
Abstract
Objective:
We evaluated the effects of continuous instillation of a local anesthetic at the nephrostomy site on postoperative pain following percutaneous nephrolithotomy (PCNL).
Patients and Methods:
Sixty patients who underwent PCNL between August 2013 and March 2015 were enrolled in this randomized prospective study. The following three groups comprising 20 patients each were analyzed: Group A, continuous infiltration of local anesthetic at the nephrostomy site; Group B, local anesthetic injected only once; and Group C, 0.9% saline injected as a control at the end of the procedure. Postoperative patients reported pain scores, and amount of analgesic use was recorded at 2, 6, 12, 24, and 48 hours after the surgery.
Results:
The mean pain scores of patients in Group A and B were significantly lower compared with Group C patients as much as 12 hours postoperatively (p = 0.001). However, at 24 hours postoperatively, the mean pain scores of Group B and C patients became comparable, while those of Group A patients remained significantly lower until 48 hours after the surgery (p < 0.001). Patients in Group A and C demanded the least and greatest amounts of analgesics, respectively, at all-time intervals (all p < 0.05).
Conclusions:
Continuous infiltration of a local anesthetic is effective for both managing pain immediately after surgery and in dealing with pain that occurs late in the recovery period.
Introduction
S
Ropivacaine is an amide used as a local anesthetic with an intermediate duration of action. Ugras et al. compared postoperative pain and pulmonary function between a group of patients with ropivacaine instilled into the nephrostomy tract and a control group. The authors reported that both postoperative pain and pulmonary function improved in the treatment group compared with the control group. 6 However, the single injection of a local anesthetic immediately after surgery would not efficiently alleviate pain while the nephrostomy tube is in place, because of its limited duration of action.
In our current study, we therefore aimed to evaluate the efficacy of the continuous instillation of a local anesthetic into the nephrostomy tract, which has never been reported previously, and to compare the effects of this approach with either a single injection of local anesthetic or a control group.
Patients and Methods
Overview
Our current prospective randomized study was conducted in accordance with good clinical practice guidelines and the Declaration of Helsinki. After receiving approval from the institutional review board committee for human subjects at our institution, written informed consent was obtained from each participant before enrolment. All aspects of this study, including its design, data collection, data analysis, interpretation of data, and writing the article, were carried out without the input of the sponsors of this study.
Patients and treatment procedures
A total of 63 adult (≥18 years old) patients with nephrolithiasis who were scheduled to undergo PCNL between August 2013 and March 2015 were enrolled in the analyses. Exclusion criteria were as follows: age more than 60 years; obesity (body mass index >30); chronic analgesic use; prior PCNL; and requirement for multiple access tracts during the surgery.
Patients were randomly assigned to one of the three study groups using computer-generated random numbers. All patients in each group received standard general anesthesia, which was induced by intravenous propofol 2 mg/kg along with effect-site target-controlled infusion of remifentanil (2 ng/mL) maintained by desflurane inhalation. Intravenous rocuronium 1 mg/kg was administered to facilitate tracheal intubation. After inducing general anesthesia, cystoscopic placement of a 5F ureteral catheter followed by percutaneous puncture under fluoroscopy guidance was performed in each patient. Balloon dilator was used to dilate the tract to 30F after placing a guidewire. A 26F rigid nephroscope was used to visualize the field, and stone(s) were fragmented using an ultrasonic lithotriptor.
After fragmentation of the stone(s), a 14F Malecot nephrostomy tube was positioned through the puncture site. A single experienced surgeon who was blind to the randomization of patients performed each procedure. In Group A patients, a 1:1 mixture of saline with 0.2% ropivacaine was continuously instilled until 24 hours after surgery, at a rate of 3 mL/hour using a portable infusion device (Ambix Anapa continuous type®; Ewha Fresenius-Kabi, Inc.; Fig. 1), which was administered through a 5.7 cm injectable catheter in the puncture site beside the nephrostomy tube. It was placed close to the nephrostomy tube, usually at 0.2 to 0.3 cm distance. The injectable catheter had multiple holes every 0.3 cm interval, therefore making it possible for local anesthetic to be instilled evenly throughout the tract, from the subcutaneous tissue to fascia.
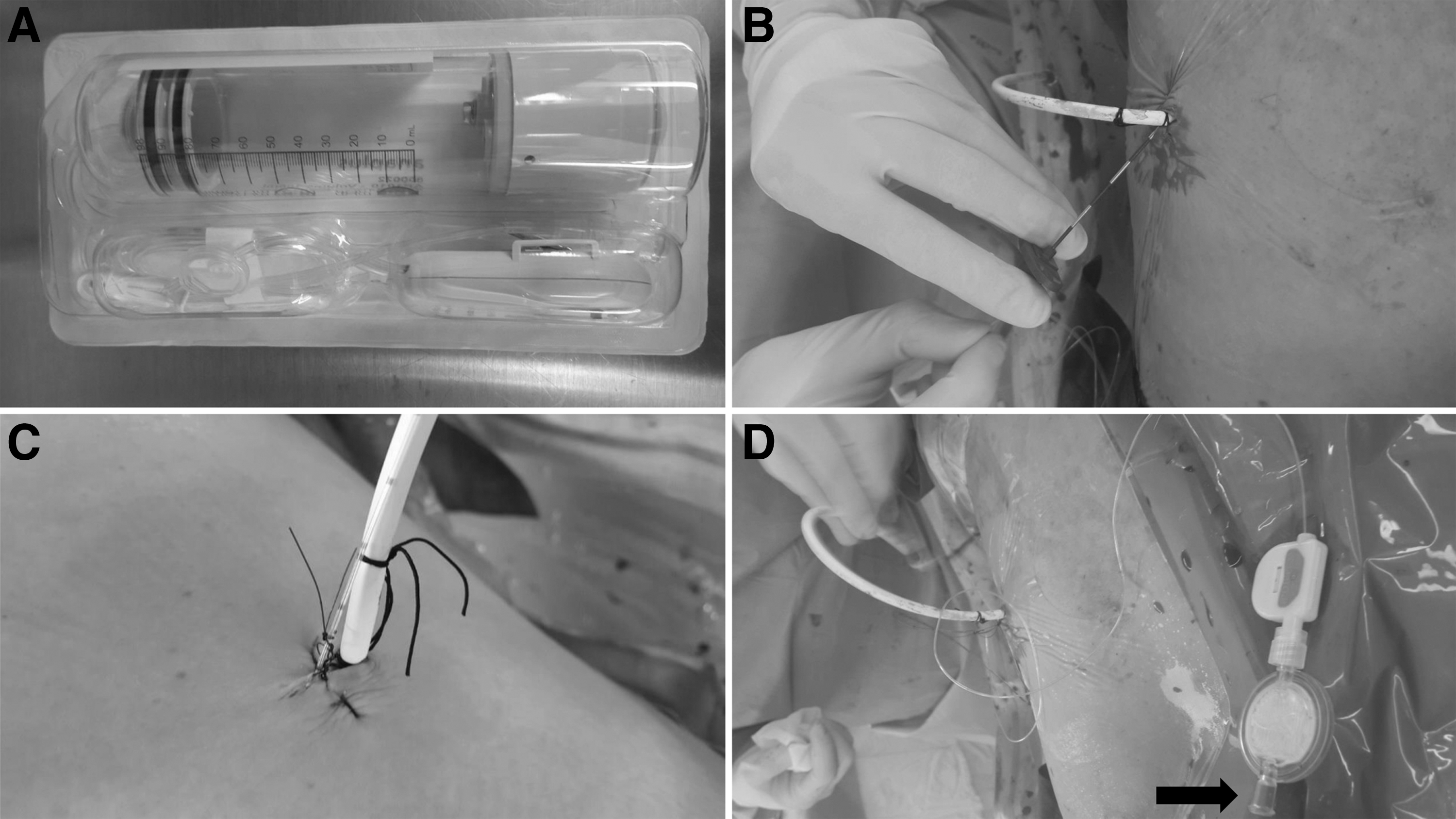
Continuous instillation of a 1:1 mixture of saline with 0.2% ropivacaine by the portable infusion device (Ambix Anapa continuous type®) in Group A patients
The procedure was performed by medical personnel besides the surgeon. Group B patients had 35 mL 0.2% ropivacaine injected slowly using a 23-gauge needle into the puncture site from the subcutaneous tissue to the fascia. Thus, similar amounts of ropivacaine were instilled in both Group A and B patients. In Group C patients, 35 mL 0.9% saline was injected instead of ropivacaine into the same layers as patients in Group B.
All patients received the following standardized postoperative pain control regimen: tramadol HCl 50 mg per os every 8 hours routinely on postoperative days 1 and 2, as well as intravenous meperidine 25 mg on demand. The postoperative heart rate, pain scores, and amounts of narcotic analgesic consumption at 2, 6, 12, 24, and 48 hours were recorded. Pain scores were assessed using visual analog scale (VAS) scores that ranged from 0 to 10, with 0 representing no or minimum pain and 10 representing the maximum pain perceived by a patient. The amounts of analgesic used were recorded as the number of demands during the study period. At 48 hours after surgery, the nephrostomy tube was removed and all patients were discharged on postoperative day 2.
Statistical analyses
Because there was no reference on the continuous local anesthetic instillation, we could not estimate the difference of pain score between Group A and other groups. Instead, we performed power analysis after the study. Group sample sizes of 20 achieved 85% power to detect a difference in pain score between Group A and B at postoperative 24 hours, with a two-sided significance level of 0.025. Statistical comparisons between groups were conducted using the Student's t-test for continuous variables and the chi-squared (χ2) test for categorical variables. Normal distribution of continuous variables was assessed by the Kolmogorov–Smirnov test. The unpaired Student's t-test with two-tailed significance was used to compare the mean VAS scores and the amount of analgesic used, as these variables showed normal distributions. All statistical analyses were performed using SPSS for Windows®, version 18.0 (SPSS, Inc.), and a threshold for statistical significance was set at p < 0.05.
Results
Among the 63 enrolled patients, we excluded 2 patients who had stones making the patients candidates for requiring multiple access tracts. After the surgery, one patient in Group B exhibited an allergic reaction (skin rash) to tramadol HCl and was withdrawn from the study. Thus, 60 patients were ultimately included in the study series, making patients evenly distributed to Groups A, B, and C (Fig. 2). The mean stone size was 3.7 ± 1.5 cm, while the average operative time was 74.1 ± 40.5 minutes. There were no significant differences between the study groups in terms of patient demographics or perioperative parameters (Table 1).
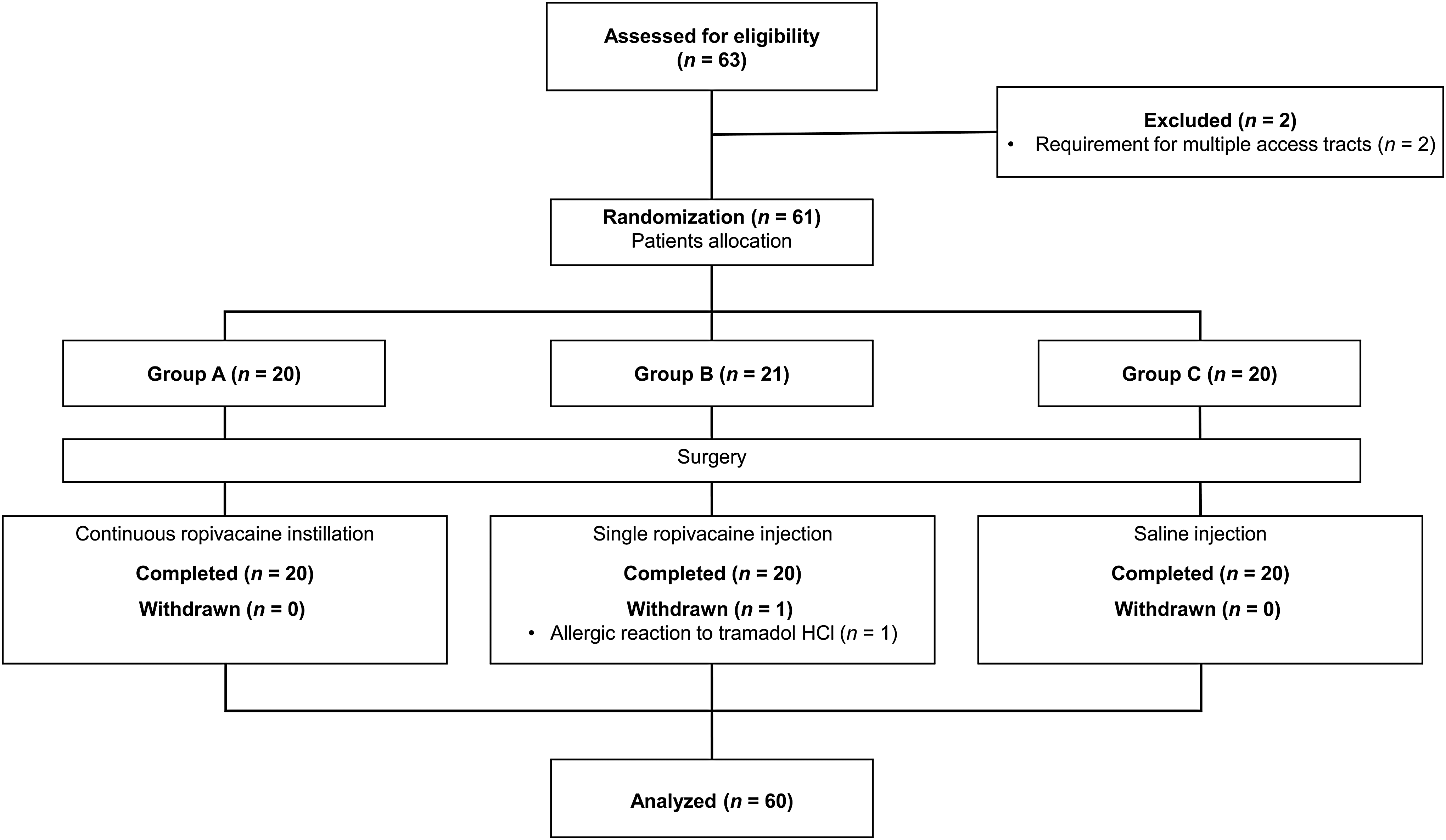
Study enrollment.
BMI = body mass index; SD = standard deviation.
No statistically significant differences were detected between cohorts for the mean heart rates at any time interval (data not shown). The mean VAS scores of patients in each group also showed no significant differences until 6 hours postoperatively; however, the mean VAS scores of Group A and B at 12 hours postoperatively showed a significant difference compared with those of Group C (p = 0.001; Fig. 3). At 24 hours postsurgery and thereafter, the mean VAS score of Group A patients remained lower compared with Group C patients, while those of Group B patients became similar to Group C patients.
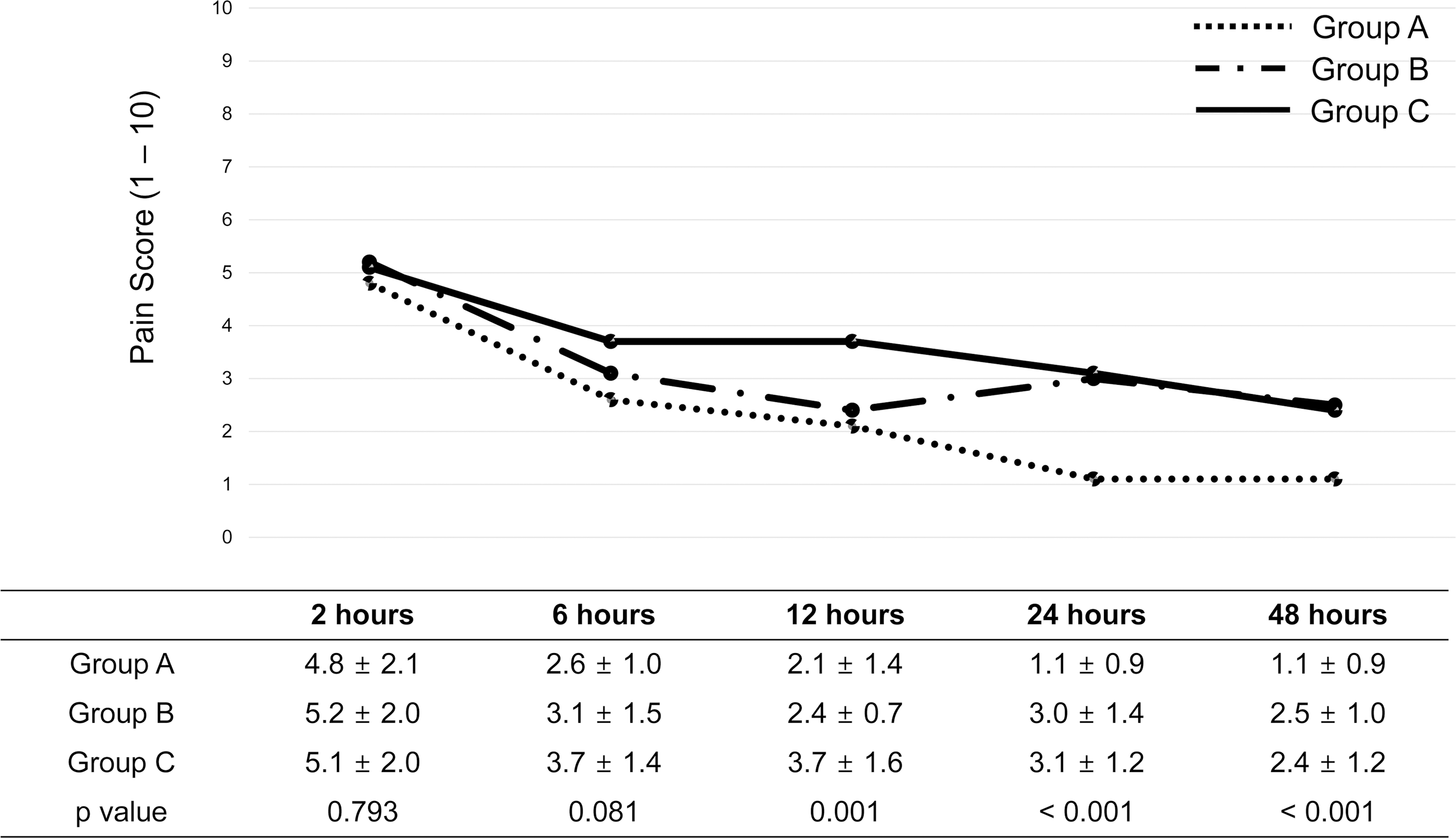
Change in the mean postoperative pain scores.
Trends for decreasing VAS scores were identified in all groups as much as 12 hours postoperatively, but the mean VAS score of Group B patients increased from postoperative 12 to 24 hours, whereas those of Group A and C patients continued to decrease thereafter. The average total use of intravenous meperidine as much as 48 hours postoperatively in Group A, B, and C patients was 37.5 ± 6.5, 107.5 ± 32.4, and 152.5 ± 34.1 mg, respectively (p < 0.001). Patients in Group A and C demanded the least and greatest amounts, respectively, of analgesics at all-time intervals (all p < 0.05; Fig. 4). No notable adverse effects related to either continuous infiltration or single injections of local anesthetic during recovery period were noted.
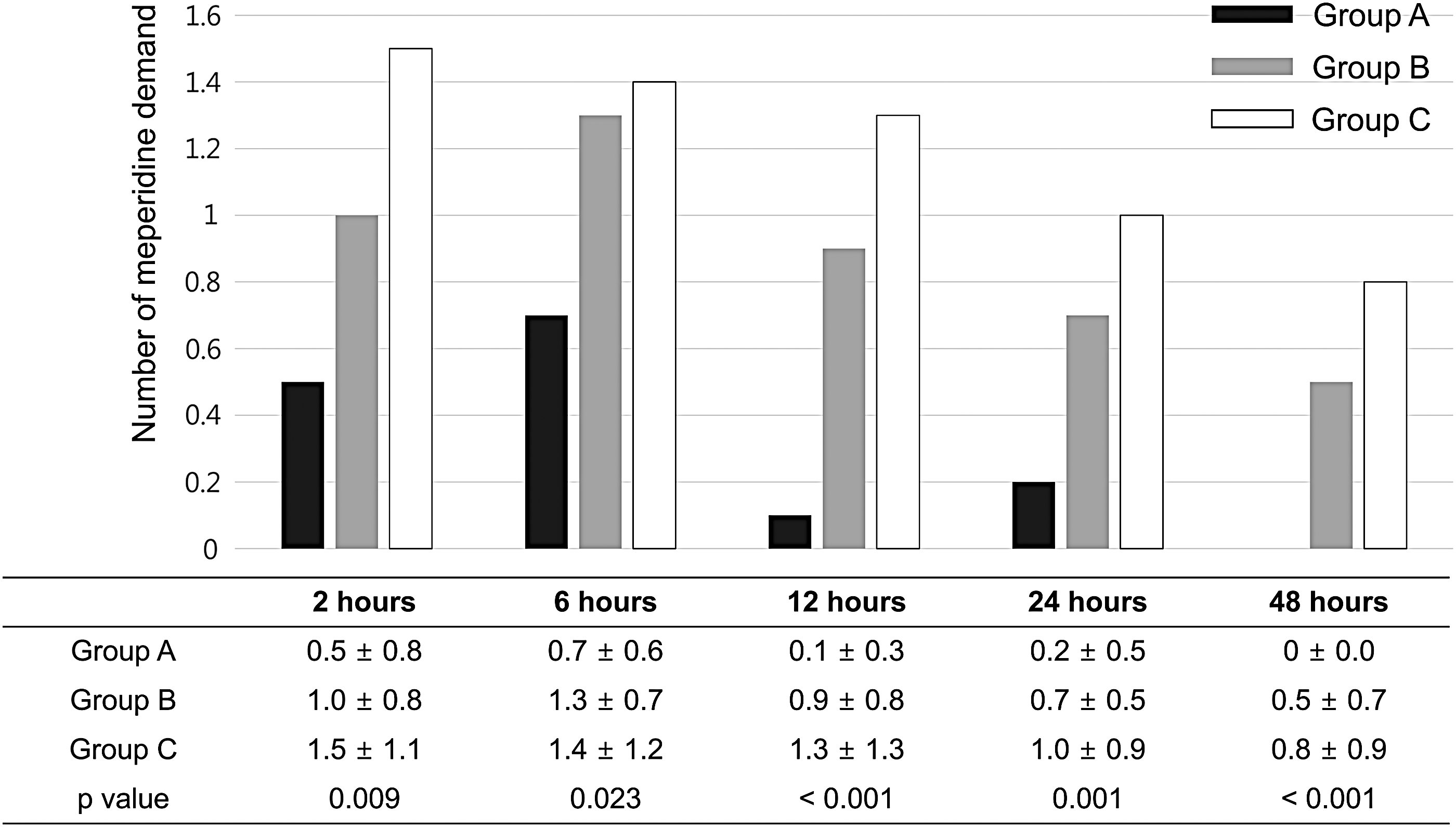
Changes in the mean amount of postoperative meperidine use.
Discussion
Postoperative discomfort in patients who undergo PCNL is generally thought to be associated with puncture site pain, which is related to the nephrostomy tube. 2,7 Thinner nephrostomy tubes have been reported to cause less pain and analgesic consumption immediately after surgery, 2 and tubeless procedures may even significantly improve patient comfort following PCNL. 8 However, in case of a relatively large stone burden, a nephrostomy tube must be placed into the puncture site for adequate drainage to prevent hematoma formation as in our series that the mean stone size was 3.7 ± 1.5 cm.
To manage pain associated with the surgical site, many studies in the urology, as well as the general surgery and gynecology literature, have described the efficacy of local anesthetic infiltration at sites of surgical incision. In these reports, the injection of local anesthetic at the surgical site in patients undergoing mastectomy, thyroidectomy, or cesarean section has been shown to be safe and effective in reducing postoperative pain. 9 –11 The efficacy of injecting local anesthetics at the puncture site after PCNL has also been thoroughly investigated, and this approach has been reported to be effective in managing postoperative pain. 5,6 However, whether a single injection of local anesthetic alone at the surgical site can reduce pain while the nephrostomy tube is in place remains the subject of debate, because of its limited duration of action. In one previous report, patients reported pain scores that were not significantly different between patients who had Marcaine or a placebo injected into the puncture tract after PCNL. 4
To overcome such challenges, several recent studies have investigated the effects of injecting local anesthetics that have a long duration of action into the puncture site, including bupivacaine and levobupivacaine. 4,5,12 However, the estimated half-life of bupivacaine is about 2 hours, 13 so a single injection might not be sufficient to control postoperative pain while the nephrostomy tube is in place after PCNL. Indeed, patients undergoing PCNL often complain about distracting pain, even at 48 hours after surgery, 4 suggesting that achieving sustainable pain management is likely to be important for improving patient comfort. Although it has high liposolubility and a relatively long half-life, the effects of ropivacaine can only be sustained for 12 hours, 6 and patient-reported pain scores and pain medication needs after 24 hours have been reported not to significantly differ between patients who received a single injection and controls. 6 In our present study, using ropivacaine as a local anesthetic, we developed a novel method for continuous instillation of local anesthetic using a portable infusion device administered through a catheter inserted into the nephrostomy site.
We confirmed that the effect of single injection of local anesthetic did not last until 24 hours after the surgery based on our current analyses. Meanwhile, the mean VAS score of Group A patients remained low with a value of nearly 1 even 48 hours after the surgery, which was significantly different from Group B and C patients. These data suggest that the effects of the continuous instillation of local anesthetic might last significantly longer and remain efficacious, until the time of nephrostomy removal. Furthermore, no bounce back pain occurred beyond 24 hours after the surgery at the conclusion of the continuous infusion in Group A patients. At 2 and 6 hours after the surgery, Group A patients demanded significantly less amount of analgesics compared with Group B and C, while VAS scores, by contrast, were comparable between the groups, suggesting that the portable infusion device may also have some visual effects. In addition, no analgesic on demand was used in patients in Group A between 24 and 48 hours postoperatively, whereas a considerable amount of analgesic was used in Group B patients during the same time period (mean 12.5 ± 5.1 mg, Fig. 4). Thus, a reduced requirement for analgesics during the postoperative recovery period resulting from the efficacy of continuous local anesthetic instillation may ameliorate the various side effects that have been related to such drugs.
The major drawback of this study is that this study does not control for the possible placebo effect of having a portable infusion device for pain control. However, to the best of our knowledge, our present study is the first to evaluate the effects of continuous local anesthetic instillation at the nephrostomy site in the management of PCNL-related pain.
Although a single injection of local anesthetic may reduce pain after surgery, its major disadvantage is the absence of a long-lasting effect, so it may only have a role in pain management immediately after PCNL. Repeated local anesthetic injections during the recovery period may compensate this duration problem, but the repeated injection itself may cause pain and discomfort to the patients. However, the effects of our novel continuous instillation method lasted long enough to reduce the perceived pain of our patients until the time point when the nephrostomy tube was removed. Moreover, we could eliminate other confounding factors for pain perception, such as age and gender, because there were no statistically significant differences in the three groups for either the patient characteristics or operative parameters. Finally, we used a standard general anesthesia protocol for surgery in all of our current patients, which made it possible to perform an adequate comparison of different local anesthetic administration protocols and methods and to assess their effects on both postoperative pain and the amount of analgesic used.
Conclusion
The continuous instillation of a local anesthetic after PCNL yielded improved postoperative pain management and reduced overall level of analgesic use compared with the single injection of local anesthetic at the puncture site throughout the entire period with the nephrostomy tube. Our novel method may represent a promising approach to improving patient comfort and preventing side effects related to analgesic use in patients who undergo PCNL and requires nephrostomy tube postoperatively.
Footnotes
Acknowledgment
This study was supported by the Ewha Fresenius-Kabi, Inc.
Author Disclosure Statement
No competing financial interests exist.