
Abstract
Introduction:
Kidney stone patients have lower health-related quality of life (HRQOL) than nonstone formers. Among active stone patients (those with stones), those with symptoms have lower HRQOL than those without. However, little is known about whether asymptomatic stones affect patients' HRQOL.
Methods:
A sample of asymptomatic stone formers was assembled by identifying patients who reported no symptoms on the disease-specific Wisconsin Stone Quality of Life (WiSQoL) questionnaire (n = 351). Of these, 107 were identified (M:F 61:46; 53 ± 17 years; BMI 29.5 ± 7.6). Patients were mostly recurrent (78%), and 42% thought they had stones at the time of the WiSQoL questionnaire. Patients' WisQoL responses were compared by self-reported stone status (yes/no), actual stone status (yes/no, corroborated from imaging and medical records), age, gender, and duration of stones.
Results:
Of patients reporting stones at the time of the questionnaire (42% of sample), 37 (82%) were correct about it. Of patients who reported not having stones (49% of sample), 29 (55%) were correct. WiSQoL results were lower (worse HRQOL) among patients with stones versus those without, regardless of whether they knew their actual stone status.
Conclusions:
Asymptomatic patients with current stones, whether they are aware of them or not, may have lower HRQOL. These results suggest that (a) some patients may not be fully aware of their stone-related symptoms or are better able to handle them than others, and (b) due to the potential impact on HRQOL, some patients may benefit from definitive knowledge of their stone status as this may inform decision-making for subsequent stone management.
Introduction
I
HRQOL is fluid and can change over time due to changes in a patient's health status. Tracking patients' HRQOL may help to better characterize the natural history of chronic conditions, and this could improve disease detection and help to identify patients who require more aggressive care. Patients' HRQOL can be useful in identifying and individualizing treatment, comparing the efficacy of different therapies and interventions, and measuring the impact of therapy on patients. Some suggest further that quality of life indicators may reveal variable biological responses to disease progression, treatments, and prospective survival. 6 Assessing patients' HRQOL may be especially useful in conditions with variable expression among patients and in those marked by recurrent exacerbations, variable periods of quiescence between exacerbations, and the life-long need for medical and/or dietary regimens.
Urolithiasis exerts unique symptoms and dysfunctions in patients. Our group and others have previously shown that patients with a history of kidney stones have lower HRQOL than nonstone formers at multiple points along the disease continuum. 7 –12 Moreover, among those with stones, symptomatic patients have lower HRQOL than asymptomatic patients. 13 However, whether or not patients with asymptomatic stones have decrements in HRQOL is not described. As HRQOL is affected not only by specific disease symptoms but also by other factors, we characterized HRQOL in asymptomatic patients with a history of stones. To assess this, we used the validated Wisconsin Stone Quality of Life (WiSQoL) questionnaire, a 28-item disease-specific regional survey instrument with a 5-point Likert scale for each item.
Patients and Methods
With institutional review board approval, 107 largely calcium-forming patients (M:F, 61:46) were identified from a larger cohort (n = 351) of patients as having no stone-related symptoms at the time they completed the WiSQoL questionnaire. 13 All patients provided written informed consent. Seventy-eight percent of the asymptomatic patients were recurrent stone formers, and most had both passed a stone(s) and/or required intervention (64% and 72%, respectively). These and other patient characteristics are described in further detail (Table 1). As part of the WiSQoL questionnaire, patients self-assessed their stone status (yes/no for current stones) at the time they completed it, and this self-assessment was compared to imaging studies, results of which were obtained from patients' medical records. A review of medical records to assess for stone passage and/or removal immediately before patients' completion of the WiSQoL questionnaire was also conducted. During analyses of WiSQoL scores, patients were stratified in multiple ways: (a) perception of stones versus no stones, (b) stones on imaging versus no stones on imaging, (c) age, (d) gender, and (e) duration of stone disease. Total HRQOL scores from the WiSQoL questionnaire and results of individual items on the WiSQoL questionnaire were evaluated. Statistical analysis included two-way Student's t-tests between groups for all comparisons. Differences were considered statistically significant if P ≤ 0.05.
Data show prevalence within the sample (%) or mean ± SD (range).
BMI = body mass index [kg (body weight)/m2 (height)].
Results
By design, all patients included in the analysis were asymptomatic as was self-reported on the WiSQoL questionnaires. Results of various imaging modalities, as available in patients' medical records, were used to confirm patients' stone status (71% KUB, 20% CT, and 5% ultrasonography). At the time of the WiSQoL questionnaire, nearly half of patients thought they did not have stones (49%), 42% thought they had stones, and 9% were not sure. Of patients who thought they did not have stones, 55% were correct when image results and medical records were reviewed. Of those who thought they had stones, 82% were correct.
Patients with stones on imaging, regardless of their perception of their stone status, were bothered more by urinary urgency than those with no stones on imaging (P = 0.022), significantly more anxious or nervous about the future (P = 0.027), and they tended to be more annoyed with their situation related to stones (P = 0.058). There was also a tendency in this group for more nausea (P = 0.078). Patients who thought they had stones, regardless of whether this was true on imaging, were bothered more by urinary frequency than those who thought they were stone free (P = 0.023) as well as those who were not sure of their stone status (P = 0.016). Age, gender, and duration of stone disease were not factors related to differences in HRQOL within this group of asymptomatic patients. Total WiSQoL scores were not statistically significantly different, while patients who thought they had stones, but actually did not, had the highest total scores (average 129 of 140 possible points), while those who thought they did not have stones, but actually did, had the lowest total scores (average 118 of 140 points) (Fig. 1). Whether this difference is clinically significant is not known at this time.
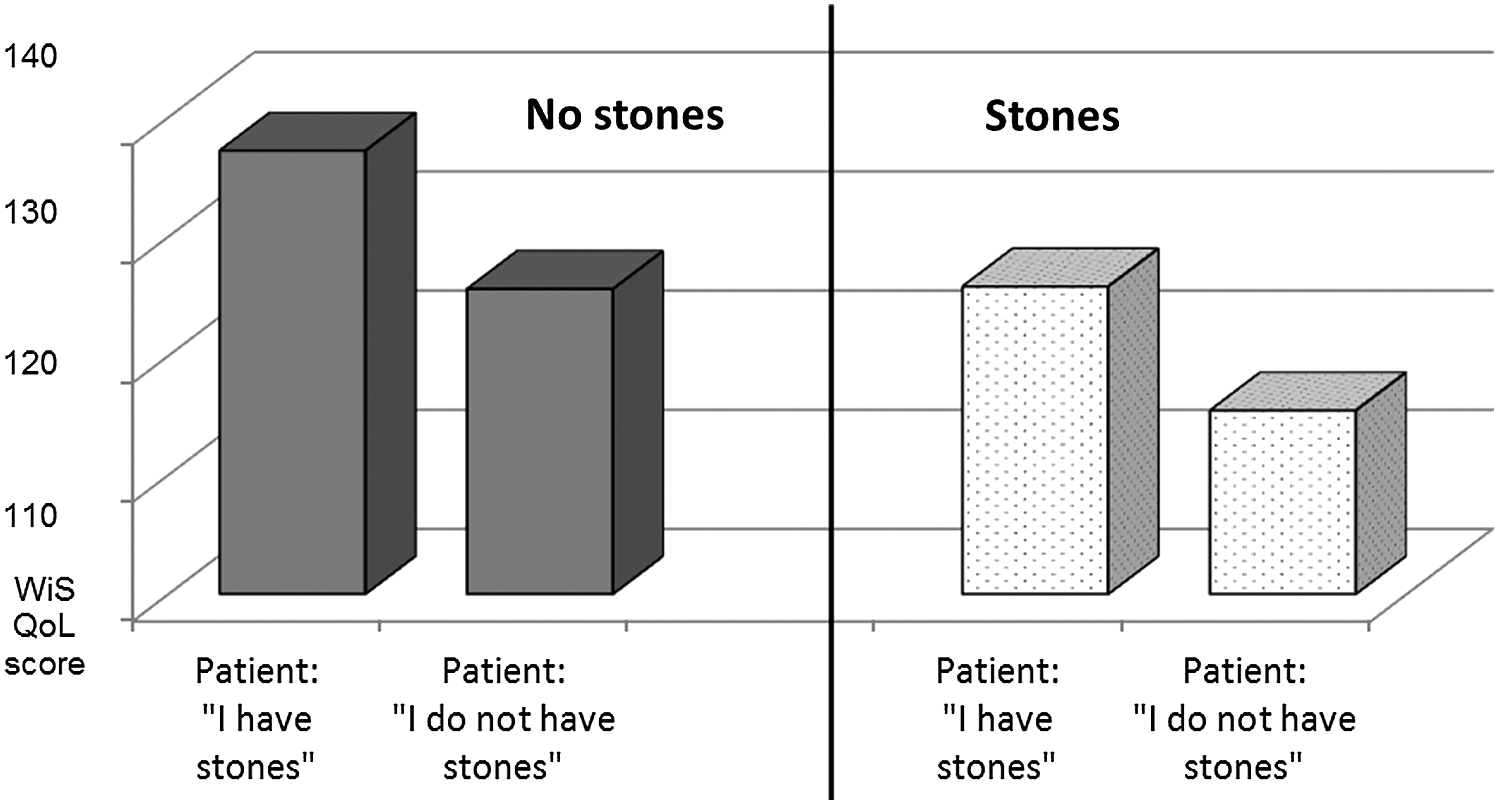
Total scores on the WiSQoL questionnaire from 107 patients with and without stones who self-reported as asymptomatic at the time they completed the questionnaire. The solid bars total WiSQoL scores for patients who did not actually have stones at the time of questionnaire completion; the dotted bars show total WiSQoL scores for patients who did have stones. The first pair of bars in each group represents patients who thought they had stones at the time they completed the questionnaire; the second pair of bars in each group represents patients who thought they were stone free. WiSQoL = Wisconsin Stone Quality of Life.
There was no difference in HRQOL scores in patients who were correct about their stone status versus those who were incorrect. Duration of stones and age were not associated with significant differences in item scores or total scores. Interestingly, while women scored lower than men for most items and for total score, none of these differences were significant. This is in contrast to symptomatic stone formers, results of which were previously reported, among whom women scored significantly lower than men on the WiSQoL questionnaires on most specific items and total HRQOL score. 13
Discussion
Results of our HRQOL study in asymptomatic stone formers reveal that patients reporting “no symptoms” related to stones may nonetheless have select HRQOL decrements. These include bother with urinary frequency, urinary urgency, anxiety or nervousness about the future (P < 0.027), and tendencies for greater annoyance with their situation (P = 0.058) and more nausea (P = 0.078). These differences were observed in patients who had stones and were aware of it, but also in those who were not aware of their presence. This suggests that the objective presence of stones, regardless of patients' perceptions, may lower HRQOL in some patients. Interestingly, even the perception of having stones–regardless of whether this was true–contributed to significantly more bother with urinary frequency than in patients who did not think they had stones. Finally, we note that patients scoring the highest on the WiSQoL (Fig. 1) questionnaire were those who thought they had stones, but actually did not. As an explanation for this, we hypothesize that without actual stones, the expected symptoms were absent resulting in less impact on patient HRQOL.
While estimates vary, approximately 50% of patients with asymptomatic stones progress to symptomatic within 5 years. 14,15 In addition, as many as one-third of asymptomatic patients will require emergent medical attention during this time, and a variable percentage of these will need surgical intervention. As further decrements in HRQOL would be expected in this patient cohort if and when symptoms do develop, the subset of asymptomatic patients with preexisting HRQOL decrements could progress to even lower HRQOL. This could be particularly devastating in patients with compromised health status (e.g., comorbid conditions, depression, frailty, infection, malnutrition) or in those in otherwise vulnerable situations (e.g., lower socioeconomic status, lack of social support systems, stressful work, or family situations). Indeed, Brown et al. assessed patient-reported parameters related to HRQOL and found that patients with chronic medical comorbidities and those functioning as primary caregivers scored lower. 16 By assessing HRQOL in patients reporting no stone-related symptoms, especially if they have current stones, prophylactic intervention could be considered.
It is logical that patients with stones, even though reporting no symptoms, have lower HRQOL as measured with the WiSQoL questionnaire. Prior studies using this instrument demonstrate that, indeed, patients with current stones have lower HRQOL than patients who do not have stones at the time of assessment. 13 The results from this study are thus understandable. Perhaps less clear is why the perception of having stones, even when not true, appears to associate with greater bother with urinary frequency (P ≤ 0.023 for difference from patients at the time of questionnaire completion who did not think they had stones or were not sure). This finding may suggest a weakness in the survey instrument or that a subset of patients might benefit from greater imaging frequency to inform them of their stone status. The latter is strengthened by the finding that asymptomatic patients who knew correctly that they had stones had higher HRQOL than those who were unaware of having stones (Fig. 1).
There is currently no clear consensus among urologists about how to manage patients with asymptomatic stones, but most visualize them. 17 Strategies for follow-up imaging among asymptomatic patients vary among providers as does the frequency of metabolic evaluation. We believe the routine assessment of patients' HRQOL in these situations may provide information about patients' expectations and preferences that can be used to make decisions regarding both follow-up and intervention. The results of our study and those of others who have investigated this topic underscore the importance of monitoring patients' HRQOL, even when they are “asymptomatic.” Clearly, the use of disease-specific instruments may prove helpful in this regard.
Next steps in this research trajectory include studies to (a) understand the role of comorbidities, socioeconomic status, and life situation/stress on the HRQOL of patients with stones, both symptomatic and asymptomatic; (b) identify the role of imaging and its frequency in maintaining suitably high HRQOL in asymptomatic patients; and (c) multi-institutional testing of patients' HRQOL using the WiSQoL questionnaires to assess its generalizability and clinical utility.
Limitations of our study include the relatively small number of patients. With a larger number of patients, it is highly likely that a greater number of differences on specific items in the WiSQoL questionnaire would be revealed. Also, the number of men versus women in our sample was skewed toward men. While the larger sample from which this subsample was obtained approached 50% men and 50% women, those reporting no symptoms on the WiSQoL (i.e., our sample) questionnaire were majority men. This could have influenced our results, especially as prior studies have shown that women may be affected more by their stones than men, at least in specific HRQOL areas. 8 And finally, the survey instrument itself may have undetected limitations.
Conclusions
Providers should increase their suspicion for the effects of even asymptomatic stones on patients' HRQOL and be prepared to offer proactive therapy for current stones in an effort to maintain and/or improve HRQOL. In addition, a subset of patients may benefit with respect to their HRQOL from definitive knowledge of their stone status.
Footnotes
Author Disclosure Statement
No competing financial interests exist.