
Abstract
Objective:
To compare three laparoscopic surgical techniques for the treatment of ureteropelvic junction obstruction (UPJO), assessing their difficulty, operating time, effectiveness, and complications.
Materials and Methods:
The clinical histories of 54 patients with UPJO who underwent a laparoscopic procedure between June 2003 and September 2013 were reviewed. Anderson–Hynes (A-H) pyeloplasty was performed on 34 patients, nondismembered pyeloplasty on 11 cases (8 Y-V Foley plasty and 3 Fenger plasty), and cephalad vascular displacement or Hellström technique (HT) on 9 patients. The patients were selected for the different techniques depending on the findings during the procedures, according to renal pelvic size and the presence of crossing vessels. We compared the techniques according to intraoperative and postoperative outcomes. Complications were interpreted following the Clavien–Dindo classification. The success rate was defined as the absence of clinical symptoms and normal diuretic renography. Analysis of variance and chi-square tests were used for the statistical analysis.
Results:
Mean follow-up was 55.58 months. The success rate achieved was 88.5% for A-H pyeloplasty, 90.9% for nondismembered pyeloplasty, and 100% for HT (p > 0.05). HT was the least time-consuming: 124 ± 30 vs 202 ± 44 minutes of A-H pyeloplasty and 147 ± 27 minutes of nondismembered plasty (p < 0.005). Mean hospital stay was 6.7 ± 1.4 days for A-H pyeloplasty, 6.6 ± 2 days for nondismembered pyeloplasty, and 3.42 ± 1.5 days for HT (p < 0.05). The postoperative complication rate was 21.1% for A-H pyeloplasty, 18.8% for nondismembered pyeloplasty, and 12.5% for HT (p > 0.05). None of the cases required open surgery, and urinary fistula was the most frequent complication.
Conclusion:
Intraoperative observation of ureteropelvic junction allows selecting cases to undergo nondismembered pyeloplasty techniques, achieving similar results to A-H pyeloplasty, reducing operating time, complication rate, and hospital stay.
Introduction
S
With the purpose of simplifying the procedure, some authors have reintroduced pyeloplasty Y-V Foley 5 and Fenger pyeloplasty (FP) 6 for the laparoscopic approach. These techniques do not require dismembering the pelvis, which significantly reduces the difficulty of the suturing. Moreover, when the crossing vessels (CVs) are displaced, the pyeloureteral cavity is left intact, 7 adapting the technique described by Hellström in 1949. 8
The different laparoscopic techniques used in our hospital to treat UPJO are compared, analyzing intraoperative and postoperative results. The goal of this article is to consider the possibility of using nondismembered laparoscopic techniques such as Y-V plasty or Hellström technique (HT), against A-H dismembered pyeloplasty.
Materials and Methods
A retrospective review was conducted of all patients treated for UPJO by the laparoscopic approach in our hospital. From June 2003 to September 2013, a total of 54 patients, 28 male and 26 female, mean age 39 years old (r = 14–71), underwent transperitoneal laparoscopic pyeloplasty. UPJO was primary in 48 cases (88.9%), and secondary, after failure of antegrade endopyelotomy, in 6 cases (11.1%). Diagnosis was based on symptoms, findings in intravenous urography and diuretic renography with TC-99m. In some cases, the study was completed with angio-CT to assess the presence of CVs. A percentage of differential renal function >20% was required for pyeloplasty. The patients were selected for the different techniques depending on the findings during the procedures, according to anatomic criteria. A-H plasty was performed on 34 patients with dilated pelvis (76.4% with CVs); 11 patients with moderately dilated pelvis underwent nondismembered pyeloplasty (Y-V plasty was performed on 8 cases and FP on 3 cases), associated with displacement of CVs in 5 cases. HT was performed on nine patients (Table 1).
Surgical technique
All of the patients were placed in a lateral decubitus position under general anesthesia. Ureteral catheter was not placed to avoid decompression of the renal pelvis, observing the factors that might contribute to pelvic distension. The pneumoperitoneum was performed in a standard manner. Four trocars were used, a 10 mm one for the laparoscope and suturing, and three 5 mm ones.
Once the colon was mobilized medially, the proximal ureter was located and released until the ureteropelvic junction (UPJ). The dissection of the pelvis allowed us to observe its volume, ureteral insertion, and the presence or absence of CVs. To reduce the pelvic size, we performed dismembered pyeloplasty on patients with large pelvis, regardless of CVs. For moderate pelvis without CVs, a nondismembered pyeloplasty was performed and, in case of CVs, they were dissected and displaced cephalad, far from the UPJ, while simultaneously decreasing the pneumoperitoneum pressure to 8 mm Hg. It was ensured that UPJ presented a normal morphology, the size of the pelvis was reduced, and peristaltism was correct. To verify it, a 16-gauge Angiocath was inserted through the flank of the patient, placing it on the anterior side of the renal pelvis, and 50 mL of saline was injected, following the drain of the renal pelvis. When the drain of the renal pelvis is correct, the CV is wrapped on the anterior side of the pelvis with three stitches of Vicryl 3.0 (Fig. 1). If there is no adequate drainage, or in doubt, after wrapping the CV, a nondismembered pyeloplasty is performed (Fig. 2). A Double-J catheter is placed on these patients and on the ones undergoing dismembered pyeloplasty as well. On the contrary, a catheter is not placed when the CV is wrapped.
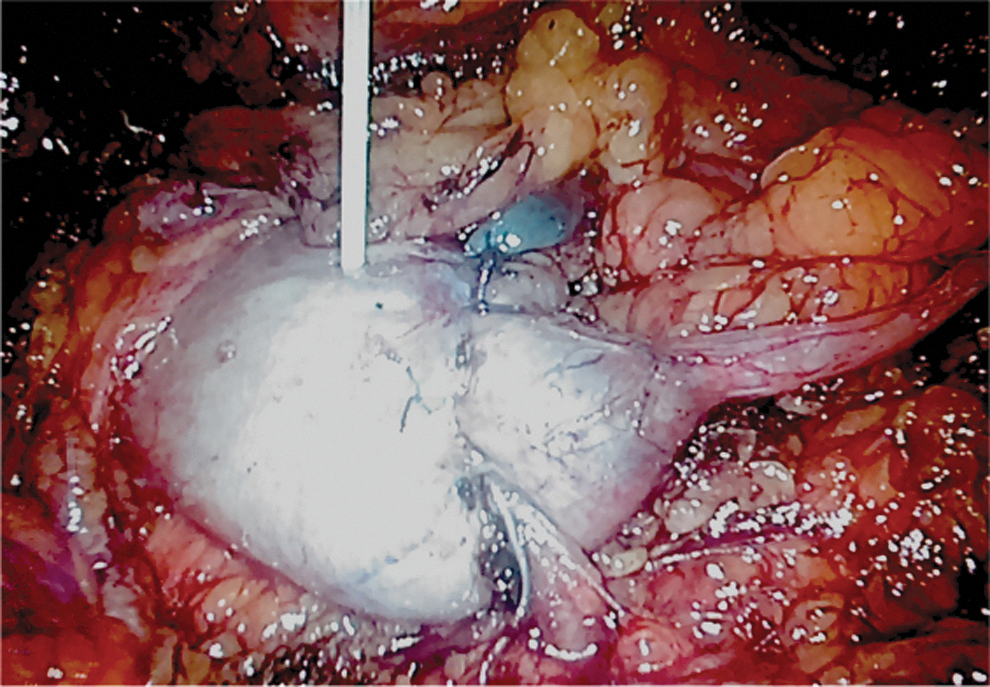
Absence of renal pelvis dilation with the saline serum injection after performing Hellström technique.
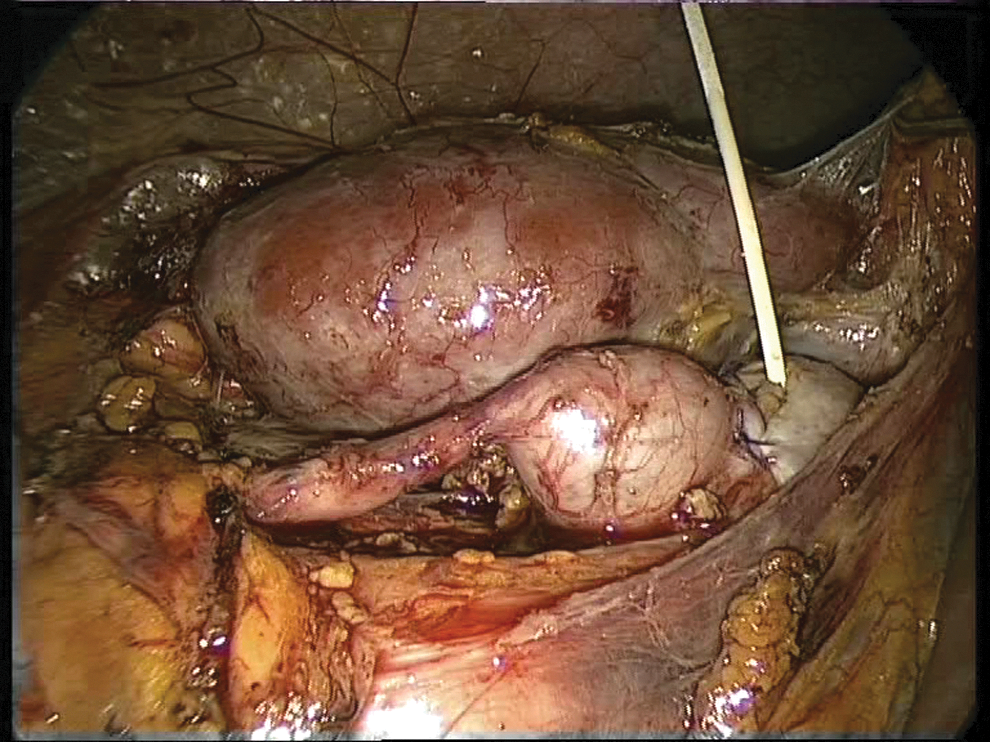
Dilation of the renal pelvis with the saline serum injection after performing Hellström technique indicates the need of nondismembered pyeloplasty.
The success rate was evaluated as the absence of symptoms and standard elimination curves in diuretic renography.
Statistical analysis was done with Windows SPSS. The results of the different techniques were compared by the analysis of variance test and chi-square test with a 0.05 statistical significance.
Results
All the procedures were completed without reconversion. Mean follow-up was 55.58 ± 41.3 months. Success rates were 88.2% for A-H plasty, 90.9% for nondismembered pyeloplasty, and 100% for HT (p > 0.05). Mean surgical time for A-H plasty was significantly longer than for the other two techniques (202 ± 44 minutes) vs 147 ± 27 minutes for Y-V Foley and Fenger plasty and 124 ± 30 minutes for HT (p < 0.05). Mean hospital stay was 5.5 ± 2, 5.8 ± 3, and 2.75 ± 0.8 days for A-H plasty, nondismembered pyeloplasty, and HT, respectively (p > 0.05). Two patients presented intraoperative complications during placement of trocars: minimum aortic lesion when introducing the first trocar in a thin male and which required one stitch; and transverse colon lesion when introducing the second trocar that required primary suturing. There were no complications directly associated to the techniques used. The global postoperative complication rate was 18.5%: nine patients were Clavien 1 and only one Y-V patient needed ureterorenoscopy to replace the Double-J catheter (Clavien 3). The itemized rate was 21.1% for A-H plasty, 18.8% for nondismembered plasty, and 12.5% for HT (p > 0.05), with urinary fistula as the most frequent complication (Table 2).
Discussion
For over a century, multiple techniques to resolve UPJO have been described in the literature. 9 In 1993, Schuessler described A-H laparoscopic pyeloplasty, 1 which has become the first choice treatment for UPJO, as its renders better results than endopyelotomy, which only tackles the intrinsic factor, whereas A-H plasty acts upon both, intrinsic and extrinsic factors. Undoubtedly, A-H plasty presents a technical difficulty due to the wide intracorporeal suturing that requires careful reconstruction and may bring about leaks that lengthen the hospital stay. Fully aware of these drawbacks and with the purpose of simplifying the procedure, some authors have used nondismembered techniques, such as Y-V plasty, 5 FP, and HT. 8 At first, HT was not widely accepted because the surgeon faced the possibility of missing an intrinsic factor (stenosis).
Undeniably, when an A-H plasty is performed, all the possible causes of obstruction are corrected, that is, the pyeloureteral segment that may or may not present stenosis is dissected, the volume of the renal pelvis is reduced, and when displacing the CVs systematically, a possible extrinsic compression is eliminated; nevertheless, these maneuvers may be the object of debate.
A first point of controversy is the importance of the results achieved when reducing the size of the pelvis. While for some authors the techniques that do not involve reducing a large pyeloureteral segment have a greater probability of failure, 3,10 for others, reduction does not contribute to improving the results. 11 Unfortunately, there are no randomized studies that might help us to decide which viewpoint is right. Szydelko 12 compares a series of 50 patients who underwent A-H plasty with 35 Y-V plasty with similar success rates, 91.8% vs 91.2%, respectively, and concludes that pelvis volume reduction is unnecessary. However, as the patients who underwent Y-V plasty were chosen due to a lower degree of difficulty during the learning curve, he recommends performing this technique on small pelvis. Janetschek 6 reports a 98% success rate in a series of 67 FP, where a CV was found in 80% of the cases. The author recommends performing A-H plasty only in cases where dorsal CV displacement becomes necessary. Based on our previous study, regarding the predictive factors of antegrade endopyelotomy failure, where a pyelocaliceal area larger than 30 cm2 was an indicator of a bad outcome regardless of finding a CV, 13 in this series, we have resorted to A-H plasty for large pelvis with the purpose of reducing volume and used nondismembered techniques for the rest of the cases, making the procedure easier and reducing operating time.
The other point of controversy is the role of the CVs in UPJO etiology. Owing to the involvement of CVs in UPJO and with the purpose of avoiding possible hemorrhage complications, it was of utmost importance to find out whether or not there were CVs before the procedure. In this article, Van Cangh 14 communicates a drop on the antegrade endopyelotomy success rate from 82% to 33% in the presence of CVs, demonstrating that the mere presence of a CV pressing on the UPJ might be the cause of obstruction. Nakada 15 had similar results in his series of patients who underwent retrograde endopyelotomy with Acucise catheter. The author reports 92% success rate in patients without CVs, which becomes 64% in patients with CVs. However, his article also shows that endopyelotomy did not always fail when CVs were found, as 31% of the patients with CVs showed a long-term positive outcome. There are other studies with a large number of cases which show that CVs were scarcely relevant in the outcome. In the series presented by Gupta, 16 only 4% of the failures were associated with CVs; for this reason, the debate remained open. Moreover, thanks to intraluminal ultrasonography, it was demonstrated that CVs at UPJ may appear in at least 19% of normal individuals. 17 Using color Doppler ultrasonography, Janetschek 18 studied volunteers with normal pelvis and found CVs 5 mm from the UPJ in 35% of the cases. Thus, it can be inferred that the presence of CV does not necessarily mean it should always be the cause of the obstruction and, in the same way, CV displacement is not always necessary in laparoscopic treatment. Notwithstanding, the same author performed FP on 67 patients and displaced the CVs found in 80% of the cases. The UPJ incision did not show intrinsic stenosis in 77% of the cases, 6 which indicates that vascular compression was the only factor involved in more than half of the cases and a simple vascular displacement would have solved the obstruction.
In our opinion, this controversy loses relevance nowadays thanks to laparoscopy. Undoubtedly, the laparoscopic approach provides a clear vision of the UPJ anatomy and helps to clarify the cause of obstruction. After a meticulous dissection of the UPJ and CVs, it is possible to displace them far from the UPJ and verify whether the volume of the pelvis has varied and observe the behavior of the peristalsis. This simple technique, described by Hellström 8 decades ago, was used again in 2003 by Meng and Stoller 7 with excellent results on 9 patients with small pelvis, normal morphological upper ureter, and UPJ. In a series of 42 patients and a 29-month follow-up, Nouralizadeh 19 cuts the vein and displaces only the artery, achieving a 90% success rate. The author bases his decision on the fact that after furosemide infusion, the pelvis drains properly and its movement is adequate.
Our series was performed in a similar way: observation of pelvis after furosemide infusion with low pressure at the pneumoperitoneum; in addition, an injection of saline directly into the pelvis helped in the selection of patients. There were 14 patients selected during procedure to undergo HT. Five of them presented completely full pelvis even though peristaltism and morphology at UPJ were normal, for this reason, UPJ was cut after vessel displacement. It is true that there are no urodynamic data to support the decision of not opening the UPJ and the pelvis pressure reached after injection is unknown. Perhaps there might be a slight bias in the selection due to false negatives; however, the maneuver did not give any false positives as shown in the nine patients who did not present full pelvis after a quick saline injection. So far, the literature only presents a study where the Whitaker test has been used (six patients), showing that vessel displacement was an effective technique 20 ; nevertheless, in the usual surgical practice, it is impractical to perform a Whitaker test systematically, whereas the technique proposed here is fast and simple. Our study showed similar success rates using the three techniques, but outstanding results were obtained using HT, just as other authors report. 7,19
Conclusions
Laparoscopy offers an excellent field to observe the factors that cause UPJO. The selection of patients on whom to perform techniques that do not displace vessels or displace them without disturbing the UPJ may simplify this procedure, achieving the same outcomes as those obtained by the dismembered technique.
Footnotes
Author Disclosure Statement
No competing financial interests exist.