risk factor for postoperative fever. 18 Serious operative complications such as urosepsis could occur despite the rate being small, for 0% to 4.5%. The mortality rate was as high as 20% once it happened. 19 Control of RPP is therefore critical in preventing serious complications. In clinical practice, maintaining an RPP of less than 30 mmHg was recommended during percutaneous chemodissolution of upper-tract stones, instillation of topical chemotherapy or immunotherapy, and endoscopic lithotripsy. 20
In regular flexible URS, current commonly used UASs provide a reflow channel for perfused liquid and reduce the RPP to a certain extent. 8,9 However, they are not able to monitor and control the RPP. Also, liquid perfusion during regular flexible URS is mainly regulated manually, by infusion through IV tubing, or by syringe injection with low perfusion efficiency. The perfusion flow cannot be accurately set and adjusted in regular flexible URS with great randomness and uncertainty. Insufficient intraoperative perfusion often leads to poor surgical visualization. On the other hand, using too large perfusion flow to meet the need of clear visualization often results in high RPP. 21 Moreover, the regular flexible URS without a highly efficient stone clearance system relies mainly on stone basketing to extract stone discontinuously, which is time-consuming with incomplete stone clearance and easiness to form steinstrasse. These problems to some extent have limited the clinical application of flexible URS for managing upper urinary tract calculi. 10 In Blew BD's report, 21 foot control type continuous infusion pump could only monitor infusion flow and infusion pressure, but not the RPP simultaneously. There was previous report that endoluminal isoproterenol irrigation could decrease RPP during flexible ureterorenoscopy. However, the perfusion flow they used was only 8 mL/minutes, limiting the surgical visualization. 22 Should they choose a higher perfusion flow, they cannot guarantee that the RPP is below the warning value since they do not have related device to monitor and control the pressure. The other disadvantage of this approach is its inability to suck out broken stone pieces actively as our device does, limiting its stone clearance efficiency.
Our patented system comprises the irrigation and suctioning platform and the UAS. The material of this sheath is hard and transparent, which enables us to place the UAS on target position with monitoring under direct visualization, to avoid intraoperative damage. One side of the cavity is connected to a vacuum suctioning tube with ability to extract small gravel particles through the sheath gap intraoperatively. Gravel particles larger than the sheath gap but less than the UAS in diameter can be sucked out by withdrawing the scope intermittently without a need of stone basketing. The other channel of the UAS was connected to the pressure monitoring and feedback system with the ability to monitor and adjust the RPP automatically. 11 This system therefore has the following functions: (1) can set the RPP control, warning, and limit values according to operative needs; (2) can receive intraluminal pressure numerical from the UAS. In the meantime, the system can automatically adjust the vacuum suctioning according to the preset pressure control value by means of pressure feedback control technology, to keep RPP constant in the preset safety range at different perfusion flow rates. When the system in case of a variety of reasons leads to elevated RPP higher than the warning value, an alarm will be activated. When the RPP is higher than the limit value, the system will automatically shut down for protection; (3) can real-time display each parameter dynamically and store the records. 11
In summary, the patented system for our flexible URS has the following advantages: first, it can monitor and control the RPP and better help operator in the intraoperative monitoring and automatic control of patient's RPP, reducing the complication rates of postoperative fever and urosepsis. It can also further facilitate investigation of safe RPP range during the flexible URS, promoting the popularization of flexible URS technique and the development of dynamics of upper urinary tract. Second, the hands-free irrigation device has the advantages of simple operation and meeting the need of continuous perfusion flow for continuous crushing of stone, to ensure clear operative visualization, improving the stone-breaking efficiency and shortening the operative time. Even if the stone is more than 2 cm in diameter, it can usually be cleared in one surgery by using our patented system. Third, the patented system can suck out the gravel particles automatically at high efficacy, while crushing the stone using the holmium laser, without a need of stone basketing that is commonly used currently, but is time-consuming, greatly reducing the rate of postoperative residual stone and the occurrence of stone street, and medical cost.
In this study, both the operative time and complication rate for patients were lower compared with literature reports. 4,23,24 One surgery SFR was as high as 95.6% without the occurrence of urosepsis. In Takazawa's report, the SFR was only 90% after averaging 1.4 times flexible URS, and 5% (1/20) of the patients in his study had complication of sepsis. 25
Of course, this study is only a retrospective descriptive study; there was no strictly designed control group to compare the safety and effectiveness of the new technique over traditional technology. Also, our case number is relatively small. 11 In the future, we will continue to do further research in this area.
Conclusion
Our patented system is technically feasible, safe, and efficient for treating upper urinary calculi. Its advantages include breaking stones effectively and low complication rates because of its automatic control of RPP.
Consent
Written informed consent was obtained from the patients for publication of this report and any accompanying images. Copies of the written consent are available for review by the editor of the journal.
Compliance with Ethical Standards
Ethical and regulatory approvals for this study were sought and obtained. All procedures performed in this study were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
The research project was funded by the Science and Technology Department of Jiangxi Province with a major scientific fund number of 20152ACG70009, and the Science and Technology Bureau of Ganzhou City, Jiangxi Province with a major scientific fund number of 2014-131.
Footnotes
Acknowledgment
We made an abstract presentation for this study at the 2016 American Urological Association Annual Meeting at San Diego, CA.
Author Disclosure Statement
No competing financial interests exist.