
Abstract
Introduction:
Fibroepithelial polyps of the ureter are a rare cause of asymptomatic and symptomatic upper urinary tract obstruction in children. While these lesions can often be managed endoscopically, large or multifocal polyps may preclude such an approach.
Objective:
We aim to describe our institutional experience with robot-assisted laparoscopic treatment of ureteral polyps and show that a robotic approach is an effective alternative for large or multifocal polyps.
Materials and Methods:
Four children were identified with ureteral polyps over a 5-year period and underwent transperitoneal robot-assisted laparoscopic excision. Patients presented with flank pain and/or worsening hydronephrosis. All patients were evaluated preoperatively with ultrasound and Tc99m-mercaptoacetyltriglycine (MAG3) diuretic renogram or MR urogram. Retrograde pyelography corroborated the diagnosis of ureteral polyps. We reviewed the charts of these patients and compared the specific robotic approach for each patient, length of hospitalization, surgical complications, need for additional procedures, and resolution of symptoms and hydronephrosis.
Results:
In one patient, more than 20 polyps were identified over a long ureteral segment and all were excised; for the remaining three patients, 1 to 2 polyps were found. Mean postoperative length of stay was 1.5 days. One patient developed a ureteral stricture requiring repeat ureteroureterostomy, and another patient required repeat retrograde pyelography for gross hematuria that occurred several months after surgery. No polyps or obstruction was observed on retrograde pyelography in these patients. Mean duration of follow-up was 29 months (9–62 months). Symptoms and degree of hydronephrosis have improved in the three patients who have been followed for at least 12 months.
Conclusions:
Robot-assisted laparoscopy is a safe and feasible alternative to endoscopic treatment of fibroepithelial ureteral polyps. The robotic platform may be preferred in cases of multifocal or large ureteral polyps, or in cases in which a concomitant ureteropelvic junction narrowing may be present.
Introduction
F
Materials and Methods
Patients
As part of a prospective robotic surgery outcomes institutional review board approval, we retrospectively identified four patients who underwent robotic surgery for the management of FEPs for presumed UPJO between 2010 and 2015. In addition to renal ultrasound, patients were evaluated preoperatively with either Tc99m-mercaptoacetyltriglycine (MAG3) diuretic renogram or MR urogram to quantify renal drainage (Fig. 1). All patients had retrograde pyelography before robotic surgery to corroborate the suspicion of FEPs (Fig. 2), and the findings were confirmed once the ureter was opened to display the polyps. For the patient with numerous polyps, retrograde pyelography was performed during a separate anesthetic procedure; diagnostic ureteroscopy was also attempted but a large polyp precluded evaluation beyond the distal ureter. For the other patients, retrograde pyelography was performed during the same anesthetic immediately before robotic polyp treatment. Surgical pathology confirmed the diagnosis of

Nuclear diuretic renogram of patient 1 shows delayed drainage on the left side consistent with obstruction. Split renal function is 45% on the right and 55% on the left.
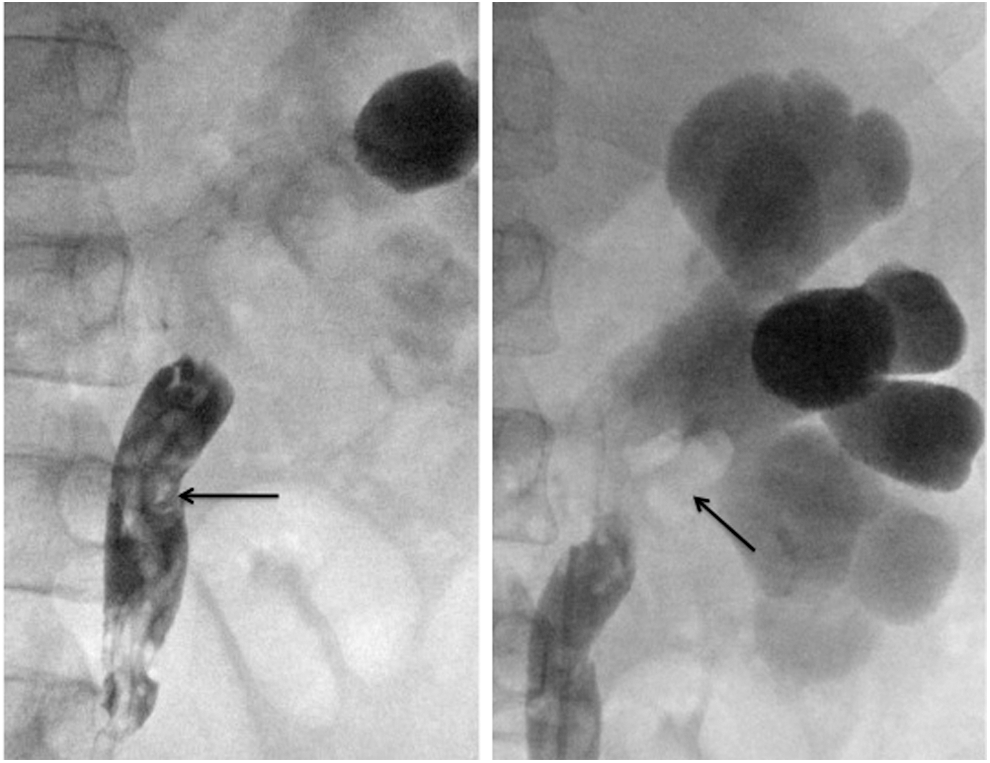
Retrograde pyelogram of patient 1 shows hydronephrosis and multiple ureteral filling defects (arrows) consistent with FEPs. FEP = fibroepithelial polyp.
Surgical procedures
After cystoscopy and retrograde pyelography, patients were then positioned in modified left flank position with arms at the sides. Peritoneal access at the umbilicus was achieved through an open laparoscopic approach through a natural fascial opening. An 8.5 mm camera port was placed through the umbilical access point. In addition, two 8 mm robotic ports were placed in the midline below the xiphoid and either in the midline suprapubic region or off the left iliac crest (all four cases were left sided). For two patients, a 5 mm assistant port was placed in the midline between the subxiphoid and umbilical ports (Fig. 3).
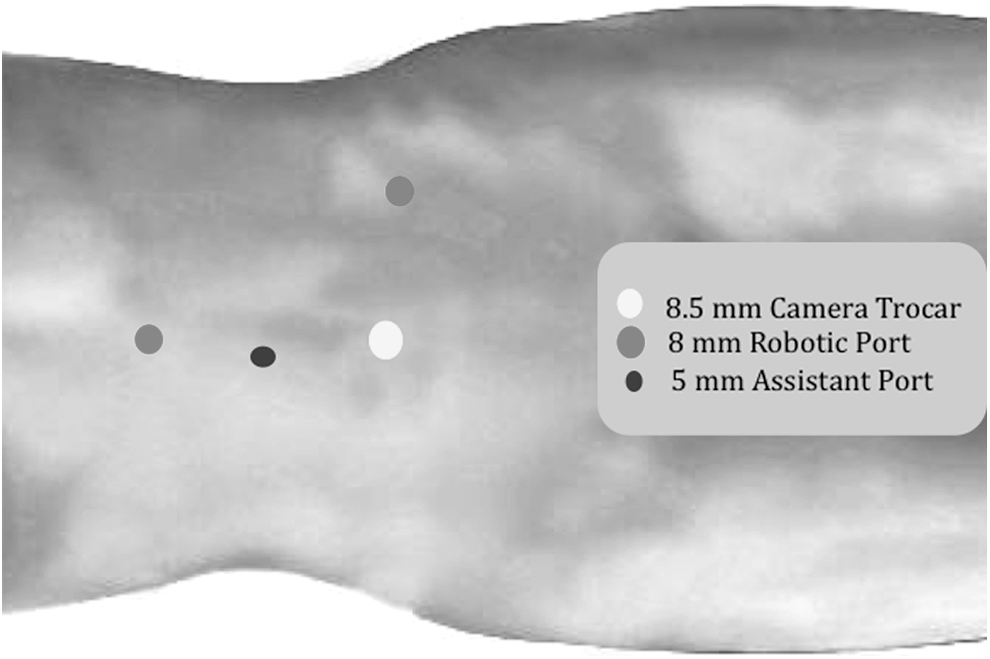
Patients are positioned in modified flank position and robotic and assistant ports are placed to optimize access to the ureter.
Due to the large number of polyps in patient 1, a modified approach was taken. The left colon was mobilized laparoscopically to expose the ureter. A ureterotomy was made at the ureteropelvic junction (UPJ) and exposed multiple finger-like polyps. A counter incision was then made more distally on the ureter at the pelvic brim to expose more polyps. The entire ureter was then opened between the two incisions. At least 20 polyps were excised using electrocautery. Intracorporeal ureteroscopy was performed using the subxiphoid robot port to ensure that the distal ureter and the renal pelvis were clear of additional polyps. The ureterotomy was then closed with 5-0 poliglecaprone 25 in a single running full-thickness manner over a double pigtail ureteral stent. The UPJ was then reconstructed with a flap pyeloplasty.
For the remaining patients, a transmesenteric window was created to identify a discrete narrowing in the ureter caused by the polyp. The ureter was transected at the point of maximal narrowing. The proximal and distal ends were spatulated, exposing the polyps. The polyps were excised with electrocautery in patients 2 and 3, and in patient 4, the polyp-containing ureteral segment was resected. The spatulated ends of the ureter were anastomosed using 6-0 GLYCOMER TM 631 over a double pigtail ureteral stent in patients 2 and 3. The ureteral stent was removed 4 to 8 weeks postoperatively. A stent-free anastomosis was performed in patient 4.
Results
All patients were male and ranged from 5 to 9 years old at the time of surgery (Table 1). Presentation included flank pain in three of four patients, and one patient had gross hematuria as well. Three patients had been previously followed with serial ultrasounds due to antenatal hydronephrosis, and one patient developed progressive hydronephrosis without pain. Interestingly, in patient 1, more than 20 polyps up to 5 cm in size were identified from the UPJ to the level of the pelvic brim (Fig. 4). Polyps at the UPJ were identified in two other patients and one patient had a mid-ureteral polyp. All patients were discharged from the hospital on postoperative day 1 or 2.
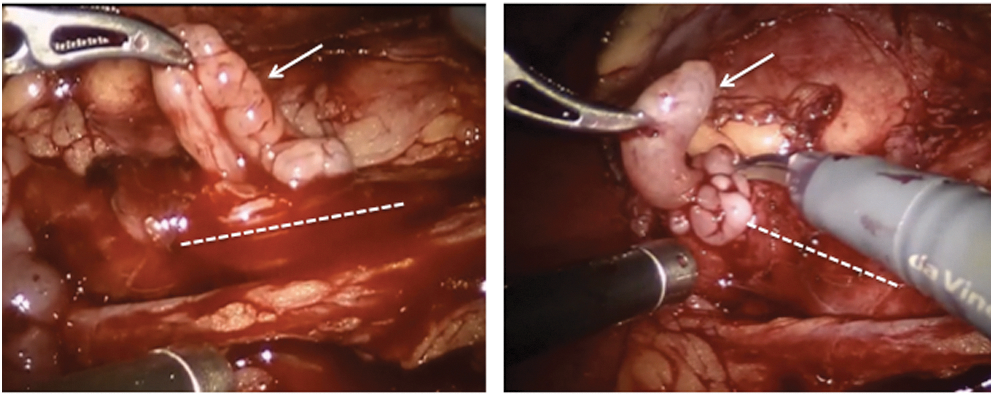
The ureter (dotted lines) is opened longitudinally and large polyps (arrows) are grasped before excision.
ANH = antenatal hydronephrosis; GH = gross hematuria; RPG = retrograde pyelogram; UPJ = ureteropelvic junction; URS = ureteroscopy; U-U = ureteroureterostomy.
Mean follow-up time was 29 months (9–62 months). One patient, in whom a stent-free anastomosis was performed, developed a ureteral anastomotic stricture and required nephrostomy tube placement followed by revision robotic ureteroureterostomy. One patient required additional cystoscopy and retrograde pyelography due to gross hematuria 8 months after polyp excision, but no cause was identified and the hematuria was self-limited. Another patient had a planned diagnostic ureteroscopy 2 months after initial surgery to evaluate the possibility of additional asymptomatic polyps, but none was identified. Flank pain resolved postoperatively in all patients, and hydronephrosis improved compared with preoperative imaging in patients with at least 12-month follow-up (Fig. 5). None of the patients has had a recurrence of ureteral polyps.

Preoperative renal ultrasound (left) shows SFU grade 3 hydronephrosis that is nearly resolved 7 months postoperatively (right).
Discussion
This study describes our single-institution experience with robot-assisted surgical management of ureteral polyps. We specifically highlight a case of a child with multiple polyps throughout the majority of the ureteral mucosa to underscore the benefits of the robotic platform in extreme presentations. The extent of his polyp disease is extremely rare in the literature and to our knowledge this is the first report of such a severe presentation being managed robotically.
FEPs of the ureter are rare, limiting the number of patients in this case series. However, with an average 29-month follow-up, all patients have had improvement of symptoms without polyp recurrence or worsening imaging findings. We intend to follow these children with biannual ultrasounds since there is sparse literature detailing the likelihood of recurrence in children with multiple polyps repaired robotically. Our experience suggests that robot-assisted ureteral polypectomy is a safe and feasible management strategy for multifocal or large ureteral polyps.
The majority of ureteral FEPs reported in the literature occur near the UPJ, which is where the majority of polyps presented in our patients. Ureteral polyps seem to occur with a 58% to 89% male predominance, and interestingly, 75% present on the left side.
7,8
In the current series, all patients were boys with left-sided polyps. Adey and colleagues reported their 35-year experience of
The etiology of FEPs is unknown. Recurrent infections, chronic irritation, nephrolithiasis, trauma, and immunologic disturbances have all been proposed. 10 However, it is curious that these lesions occur in otherwise healthy children and they tend to have a male and left-sided preference. Furthermore, in our series, 75% of the patients had antenatal hydronephrosis, suggesting a developmental etiology. It is possible that some of these children may have an antecedent mild UPJ obstruction, which creates turbulent urine flow and applies sheering on the urothelium that leads to inflammation, thus triggering the milieu to develop polyps. Other studies of children with FEPs did not report prenatal ultrasound findings.
Traditionally, FEPs have been managed with open surgery.
2
However, open surgical techniques may have led to overly aggressive treatment, as 49% of patients in one series received a nephroureterectomy. With advances in endoscopic technique over the past several decades, most cases of ureteral polyps can be managed with a minimally invasive approach.
4,5,11
–13
Childs and colleagues report their experience of managing
Large and/or multifocal polyps present a therapeutic dilemma, as ureteroscopic access may not provide sufficient exposure or visualization. For large polyps or those where the stalk base was difficult to reach by means of retrograde manner, Lam and colleagues have described endoscopic treatment through a percutaneous antegrade approach. 4 Laparoscopic treatment has also been advocated for FEPs that were too large or numerous to be managed endoscopically. In a series by Bian and colleagues, 12 of 13 patients with UPJ or upper ureteral FEPs were effectively treated with transperitoneal laparoscopy. 1 One patient with bilateral polyps required open conversion. Surgery was effective in all 13 patients in relieving symptoms and improving hydronephrosis with a mean follow-up of 16 months. Retroperitoneal laparoscopic polyp excision has also been effective in treating children in one case series of five children. 6 FEPs that have been incidentally discovered near the UPJ at the time of pyeloplasty have been effectively treated with robot-assisted laparoscopic polypectomy and pyeloplasty. 17,18 The present study expands the use of robotic excision for FEPs beyond the UPJ and highlights a specific benefit of the robotic approach when multifocal, large polyps are encountered and require a long spatulation of the majority of the ureteral wall.
Conclusions
Fibroepithelial ureteral polyps are a rare cause of upper urinary tract obstruction in children. The majority of FEPs tend to occur near the UPJ and mimic classic UPJO. The current series highlights a child with multiple FEPs throughout the ureter that were treated effectively with robot-assisted laparoscopic excision. While small and unifocal polyps may be managed endoscopically, robot-assisted laparoscopy serves as an alternative strategy for treatment of large or multifocal polyps, or for cases in which a concomitant narrow lumen at the polyp base may be present.
Footnotes
Acknowledgments
We acknowledge Carrie Wachob for video editing assistance and Jim Pridgeon for narration of the video that accompanies this article, first published online January 2016 in Videourology.
Author Disclosure Statement
No competing financial interests exist.