
Abstract
Introduction:
Urinary stone disease is a common and often recurrent condition that can affect kidney function and requires a range of medical and surgical treatments, all of which can have a significant impact on patients' health-related quality of life (HRQoL) and treatment preferences.
Objective:
To review the literature systematically for all studies that include HRQoL measurement or patient preferences in the context of urinary stone disease.
Methods:
Ovid MEDLINE(R), Ovid MEDLINE(R) In-Process, EMBASE, SCOPUS, EconLit, and Web of Science were searched from inception to January 2016. All study designs with adult participants were included. Narrative synthesis was performed.
Results:
Thirty-five studies met the inclusion criteria (six randomized controlled trials and 29 observational studies) from 15 countries, including 5472 patients. Eleven studies showed that stone formers had worse HRQoL than the general population; it was noted that stone formers were more likely to suffer from depression. Women have significantly lower HRQoL than men. Twenty-six studies used a generic HRQoL measure and six were nonvalidated disease specific. Studies concerning patient preference were heterogeneous and showed that extracorporeal shock wave lithotripsy is still favored above other interventions and that a large number of patients would prefer the treatment pathway to be decided upon by their clinician.
Conclusion:
Urinary calculi and its treatment can have significant negative patient impact and influence patient preferences. Patients with stone disease tend to have worse physical and mental HRQoL, quantified using generic measures. Structured research with disease-specific measures underpinned by sound methodology would be beneficial and aid in development of patient-centric management.
Systematic Review Registration:
This review was prospectively registered with the international prospective register of systematic reviews–PROSPERO 2013:CRD42013006084.
Introduction
Disease and treatment
U
When presentation is with acute colic, treatment of urinary stone disease involves control of pain, infection, and, if present, obstruction on an emergency basis. After the acute phase, further hospital visits/admissions for definitive medical treatments and therapeutic interventions are often needed. The overall patient journey can be long, multistep, and varies depending on treatment options and choices. Stone disease and its treatment affect patients' health and may have a significant negative impact on their health-related quality of life (HRQoL).
The European Association of Urology (EAU) and American Urological Association (AUA) guidelines state that patients with large stones or significant obstruction and those who fail to respond to expectant treatment require interventional treatment. Extracorporeal shock wave lithotripsy (SWL) and ureteroscopy (URS) are two most common competing interventional treatment options for ureteral or renal stones. Percutaneous nephrolithotomy (PCNL) and additional treatments are generally reserved for large renal stones. 4 The treatments can offer equivalent clinical outcomes, but involve different pathways and risks. When considering patient preferences, outcomes, and resource efficiency, it is unclear if the current pathway of care is optimal. It is possible that some aspects of treatment could be changed and traded if patient impact and perspectives could be better understood.
Patient-reported outcome measures
The goals of modern surgery have been to treat pathology and restore normal anatomy and physiology, and therefore the goal of the stone surgeon has been to render the patient stone free. In recent years, it has become apparent that this is not always possible or necessarily the only important consideration. 5 Similarly, assessment of disease impact on patients is likely to be important and can guide treatment decisions. All treatments have their inherent risk and complications, and quality of life may be more important to many patients than achieving a radiological stone-free status alone. 6
Patient-reported outcome measures aim to measure patient's perspective of illness, health, and interventions in a valid reproducible way. Generic HRQoL measures have been developed and validated, such as the short-form 36 questionnaire (SF-36) and EuroQol 5 dimension (EQ-5D), and are used widely. Many specialty, disease, and procedure-specific measures have also been developed and validated, such as the EORTC QLQ-C30 and the Oxford Hip Score, and have been taken up into general use with varied effects. 7 –9 Attempts have been made to measure the disease and intervention impact in the field of urinary calculi as part of clinical studies. 6,10
Worldwide practices across different hospitals that incorporate patient preference vary significantly. Similarly, the impact of various treatments on patients' HRQoL, utilities, and preferences has not been examined and this is important in the context of clinical equipoise between treatment modalities. 11,12 Patients' expectations of treatment and the impact of disease on HRQoL, as well as changes to it due to treatments, would be important outcome parameters.
The aim of this study was to review systematically the available evidence regarding quality of life of adult patients with urolithiasis and how that might have influenced their treatment choice.
Methods
Design
A systematic review of the evidence regarding quality of life and patient preferences in urinary stone disease was conducted in accordance with the principles outlined in the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines and the Cochrane Handbook of Systematic Reviews. The review was prospectively registered with the international prospective register of systematic reviews (PROSPERO 2013:CRD42013006084) to increase transparency and to avoid duplication of work.
Search strategy
A search strategy was developed in Ovid Medline, using Medical Subjecting Headings as well as free text and controlled vocabulary built around the research question (Table 1). The Medline search strategy was modified to use in the rest of the databases. The databases searched were Ovid MEDLINE(R) 1946 to present, Ovid MEDLINE(R), In-Process, and Other Nonindexed Citations, EMBASE 1947 to present, SCOPUS, EconLit, and Web of Science 1900 to present with no language restriction. All databases were searched up until January 2016. Autoalerts were set up for databases that allowed them. The records were imported into Endnote X7 and duplicates were removed. Two independent reviewers examined the titles/abstracts and irrelevant articles were discarded.
Throughout the process, any disagreement was resolved by discussion and, if needed, a third impartial reviewer. The articles that remained were subject to a citation search and a hand search of references was performed.
Inclusion and exclusion criteria
Types of study designs included all relevant, published, randomized controlled trials (RCTs) and nonrandomized studies, as well as prospective observational studies with controls, retrospective studies, and comparative studies. Study populations were limited to adults (18 years old and above) with urinary stones or history of urinary calculi in primary, secondary, and tertiary care. Studies that examined patients with stones in the kidney, ureter, or both and that examined patients with stones of all sizes were included. Studies that made reference to ureteral stents without urinary stone disease were excluded.
Critical appraisal of the evidence
Two independent authors assessed all studies that met the inclusion criteria for quality. Observational studies were classified as being at a high, low, or of unclear quality, using the strengthening the reporting of observational studies in epidemiology (STROBE) checklist as guidance. 13 RCTs were assessed for quality using the Critical Appraisal Skills Program (CASP) RCT checklist and Jadad scale. 14 Measures of quality included appropriateness of study design, quality of reporting, and generalizability. Any disagreements were resolved by consensus or, if needed, adjudicated by a third impartial reviewer.
Data extraction and synthesis
Copies of all articles identified as being of potential importance were obtained and authors were contacted if necessary. Data extraction was performed by two independent reviewers using a bespoke data extraction form, designed specifically for this task. Data from articles were extracted into a Microsoft Excel spreadsheet.
Results
Evidence synthesis
A total of 3946 records were identified through database searching. Checking the reference lists of the articles identified four additional records. Duplicates were removed and finally 55 abstracts were assessed (16 poster abstracts and 39 full-text articles). Four articles were found to be without demographic data and requests for this information were sent to lead authors. No replies were received and they were therefore excluded. Of these 51 articles, 35 fulfilled the inclusion criteria after they were assessed for eligibility (six RCTs and 29 observational studies). The 16 articles that were not analyzed were excluded due to lack of appropriate data, article not being in English, or inclusion of pediatric patients with the adult population (see Figure 1). The studies included originated from 15 countries and involved 5472 patients.
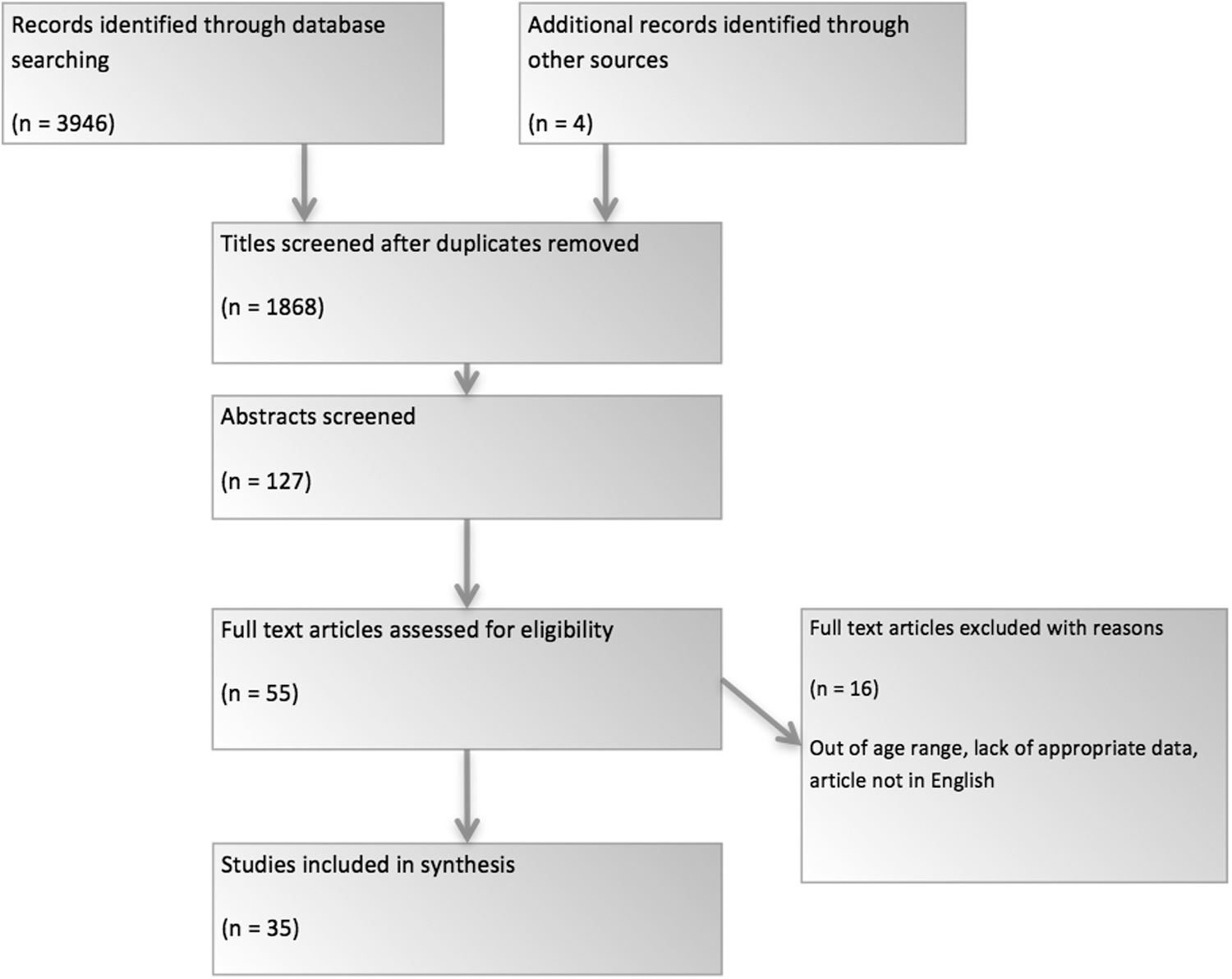
Standard flow diagram (adapted from PRISMA): summary of evidence search and collection. PRISMA, preferred reporting items for systematic reviews and meta-analyses.
Six RCTs were included, but their data could not be collated for meta-analysis due to their heterogeneity of both variables and outcomes. Dellabella and colleagues described tamsulosin vs tamsulosin plus steroid with regard to stone expulsion time and HRQoL. Pearle and colleagues compared SWL with URS for lower pole caliceal stones with regard to stone clearance rate and HRQoL. Eryildirim and colleagues in 2015 compared patients taking analgesia alone with patients taking analgesia and tamsulosin. In 2001, Keely and colleagues compared the HRQoL of patients undergoing SWL with those being observed only for renal stones. Lee and colleagues compared medical expulsive therapy (tamsulosin) with no treatment for proximal ureteral stones. Stone passage time and HRQoL were compared. 15 –20 Finally, in a large, multicenter double-blind RCT, Pickard and colleagues compared tamsulosin, nifedipine, and a placebo. They found no difference in HRQoL between any of the groups at 4 or 12 weeks and no difference between rates of stone passage at 4 weeks. 21 Due to the heterogeneity of the methods employed, process or intervention being measured, and lack of raw figures, domain data from these studies could not be pooled.
Summary of studies
Thirty-five studies were included in the narrative synthesis. The studies were split into two groups; those concerning HRQoL and those relating to patient preference. The HRQoL groups were divided into studies that include interventions (medical/surgical) and those that did not. The intervention group was further subdivided into groups based on stone site—ureteral, renal, or both (Tables 2 –5).
BMI = body mass index; ER = emergency room; HRQoL = health-related quality of life; MCS = mental component score; PCNL = percutaneous nephrolithotomy; PROM = patient-reported outcome measure; QoL = quality of life; SF-36 = short-form 36 questionnaire; SWL = extracorporeal shockwave lithotripsy; URS = ureteroscopy.
ED = emergency department; EQ-5D = EuroQol 5 dimension; MET = medical expulsive therapy; RCT = randomized controlled trial; VAS = visual analogue scale.
OBS = observation.
SD = standard deviation.
HRQoL studies
Most studies use radiological clearance of stones as the primary outcome for research into the treatment of urinary stones. Five studies state that in the modern era of patient-centered care, HRQoL must be considered as an important outcome. 6,22 –24 Generic HRQoL tools have been used for this purpose up until now. The SF-36 was used as a measure in 16 studies. Other validated measures of HRQoL used by researchers include SF8, EQ-5D, LifeScale, Perceived Stress Scale, CUES-D depression questionnaire, and the Nottingham Health Profile. 6,15,17 –19,25 –30 Seven studies used nonvalidated measures or questionnaires either in isolation or in conjunction with validated generic questionnaires. 27 –29,31
Results from the studies using the SF-36 revealed that general health physical function, role limitations due to physical health problems, bodily pain, general health perception, and social function were main domains that were affected. Additional questionnaires revealed that trouble looking after the home, lower urinary tract symptoms, and sleep disturbance were also affected, but not evaluated by the SF-36. Six studies showed that stone formers had worse HRQoL than the general population or controls. 22,23,25,32,33 Two studies showed this to be true for those without active stone disease and one showed that patients with stone disease were more likely to suffer from depression. 25,33
Women tended to have statistically lower HRQoL than men. 34 Greater medical comorbidity (including being obese, increasing age, suffering from diabetes, hypertension, and musculoskeletal complaints) resulted in worse reported HRQoL than fitter patients. 22,23,29,35 Diniz and colleagues reported that stone patients in lower socioeconomic groups had lower HRQoL. 33
Bryant, Angell, and Penniston reported that stone formers and/or those undergoing treatment for stone disease were more likely to suffer from depression, have more stressful life events, and have lower emotional HRQoL. Angell also stated that those suffering with one or more complications after stone surgery were statistically more likely to be depressed. 22,23,25,32,35,36 It was also noted that the greater the number of stone events requiring medical consultation, the lower the HRQoL score. 23,35
Three studies found problems with using generic HRQoL measures for patients with urinary stone disease and six concluded that a disease-specific HRQoL measure for patients with urinary stones is needed. 22 –24,27,35
Studies with no intervention
Modersitzki and colleagues reported lower HRQoL in American patients with cystinuria compared with noncystinuria patients in all domains except emotional role. 35 They found that temporal proximity to the last stone event and greater frequency of stone events per year decreased HRQoL. Diniz and colleagues described a Brazilian patient population with recurrent urinary stone disease in an intercrisis period. 33 These patients had lower HRQoL across all domains of the SF-36 compared with controls.
Donnally and colleagues reported that in an American patient population with urinary stone disease, patients who did not experience any stone episodes in the month before completing the SF-36, did not have any significant difference in HRQoL compared with controls. 24
Penniston and Nakada reported lower general health and bodily pain scores for American patients with urinary stone disease compared with the healthy American population. Women reported lower scores than men. 34 Bryant and colleagues reported that compared with the general American population, American stone formers suffered with lower SF-36 scores in six of the eight domains (including physical function, role limitations due to physical health problems, bodily pain, general health perception, vitality, and social function). 16,22 –24,32,33,35 –37
Studies with intervention for ureteral stones
Izamin and colleagues reported significant differences in mental component (MCS) and physical component (PCS) scores before and after treatment for ureteral stones in those undergoing treatment (SWL or URS) in a Malaysian patient group compared with the control population. However, there was no significant difference in scores between those undergoing either treatment. 38 Rabah showed that in their Saudi population, those undergoing SWL suffered with statistically significant lower SF-36 scores in the physical functioning, social functioning, and bodily pain domains. 39
Studies with intervention for renal stones
Deem and colleagues reported similar results to Rabah in an American cohort undergoing either SWL or PCNL for renal stones, with all patients reporting improved PCS, but no difference in MCS. This improvement was statistically significant in patients who had undergone PCNL at 3 months, whereas those who had undergone SWL showed no significant difference. Two articles by Sahin and colleagues in 2014 and 2015 showed that larger residual fragments after SWL caused worse HRQoL. 40,41 Staios and colleagues saw a statistically significant improvement after treatment in the mental health and emotional role domains in British patients who had undergone PCNL for lower pole stones. 42 Pérez-Fentes and colleagues studied patients undergoing PCNL and compared preoperative HRQoL with HRQoL at 3 and 12 months. 43 They found that patients' HRQoL was better after 3 months and that perceived benefit continued up to a year.
Studies with interventions for both renal and ureteral stones combined
Arafa and Rabah described better HRQoL scores for Saudi patients after SWL compared with healthy controls a few months after treatment in all domains except bodily pain and general health. 32 Interestingly, Kurahashi and colleagues reported that there was no significant difference in Japanese patients who had undergone SWL and healthy Japanese people. 37
Studies of patients with lower pole stones by Pearle and all urinary stones by Arafa showed that those undergoing SWL were more likely to get back to a normal routine more quickly (this included returning to work) than those undergoing other interventions; however, Mays and colleagues reported the converse and Karlsen and colleagues reported no significant difference in patients with proximal ureteral stones. Karlsen and colleagues also reported no difference in the number of patients who claimed that their social life was affected and no difference between patients' satisfaction with treatment, but SWL was generally preferred to URS due to fewer postoperative symptoms. 16,27,30,32
Studies evaluating patient preference
Studies regarding patient preference were heterogeneous in nature and were subdivided into those that asked patients about intervention and those that did not.
Noninterventional patient preference studies
Bensalah reported in 2009 that of the urologists questioned, most thought that patients would tolerate one or two stone episodes a year to avoid long-term medication; however, 81% of patients stated they would prefer long-term medication than suffer any more stone episodes.
One study showed that educating patients before treatment tended to decrease anxiety associated with the treatment. 26 Tiselius showed in 2006 that almost all patients were motivated (in theory) to change dietary and drinking habits to decrease the chance of a further stone episode, but only 81% felt that a regular follow-up program was useful. Interestingly, only 76% were interested in prevention of further episodes if it were to cost them money. 44
Interventional patient preference studies
In two studies, patients were asked to rank treatment options from most to least desirable and, in both studies, the order was SWL, URS, and PCNL. 29 Sarkissian and colleagues reported that 56.4% of patients would defer treatment choice to their urologist. 31 It was also shown in two studies that those who have undergone a particular intervention would be most likely to choose that intervention again in the future and that past stone experience affects treatment. 27,31
Discussion
The primary goal of treatment for urinary stone disease has been to achieve the highest radiological stone-free rate. Better HRQoL has been a secondary outcome if considered at all. However, in the era of holistic medicine, greater patient-centric care has become the focus of treatment. As the importance of HRQoL grows, so does the desire to quantify it to measure something that was thought to be immeasurable in the past. 45
Until recently, HRQoL in urinary stone disease has been gauged by and large by generic measures such as the Nottingham Health Profile in the past and the SF-36 and EQ-5D EuroQol questionnaires in more recent years. Most studies showed that patients with urinary stone disease have lower HRQoL than the reference population. Studies have also shown a relationship between HRQoL and the burden of comorbidities, as well as socioeconomic status. The few studies that evaluated patient preference were heterogeneous. SWL seemed to be preferable to other interventional options when surgical treatments were considered. More than half of patients would choose to follow their surgeon's choice of treatment.
The idea that patients with active urinary stone disease tend to have worse HRQoL than those without makes sense, but all authors except Donnally found that even between episodes, HRQoL was worse in both the physical and mental health domains. This suggests two things. First, even between acute episodes, stone patients suffer with physical symptoms greater than that of the reference population. Second, stone patients always have their stone symptoms borne in mind either on a conscious or subconscious level and this in turn affects their emotional well-being. Decreased HRQoL has been noted in other chronic diseases such as diabetes and chronic renal failure. 46,47 Greater education empowers patients and allows them to feel more in control of their disease and this may help increase HRQoL in the long term. 48
Most patients surveyed appeared to have poorer HRQoL during and immediately after treatment, but at the time of follow-up (most often at 3 months), patient's HRQoL was improved. One study measured HRQoL at 12 months after the procedure and the improvement was maintained. It would be interesting to know whether that improvement was maintained at 3 or 4 years, when new stones may be appearing and need treatment. Better HRQoL following SWL, compared with controls, shown in the study by Arafa and colleagues could be due to SWL patients being more aware of their bodies and appreciation of good health or by virtue of a response shift, which involves a change in internal values and standards following illness.
With regard to return to work after interventional treatment, reports were varied and no consensus reached. This is an important point because patients tend to suffer with stone episodes in the most productive years of their life and may be the main breadwinners of the household. Decreasing the length and severity of stone episodes may help both the patient and the wider economy.
An interesting point raised by Bensalah and colleagues is the disparity between patients' and urologists' view of acceptability of treatment. A vast majority of patients did state that they would prefer long-term medication to experiencing any stone episode in the future, and a majority of urologists thought their patients would prefer to experience one or two stone episodes a year to avoid long-term medication. This may be explained, in part, by the fact that although patients would initially like long-term prophylactic treatment, long-term compliance tends to be poor and this can be predicted by the experienced clinician. 49
Studies regarding patient treatment preference were heterogeneous, and being such a small number of articles, it is difficult to draw firm conclusions from them. Patients tend to prefer SWL to other interventional treatments because it carries a lesser burden of postprocedural symptoms. More than half patients said they would follow their surgeon's advice with treatment choice. It was unclear if these patients were significantly different from the rest of the study population. These patients may represent an older more deferential subset of patients who feel that the doctor is the expert and they do not feel comfortable making a choice about their own healthcare. 50 Patients also seemed to prefer to have treatments they have already undergone in the past. Any procedure carries risk and risk of the unknown. A false sense of security may exist in the minds of patients who have undergone a certain treatment with no harm done to them. They may feel that the procedure is safer than the alternatives because no harm came to them last time, even though the true level of risk might be different. Greater patient education and empowerment may negate these effects.
The results of this review highlight the importance of HRQoL in patients with urinary stone disease and the need of good quality evidence to improve patient care. The journey experience of patients with stone disease has not been fully explored and these results highlight the lack of standardized and valid disease-specific HRQoL measures. The task of creating an HRQoL measure for urinary stone disease has been challenging due to wide variation of patient experience and symptoms, coupled with the HRQoL impact of the treatments offered.
Little work has been done with regard to patient preference of treatment. This is surprising as the current EAU and AUA Guidelines suggest that patients with ureteral or renal stones as much as 20 mm can be offered SWL or URS as first-line interventional treatment and SWL or URS as first- or second-line treatment for ureteral stones of any size. 51 We found that a significant proportion of patients were likely to choose an intervention they had already received or to defer the decision to their urologist.
None of the studies evaluated the impact of patients' disease and management on patients' family members. Due to the chronic nature of the condition, this is an important aspect to consider in the wider psychosocial context as medical decision-making is often an amalgamation of the ideas, concerns, and expectations of the patients and their confidants, who are often close members of the family. 52 Similarly, many other aspects of stone disease and its treatments that could alter current treatment pathways need to be studied. Detailed economic health service research in this area could aid in development of patient-centric treatments.
Our review has limitations. We excluded non-English language articles and studies published only as abstracts. We could not use graphical or statistical methods to assess for publication bias because of the paucity of evidence, and we did not identify any unpublished randomized trials that met our inclusion criteria.
Conclusion
Our study has shown that both urinary stone disease and its treatments have short- and long-term impacts on patient's HRQoL, affecting a wide variety of domains. This is likely to have influence on patients' treatment choices. This has been objectively demonstrated with the use of generic valid and unvalidated measures. The results highlight the importance of the creation of sound, standardized, patient-reported outcome measures as the currently used generic tools were found to be lacking. Further research in this area would aid in better patient-centric care.
Footnotes
Acknowledgments
The authors would like to thank Mala Mann (MCLIP) from Specialist Unit for Review Evidence (SURE), Cardiff University, for her advice on systematic review methodology and assistance with designing the search strategy and Prof. Sam Salek from Cardiff University for his support. No funding was sought to undertake this review.
Declarations
The corresponding author has the right to grant on behalf of all authors and does grant on behalf of all authors a worldwide license to the Publishers and its licensees in perpetuity, in all forms, formats, and media (whether known now or created in the future), to i) publish, reproduce, distribute, display, and store the Contribution; ii) translate the Contribution into other languages, create adaptations, reprints, include within collections, and create summaries, extracts, and/or abstracts of the Contribution; iii) create any other derivative work(s) based on the Contribution; iv) to exploit all subsidiary rights in the Contribution; v) the inclusion of electronic links from the Contribution to third-party material wherever it may be located; and vi) license any third party to do any or all of the above.
Hrishi Joshi affirms that this article is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained.
Authors' Contributions
A.R.—First reviewer, created search strategy and data extraction form, wrote first draft of manuscript, and created tables and figures. Z.H.—Second reviewer, helped write the first draft of manuscript and helped in creating tables. H.J.—Initial concept, referee, editor of manuscript, and guarantor.
Author Disclosure Statement
No competing financial interests exist.