
Abstract
Introduction:
The American Urological Association (AUA) guidelines recommend partial nephrectomy (PN) as the gold standard for treatment of small renal masses (SRMs). This study examines the change in utilization of partial and radical nephrectomies at teaching and nonteaching institutions from 2003 to 2012.
Materials and Methods:
The data sample for this study came from the Healthcare Cost and Utilization Project Nationwide Inpatient Sample from 2003 to 2012. International Classification of Diseases, Ninth Revision and Clinical Modification codes were used to identify patients undergoing PN and radical nephrectomy for renal masses limited to the renal parenchyma. Teaching hospitals were defined, but not limited to any institution with an American Medical Association-approved residency program. Linear regression, bivariate, multivariate, and odds ratio analysis were used to demonstrate statistical significance.
Results:
39,685 patients were identified in teaching hospitals, and 22,239 were identified in nonteaching hospitals. Prior to the 2009 AUA guidelines, cumulative rates of PN were 33% vs 20% in teaching vs nonteaching hospitals (p < 0.0001) compared with postguideline rates of 48% vs 33% in teaching vs nonteaching hospitals (p < 0.0001).
Conclusions:
During the 10-year study period, the use of PN to treat SRMs has significantly increased in both teaching hospitals and in nonacademic centers; however, these changes are occurring at a slower rate in nonteaching hospitals.
Introduction
T
The National Cancer Institute estimates that 61,560 new cases of renal cell cancer will be diagnosed in the United States in 2015. 4 A majority of these patients are diagnosed when the tumor is still organ confined and amenable for curative surgery. The current study aims to elucidate the differences of surgical management between teaching and nonteaching hospitals for patients undergoing nephrectomy for localized renal masses, specifically with regard to adoption of treatment guidelines for small renal masses (SRMs) published in 2009 by the American Urological Association (AUA). 5 We hypothesize that the rates of routine partial nephrectomy (PN) adoption for SRMs in nonteaching hospitals are increasing at a lower rate than in teaching hospitals. The current study investigates changes in clinical practices after the AUA guideline implementation in November 2009 in an effort to demonstrate a relative delay on the part of nonteaching institutions to adopt the new recommendations.
Materials and Methods
Data source
Data for this study were obtained from the Healthcare Cost and Utilization Project (HCUP) National Inpatient Sample (NIS) from January 2003 to December 2012. The NIS is a de-identified publically available national database developed by the Agency for Healthcare and Quality (AHRQ) to provide researchers with information regarding healthcare utilization, quality, cost, and outcomes. The NIS contains all payer data on hospital inpatient stays from States participating in the HCUP and provides annually updated information on ∼8 million inpatient stays from about 1000 hospitals. All discharges from sampled hospitals are included in the NIS database. The NIS is designed to approximate a 20% sample of U.S. community hospitals. Included among community hospitals are specialty hospitals such as obstetrics gynecology, ear nose throat, orthopedic, and pediatric institutions. Also included are public hospitals and academic medical centers. During the 10-year study period, a total of 46 states participated with the exception of Alabama, Arkansas, Delaware, and Idaho. The NIS database provides diagnosis and procedure codes according to the International Classification of Diseases, Ninth Edition (ICD-9). Additional coded data pertaining to hospital discharge include, but are not limited to, patient demographics, hospital characteristics, total charges, and length of stay.
Patient selection
Patients who underwent either PN or radical nephrectomy (RN) for benign or malignant SRMs limited to the renal parenchyma were drawn from the NIS database and selected according to hospital ICD-9 diagnosis and procedure codes (Appendix Table A1). All patients with the procedure codes for partial and radical nephrectomy were analyzed initially. This group of subjects was then further limited to patients without evidence of extrarenal disease and patients with benign neoplasm of the kidney except pelvis and malignant neoplasm of the kidney except pelvis. Benign masses were included for completion with the assumption that a small proportion of clinicians would be operating with equivocal radiologic evidence that may lead to removal of pathologically benign lesions. Patients with procedures billed as nephrectomy of remaining kidney, removal of transplanted or rejected kidney, and bilateral nephrectomy, as well as those with evidence of extrarenal tumor spread as demonstrated by lymph node dissection or metastatic disease, were excluded.
Institution stratification
Patients undergoing nephrectomy for renal masses meeting the above inclusion criteria were stratified by hospital type as follows: urban teaching institutions, urban nonteaching institutions, and rural institutions. Institutions defined by the NIS database as teaching hospitals were those with an American Medical Association-approved residency program or with membership to the Council of Teaching Hospitals.
Study parameters
Patients assigned to teaching, nonteaching, and rural cohorts were then stratified by type of nephrectomy to either partial or radical nephrectomy. Nephrectomy method was determined using procedure codes for robotic assistance and laparoscopic assistance. Of note, robotic procedures were not introduced into the ICD-9 registry until the first quarter of 2008. Age, sex, length of hospital stay, inpatient hospital charges, and mortality rate were examined. Elderly was defined as greater than or equal to 60 years old.
Complications
Selection of inpatient complications was determined based on rates of acute postoperative complications reported in the literature. 6,7 Surgical complications included in the study were multiple and are detailed in Appendix Table A1. Complication incidence was analyzed, and relative risk association within each particular system was calculated.
Statistical analysis
A statistical analysis of categoric outcome variables was performed using unpaired t-tests and two-tailed chi squared with Yates' correction. Linear regression analysis was completed using Pearson correlation coefficients with two-sided p-values with a statistical cutoff of p < 0.05, set a priori. Crude odds ratio (OR) with 95% confidence interval (95% CI) and z statistics were determined where appropriate with a statistical cutoff of p < 0.05, set a priori. Statistical analysis was performed with the use of Statistical Package for the Social Sciences (SPSS) version 22 (IBM Corporation, Armonk, NY).
Results
Study cohort
A total of 66,068 patients underwent nephrectomy of any type between 1/2003 and 12/2012. Within this population, 39,924 (60%) received treatment at a teaching hospital and 22,439 (34%) at a nonteaching hospital. An additional 3705 (6%) patients underwent nephrectomy at a rural institution. The proportion of patients receiving care increased at teaching hospitals from 55% to 67% during the study period (r = 0.94; p < 0.0001) and decreased in nonteaching hospitals from 37% to 28% (r = −0.83; p < 0.01). The proportion of patients undergoing nephrectomy in rural hospitals did not significantly change during the study period.
Partial nephrectomy vs radical nephrectomy
The proportion of PN relative to RN increased in teaching, nonteaching, and rural institutions during the study period. PN rate increased from 27% to 50% in teaching hospitals (r = 0.97; p < 0.0001) and from 16% to 34% in nonteaching hospitals (r = 0.95; p < 0.0001) (Fig. 1). Conversely, utilization of radical nephrectomy decreased from 74% to 50% in teaching (r = −0.97; p < 0.0001) and 84% to 66% in nonteaching institutions (r = −0.95, p < 0.0001). In the rural setting, PN rates increased from 14% to 32% during the study period (r = 0.83; p < 0.01). The respective mean incidence of PN before and after the 2009 AUA guidelines was 33% and 48% (p < 0.0001) at academic and 20% and 30% (p < 0.0001) at nonacademic institutions. Patients were more likely to undergo PN in teaching hospitals relative to nonteaching hospitals both before (OR: 1.94, CI: 1.84–2.02; p < 0.0001) and after (OR: 1.91, CI: 1.80–2.03; p < 0.0001) AUA guidelines.
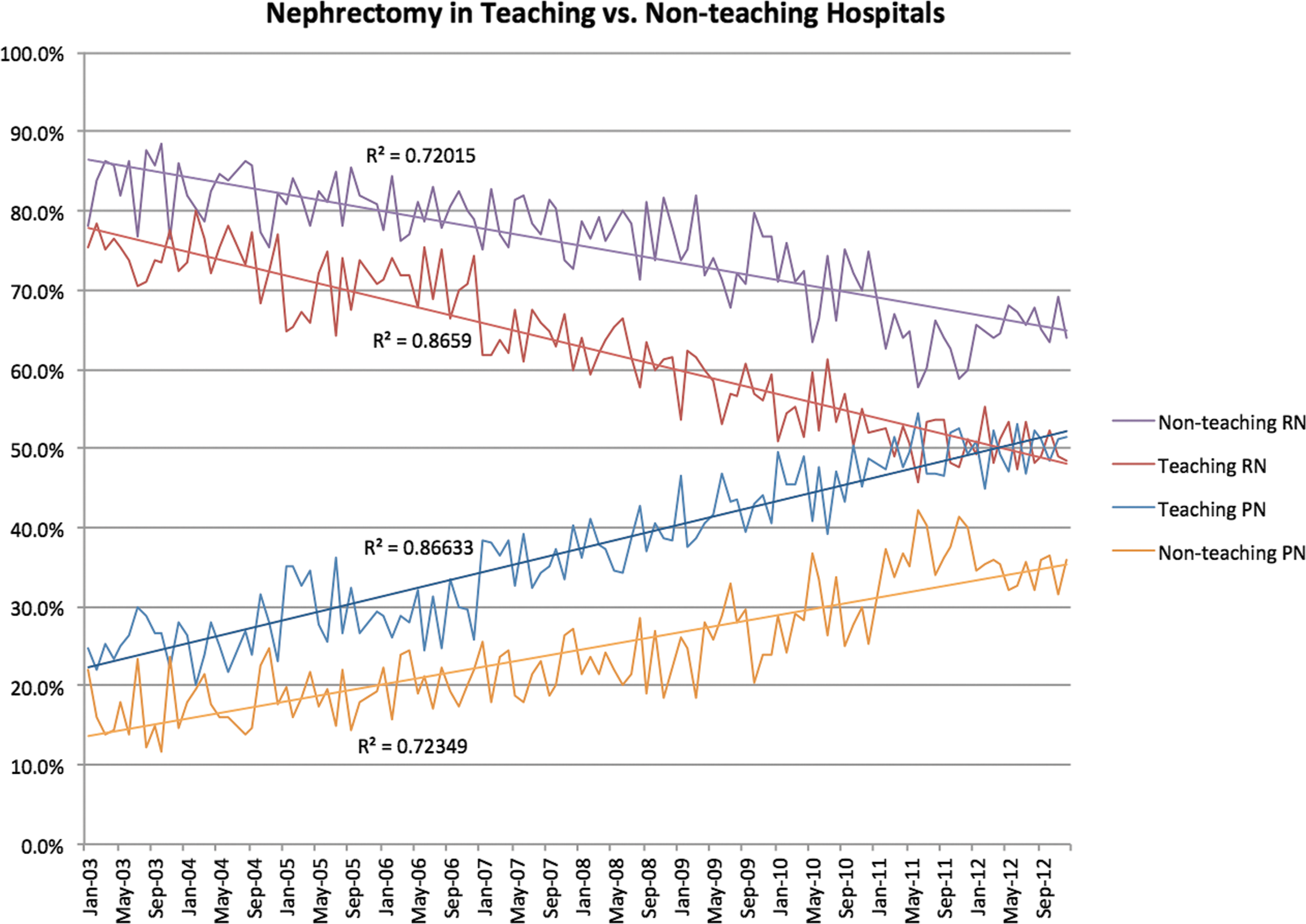
Nephrectomy in teaching vs nonteaching hospitals. The decline in radical nephrectomy utilization in nonteaching and teaching institutions and the rise of partial nephrectomy (PN) in teaching and nonteaching institutions. (1) Nonteaching radical nephrectomy, (2) Teaching radical nephrectomy, (3) Teaching PN, and (4) Nonteaching PN.
Robotic vs laparoscopic assistance
Between 1/2003 and 12/2007, the proportion of laparoscopic nephrectomies (LN) increased from 15% to 17% at teaching hospitals (r = 0.14, p = 0.82) and from 9% to 13% in nonteaching hospitals (r = 0.60, p < 0.28). Between 1/2008 and 12/2012, the rate of LN decreased in both institution types, from 19% to 14% in teaching (r = −0.97, p < 0.01) and from 18% to 14% in nonteaching (r = −0.80, p = 0.11). During the same period, rates of robotic nephrectomy increased in teaching hospitals from 1% to 30% (r = 0.98, p < 0.01) and in nonteaching hospitals from 1% to 22% (r = 0.97, p < 0.01). Following the release of the AUA guidelines, the mean incidence of LN decreased from 17% to 15% (p < 0.0001) at academic institutions and increased from 13% to 15% (p < 0.0001) at nonacademic institutions. Before AUA guidelines, teaching hospitals utilized more robotic (OR: 1.53, CI: 1.30–1.81; p < 0.0001) and laparoscopic (OR: 1.37, CI: 1.30–1.45; p < 0.0001) assistance than nonteaching hospitals. Following AUA guidelines, teaching hospitals still utilized more robotic assistance (OR: 1.34, CI: 1.25–1.44; p < 0.0001) than nonteaching hospitals; however, there was no difference in laparoscopic assistance between the two institution types (OR: 0.98, CI: 0.90–1.06; p = 0.56).
Complications
Overall complication rates increased in teaching institutions from 32% to 34% (r = 0.79; p < 0.01) and from 34% to 37% in nonteaching institutions (r = 0.63; p = 0.05). At teaching and nonteaching institutions, hematologic complications increased from 8% to 13% (r = 0.90; p < 0.001) and 9% to 12% (r = 0.90; p < 0.001), respectively, and renal complications increased from 5% to 9% (r = 0.94; p < 0.001) and 5% to 12% (r = 0.90; p < 0.001), respectively. Before the guidelines, there was no difference in surgical, wound, cardiac, or pulmonary complications between teaching and nonteaching hospitals, but transfusion rates, digestive, renal, hematologic, and infectious complications were less likely to occur in teaching hospitals (OR: 0.85, CI: [0.81–0.89]; OR: 0.89, CI: [0.83–0.95]; OR: 0.80, CI: [0.74–0.85]; OR: 0.87, CI: [0.80–0.94]; OR: 0.82, CI: [0.77–0.88]; and OR: 0.80, CI: [0.73–0.88], respectively, with all p < 0.01). After the guidelines, there was no difference in surgical, wound, and hematologic complications in teaching and nonteaching hospitals, but transfusion rates, digestive, renal, infectious, cardiac, and pulmonary complications were less likely to occur in teaching hospitals (OR: 0.83, CI: [0.76–0.91]; OR: 0.70, CI: [0.63–0.76]; OR: 0.73, CI: [0.66–0.80]; OR: 0.84, CI: [0.73–0.96], p = 0.01; OR: 0.83, CI: [0.75–0.93]; OR: 0.69, CI: [0.61–0.79], respectively, with remaining p < 0.01) (Figs. 2 and 3).
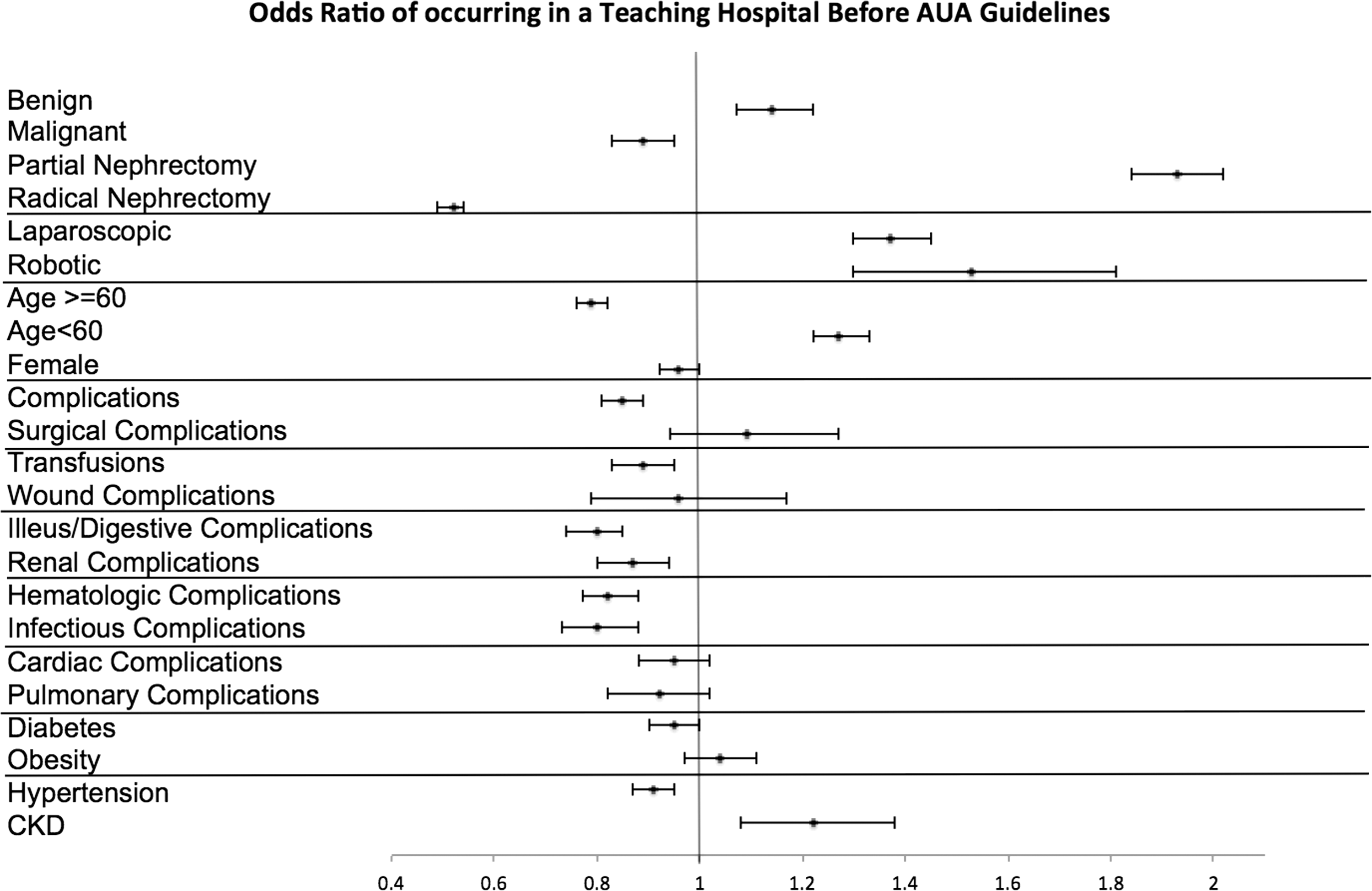
Odds Ratio of occurring in a Teaching Hospital before AUA guidelines. Odds of tumor characteristics, operative method, patient demographics, complications, and patient comorbidities in teaching hospitals before the 2009 AUA guidelines for treatment of small renal mass (SRM). AUA = American Urological Association; CKD = chronic kidney disease.
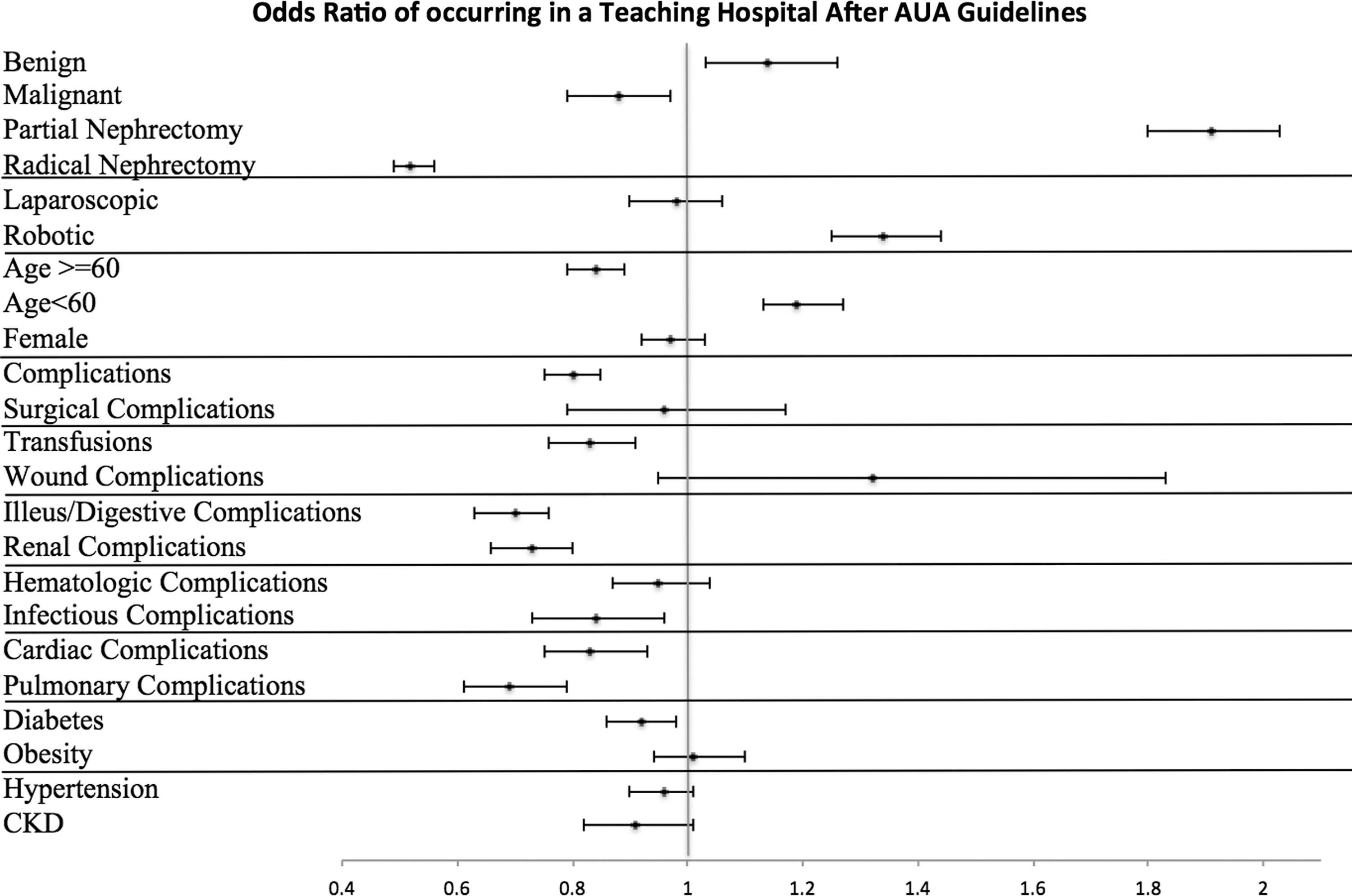
Odds Ratio of occurring in a Teaching Hospital after AUA guidelines. Odds of tumor characteristics, operative method, patient demographics, complications, and patient comorbidities in teaching hospitals after the 2009 AUA guidelines for treatment of SRM.
A decrease in hospital length of stay was observed in both teaching institutions, from 5.64 to 4.21 days (r = −0.99; p < 0.001), and nonteaching institutions, from 5.74 to 4.45 days (−0.92; p < 0.001). Mean hospital length of stay before and following AUA guidelines was 5.07 and 4.41 days (p < 0.001) in teaching and 5.26 and 4.57 days (p < 0.001) in nonteaching institutions, respectively.
Discussion
For much of the 20th century, radical nephrectomy remained the gold standard for treatment of SRMs. An increasing volume of evidence has since demonstrated that PN may allow for preservation of renal function, decrease in cardio and cerebrovascular complications postoperatively, and greater overall survival (OS) compared with RN while maintaining excellent oncologic outcomes. 6,8 As such, the 2009 AUA guidelines recommend the use of PN as the standard treatment for T1a renal mass. 5 Despite these societal guidelines, consensus data suggest that PN remains underutilized for the treatment of SRMs. 9 In an effort to elucidate the reasons for the slow adoption of nephron-sparing surgery (NSS), efforts to describe national trends in incidence of PN are underway. 6,10 –12
Evidence shows that NSS promotes the preservation of renal function in both progression to advanced stages of chronic kidney disease (CKD) and decline in glomerular filtration rate. 13 –16 Furthermore, the effects on renal function preservation can be linked to improved cardiovascular functioning and reduction in both cardiovascular-related death and overall death. 17 Survival data show that stage T1a renal cancer treated with PN provides comparable 5-year survival rates to RN. 17 Despite these findings, the only study conducted with the highest level of evidence spanning multiple centers showed that RN was superior to NSS in OS. 18 This randomized control study has since been met with a great amount of criticism and skepticism arguing that results cannot be generalized; nevertheless, such data clouded the current debate regarding early stage renal-cell carcinoma and the role of NSS. 19 –22
Given this controversial literature regarding nephrectomy, it is important to evaluate what other factors are contributing to clinicians' decisions for treatment of SRMs. Interestingly, before the 2009 AUA guidelines, data showed an increase of PN utilization and adoption in both academic vs nonacademic centers, yet higher rates of NSS in teaching hospitals. Woldrich and colleagues 23 found that large urban teaching hospitals were more likely to perform PN than small rural nonteaching hospitals. Breau and associates determined that an academic background as either an academically affiliated urologist or a fellowship trained surgeon was highly predictive in performing PN and treating patients with NSS. 24 With the changing tides in literature and evidence of NSS efficacy, one wonders if simple close association with an academic institution might affect adherence to guidelines.
This study examined the practice of nephrectomy for SRM while examining a decade of trends and differences between urban-teaching and urban-nonteaching hospitals spanning the AUA guideline implementation and beyond. We show that although the total number of partial nephrectomies is increasing nationally in both the teaching and nonteaching settings, the rate of partial nephrectomies being performed by each institution is higher for teaching hospitals than their nonteaching counterparts both before and after implementation of AUA guidelines. Liss and coworkers 11 similarly explored the incidence of PN across U.S. hospitals between 2007 and 2011 and found evidence of increased PN utilization independent of AUA guideline release that further support our findings.
It is still unclear why nonteaching hospitals have consistently lower rates of PN. Opponents of NSS recognize the technical difficulty associated and postulate that the absence of surgical experience may be a primary factor for underutilization. Although some data suggest that uptake of laparoscopy is associated with younger surgeon age and higher surgical volume, the same study showed that adoption of PN is only demonstrably associated with status as an academic surgeon. 25 Others point toward controversial literature on OS for RN vs PN as an argument against adapting a new surgical practice. Given the high barrier to entry for this skillful procedure in nonacademic centers, our predication is that until established studies help more clearly define the correct procedure, there will remain a gap between teaching and nonteaching rates of PN. Unfortunately, this gap may perpetuate a disparity in operative ability leading to longer operative times, higher complication rates, and worsening all cause mortality rate.
Limitations of our study largely stem from utilization of the HCUP NIS data source. The Council of Teaching Hospitals' definition of “teaching hospitals” extends beyond just institutions with urologic trainees and includes other residency programs such as anesthesia and ICU, as well as ancillary training programs such as nursing. Despite this distinction, there is some uncertainty as to the degree of trainee involvement between academic centers. The NIS is an inpatient database with information drawn from hospital admissions, which inherently lack information regarding cancer recurrence, development of CKD, or other long-term outcome metrics. The NIS draws data from ICD-9 billing codes, and a degree of interprovider variation is expected. Procedure codes for robotic procedures were introduced in 2008, and prior data pertaining to rates of robotic nephrectomies were unavailable; however, studies have shown robot-assisted PN to be safe and effective. 26 No ICD-9 diagnosis codes exist for tumor staging, and thus, tumor size and location were approximated using codes detailed in the Methods section. Despite these efforts, it is not possible to differentiate between T1a and T1b masses in the NIS database, which is relevant with respect to AUA guidelines. Finally, the NIS represents a subset of the US population and, therefore, is certainly not comprehensive in its scope.
Conclusions
The rate of PN increased significantly relative to RN in the period between January 2003 and December 2012, with a more pronounced trend in teaching than nonteaching hospitals. However, the rate of PN utilization did not further diverge after the 2009 AUA guidelines. The etiology of these trends is multifactorial and may involve absence of familiarity with PN in nonacademic institutions and increased referral to academic centers for PN, as well as academic centers' adoption of PN before the AUA guidelines. However, in concordance of the AUA guideline recommendation, the authors would recommend referral for any indicated PN to a surgeon with this particular skill set. Consistent with prior studies, we did not observe a considerable change in postoperative complications in the context of increased PN use. While a clear gap exists in utilization of PN between teaching and nonteaching institutions, further studies are needed to determine the etiology for this difference. Studies investigating practitioners' participation in CME events, reading of Guidelines, and attendance at national and regional AUA meetings are the next step in understanding this trend.
Footnotes
Author Disclosure Statement
No competing financial interests exist.