
Abstract
Purpose:
We compare oncologic outcomes of minimally invasive and open nephrectomy for locally advanced kidney cancer.
Materials and Methods:
A retrospective review of a single-institutional, prospectively maintained database from a National Comprehensive Cancer Network-designated center was conducted. All patients who underwent radical nephrectomy at Roswell Park Cancer Institute with diagnosis of pT3 and pT4 renal-cell carcinoma (RCC) between years 1998 and 2015 were reviewed. Patients who underwent partial nephrectomy and nephroureterectomy were excluded.
Results:
We identified 172 patients with pT3 or pT4 tumors resected by minimally invasive (laparoscopic and robotic) or open radical nephrectomy. Demographic characteristics were similar between the two groups. Patients in the minimally invasive group had a higher mean body mass index (31.9 vs 28.1, p = 0.002), radiologically smaller tumors (7.7 cm vs 9.1 cm, p = 0.008), lower mean estimated blood loss (277 vs 1429, p < 0.001), lower rate of blood transfusion (4.7% vs 45.5%, p < 0.001), and a shorter mean length of stay (3.5 days vs 5.7 days, p < 0.001) compared with patients who underwent open surgery. At a median follow-up of 32.8 months, there was no significant difference in overall survival (p = 0.8) between the two groups.
Conclusion:
Minimal invasive nephrectomy is a safe approach with similar oncologic outcomes to open nephrectomy for select patients with locally advanced RCC.
Introduction
R
The present study aimed to determine the operative, postoperative, and oncologic outcomes of minimally invasive radical nephrectomy compared with open radical nephrectomy for locally advanced RCC performed in an NCI-designated Comprehensive Cancer Center.
Patients and Methods
Institutional Review Board approval was obtained for this study. A retrospective review of a single-institutional, prospectively maintained database from an NCI-designated center was conducted. All patients who underwent radical nephrectomy at Roswell Park Cancer Institute with diagnosis of pT3 and pT4 RCC between years 1998 and 2015 were identified. Patients who underwent partial nephrectomy and nephroureterectomy were excluded.
Preoperative patient characteristics, including gender, age at surgery, body mass index (BMI), RCC typical symptoms, Eastern Cooperative Oncology Group performance status (ECOG), nephrometry score (R.E.N.A.L. SCORE), radiographic tumor size and laterality, tumor stage and sites of metastases, were collected. Pathologic and serum variables were also collected and included preoperative and postoperative creatinine, pathologic tumor size, histology, margin status, adrenal involvement, node involvement, and the presence of lymphovascular invasion. Perioperative information was collected and included type of incision, surgery time, estimated blood loss (EBL), blood transfusion, and conversion from minimally invasive to open surgical approach. Intraoperative and postoperative complications were graded according to the Clavien–Dindo classification. Time to recurrence, metastasis, and mortality rate were used to calculate recurrence-free, metastasis-free, and overall survival (OS) rates.
Comparisons of patients’ characteristics were made using the Mann–Whitney U and Fisher's exact tests for continuous and categorical variables, respectively. The time-to-event outcomes were summarized by cohort using standard Kaplan–Meier methods, with estimates of the median and 1/3-year rate survival obtained with 95% confidence intervals. Comparisons were made using the log-rank test. OS was defined as the time from surgery until death (event) or last follow-up (censored). Recurrence-free survival was defined as the time from surgery until local recurrence (event) or last follow-up/death (censored). Metastasis-free survival was defined as the time from surgery until development of new metastatic disease (event) or last follow-up/death (censored). Progression-free survival (PFS) was defined as the time from surgery until disease progression (event—death, local recurrence, or new metastatic disease) or last follow-up (censored).
All analyses were conducted in SAS v9.4 (Cary, NC) at a significance level of 0.05; therefore, p-values less than 0.05 denote statistically significant results.
Results
We identified 172 patients with pT3 and pT4 RCC tumors who underwent minimal invasive (laparoscopic and robotic) or open radical nephrectomy. Sixty-seven patients underwent MIS (18 and 49 patients underwent robotic and laparoscopic approach, respectively) and 105 patients underwent open surgery. Both groups had similar demographic characteristics, including ECOG 0 or 1 in all cases. Nephrometry score was similar between the two groups (9.52 vs 9.58, p = 0.66). Patients in the MIS group had a higher mean BMI (31.9 vs 28.1, p = 0.002) and radiologically smaller tumors (7.7 cm vs 9.1 cm, p = 0.008) compared with patients who underwent open surgery (Table 1).
MIS = minimally invasive surgery; BMI = Body Mass Index; ECOG = Eastern Cooperative Oncology Group.
Compared with open surgery, patients in the MIS cohort had a lower mean EBL (277 vs 1423, p < 0.001), lower mean rate of blood transfusions (4.7% vs 45.5%, p < 0.001), longer mean operative time (294 minutes vs 273 minutes, p = 0.013) and mean surgical time (231 minutes vs 213 minutes, p = 0.033), and shorter mean length of stay (3.5 days vs 5.7 days, p < 0.001). There was a trend toward more complications in the open surgery group, but this difference was not statistically significant (37.1% vs 23.9%, p = 0.093). There was no difference in high-grade complications (Clavien–Dindo III-V, 37.5% vs 28.2%, p = 0.53) (Table 2).
EBL = estimated blood loss; LOS = length of stay.
The two groups had similar postoperative pathologic characteristics (Table 3), with the exception of a significantly lower rate of lymphovascular invasion (64.5% vs 88.2%, p = 0.001) in the MIS group compared with the open surgery group. In the MIS group, laparoscopic and robotic surgery had similar characteristics, except for lower mean EBL, and radiologically and pathologically smaller tumors on the robotic surgery group (Supplementary Table S1; Supplementary Data are available online at
LVI = lymphovascular invasion.
Table 4 summarizes the 3- and 5-year survival outcomes. Median follow-up for all patients was 32.8 months. There were no significant differences in OS (p = 0.8), freedom from local recurrence (p = 0.9), freedom from new metastatic disease (p = 0.1), or PFS (p = 0.5) between the MIS and open surgery groups (Fig. 1).
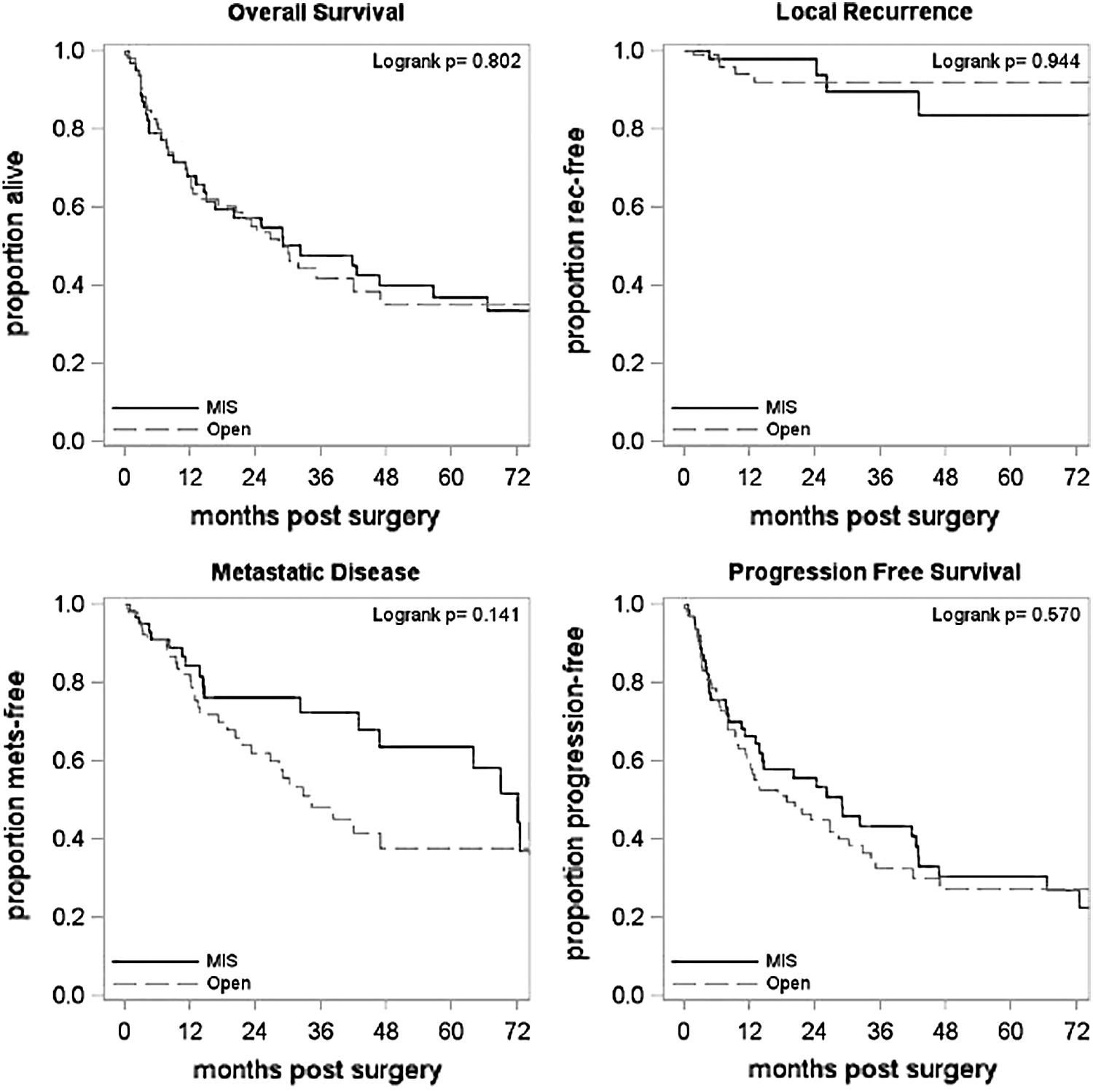
Overall survival, recurrence free-survival, metastatic free-survival, progression free-survival.
CI = confidence interval.
On multivariable analysis, there was no difference in any variable analyzed between the MIS group and open surgery group (Table 5).
HR = heart rate.
Discussion
The present study has shown that with an intermediate duration of postoperative follow-up of 33 months, MIS for locally advanced RCC achieves similar oncologic outcomes to those of open surgery, without differences in OS or freedom from local recurrence, metastasis, or any progression. MIS was associated with better perioperative outcomes in terms of EBL, rate of transfusions, and length of hospitalization. However, patients selected to undergo MIS had less bulky disease, which may have contributed to better oncologic and perioperative outcomes.
Since the first description of laparoscopic nephrectomy by Clayman, 13 the technique has evolved and surgeons have been gaining more experience. 3,9 Recently, complex open and laparoscopic cases have been performed with the robotic platform. 7,11,14 The utilization of these minimally invasive techniques has increased over time, with MIS radical nephrectomy now accounting for 61% of all RN procedures. 15 Several studies have demonstrated the advantages of MIS over open nephrectomy for pT1 and pT2 kidney tumors in terms of decreased blood loss, analgesia, length of stay, and convalescence, with similar oncologic outcomes, including long term. 3 –6,16 Nevertheless, the utilization of MIS for pT3-4 RCC has not been reported consistently and few studies have compared it with the open approach. 8,10
Bensalah and colleagues performed a matched comparison of 44 and 135 patients, who underwent laparoscopic and open nephrectomy for nonmetastatic pT3 RCC, respectively. They evaluated the survival of both groups and did not find any difference in oncologic outcomes, although the study was limited in that the open surgery group had a significantly longer follow-up (55 months vs 28 months, p < 0.001). 8 More recently, Laird and colleagues analyzed matched cohorts of 25 laparoscopic and 25 open nephrectomies for pT3 RCC patients. They did not find any difference in preoperative characteristics, mean operative time, or complications between the two groups, but there was a significant difference in mean EBL (100 cc for laparoscopic surgery vs 650 cc for open surgery; p < 0.001) and length of hospitalization (4 days for laparoscopic surgery, 9 days for open surgery; p < 0.001) in favor of the laparoscopic group. There was no significant difference on OS (85.9 months for laparoscopic surgery, 74.9 months for open surgery; p = 0.36) after a median follow-up of 54.6 months. 10 Similarly, after a median follow-up of 32.8 months, we did not find any difference between the MIS group and open surgery group in OS (32.2 months for MIS, 28.4 months for open surgery; p = 0.80). We found a lower EBL and shorter length of hospitalization within the MIS group, however, contrary to Laird and colleagues, 10 the operative time was slightly higher in the MIS group than the open group (294 minutes vs 273.1 minutes, p = 0.013). Nine (13.4%) MIS patients were converted to open due to invasion of adjacent organs and/or bleeding.
In summary, our study supports feasibility along with acceptable perioperative and oncologic outcomes of MIS nephrectomy for locally advanced RCC, consistent with several prior reports. 8 –10,17 However, our study is not exempt of limitations, which include the retrospective nature of the study and its related biases, and multiple surgeons with different experiences may affect outcomes. In addition, we investigated pathologic instead of clinical staged RCC, and precise criteria for selection of patients to MIS or open surgery could not be defined in this study.
Conclusion
Minimal invasive nephrectomy is a safe approach with similar oncologic outcomes to open nephrectomy in select patients with locally advanced RCC. Lower EBL, transfusion rate, and shorter length of hospitalization were shown to be more prevalent within the MIS cohort. Prospective randomized trials with a larger number of cases and longer follow-up are necessary to confirm our results.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.