
Abstract
Objective:
To assess the feasibility and safety of a modified retroperitoneoscopic technique in supine position for the primary tumors located below the level of renal pedicle.
Materials and Methods:
In this retrospective study, 27 patients with primary retroperitoneal tumors located below the level of renal pedicle were recruited from January 2009 till now. The mean age of patients was 49.0 years (36–66 years). The average body mass index was 21.1 ± 1.4 kg/m2. The retroperitoneoscopic resections were performed in supine position for all patients. The perioperative outcomes were collected and analyzed.
Results:
All cases were performed by the modified technique without converting to open surgery. The mean operation time was 98.3 ± 12.8 min, with a mean estimated blood loss of 94.4 ± 42.5 mL. There were four patients suffering from intraoperative complications, one with the inferior vena cava (IVC) injury, one with the lumbar vein injury, and other two with the peritoneum breach. Postoperatively, the median bowel recovery time was 2 days (range: 1–3 days), and the mean length of stay after operation was 2.9 ± 1.0 days. Additionally, compared with the tumors located around the aorta (region B), a longer operation time was needed with tumors located around the IVC (region A) (A vs B: 105.8 ± 10.2 vs 91.2 ± 14.4, p = 0.02). Histopathology confirmed paraganglioma in 5 cases, schwannoma in 10 cases, and ganglioneuroma in 12 cases. After follow-up of 12–72 months, no recurrences have been identified.
Conclusion:
Our modified retroperitoneoscopic technique in supine position was proven to be safe and effective for the treatment of primary retroperitoneal tumors, especially suitable for the tumors located below the level of the renal pedicle.
Introduction
R
Laparoscopic surgery, popularized in the late 20th century, is commonly used in performing adrenalectomy, nephrectomy, and retroperitoneal lymph node dissection and has the benefits of better postoperative recovery and cosmetic outcomes. 5 –7 Recent advancements in technology coupled with operator experience have allowed urologic surgeons to broaden the indication of laparoscopic surgery in the treatment of retroperitoneal tumors regardless of their location. The transperitoneal approach has been increasingly reported in operations involving benign schwannomas, ganglioneuromas, and lesions adjacent to the aorta and inferior vena cava (IVC). 8 –10 De Fourmestraux and his associates reported their experience with retroperitoneal laparoscopic resections of extra-adrenal pheochromocytomas and reported advantages of lesser handling of abdominal organs and shorter duration of hospitalization. 11 However, it was limited for a surgeon to perform retroperitoneoscopic excision of tumors located below the level of renal pedicle in a decubitus position. Hence, some certain additional technical modifications were made to develop a new method of retroperitoneoscopic excision of primary retroperitoneal tumors. Herein, we report our experience with the initial 27 cases of such resections performed at our center and analyze the feasibility and safety of our technique.
Patients and Methods
Clinical characteristics
From January 2009 till date, a total of 27 patients underwent retroperitoneoscopic resection of retroperitoneal tumors. Patient recruitment was based on the following criteria. (1) The retroperitoneal mass was the primary tumor in the retroperitoneal space (all adrenal, renal, and lymph node masses were excluded) and (2) the retroperitoneal mass was located inferior to the level of the renal pedicle.
All patients underwent preoperative examinations, including abdominal CT (plain and contrast enhanced) and adrenal hormone tests (including the 24-hour urinary vanillylmandelic acid test). Based on the CT scan results, five patients were diagnosed as having ectopic pheochromocytomas and received preoperative α-adrenergic blockade (phenoxybenzamine at dosages of 15–30 mg per day for 2 weeks). Beta-adrenergic blockade with metoprolol and calcium channel blockers (nifedipine) was additionally used if tachycardia developed. In addition, these five patients received 5% dextrose, 0.9% normal saline, and 400 mL of plasma to expand blood volume 1 day before the operation. Three units of red blood cells and 600 mL plasma were reserved for the surgery. The detailed clinical characteristics of the 27 patients are listed in Table 1.
BMI = body mass index, EBL = estimated blood loss, IVC = inferior vena cava, SD = standard deviation.
Tumor location
The retroperitoneal space below the level of renal pedicle was divided into four regions: A, B, C, and D based on anatomic landmarks. Regions A and B were located between the level of the renal pedicle and the bifurcation of common iliac vessels. The vertical lines on each side corresponded to the ureter and the great vessels (the aorta on the left side and the IVC on the right side). Region A was defined as the area lateral to the right ureter and medial to the IVC. Region B was defined as the area lateral to the left ureter and medial to the abdominal aorta (Fig. 1). Region C was defined as the area between the IVC and the aorta. Region D, located below the level of inferior mesenteric artery (IMA), included several important structures, such as the common iliac vessels, the root of IMA, and presacral vessels.
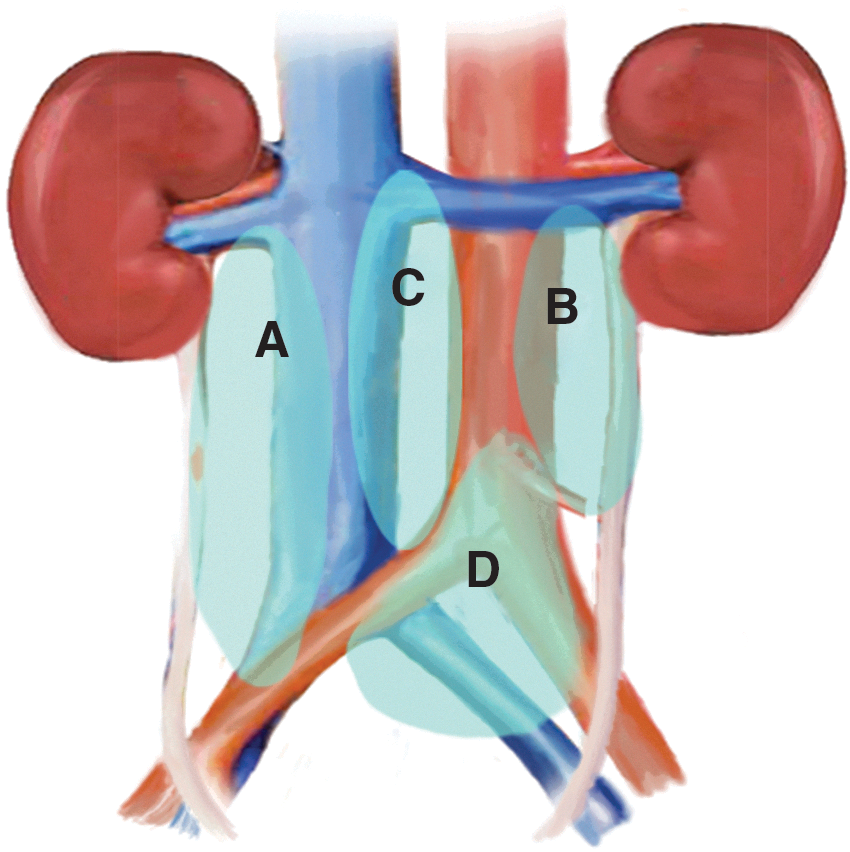
Sketch of divisions for the retroperitoneal space located below the level of renal pedicle.
Surgical technique
Patient position
All the patients were placed in the supine position according to the description provided in Qin's article. 12 The surgeon and two assistants stood on the side ipsilateral to the tumor, one holding the camera and another one helping the surgeon expose the retroperitoneal space. Video monitors were placed on the other side to provide a comfortable view to the surgeon as well as the assistants.
Surgical procedure
After induction of general anesthesia, a 15-mm incision was made ipsilateral to the tumor, 2–3 cm medial and superior to the anterior iliac spine. The fascia of the external oblique muscles and internal oblique and transverse muscles was bluntly divided along the fibers to reach the retroperitoneal space. Through the incision, the surgeon swept the peritoneum inward by using the index finger. An improvised balloon was inserted into the retroperitoneal space through the incision and inflated with about 800 mL of gas to expand the space. After removal of the balloon, three trocars were inserted into retroperitoneal space (7–8 cm lateral and superior to the first incision, 7–8 cm medial and inferior to the first incision, and 7–8 cm superior to the first incision, trocars B, C, and D, respectively) under the guidance of the surgeon's index finger. A 10-mm trocar (trocar A) for the camera was inserted through the first 15-mm incision. For tumors located in region D, the distribution of trocars was modified as shown in Figure 2. Pneumoperitoneum was created by using an insufflator to a pressure of 15 mmHg. Care was taken to avoid injuring the peritoneum.

Distribution of trocars. Trocar A, B, C, and D were applied for tumors located above the level of the root of IMA. While for tumors below the level of the root of IMA (region D), distribution should be modified as A’, B’, C’, and D’. IMA = inferior mesenteric artery.
Retroperitoneal fat was removed by using a harmonic scalpel. Gerota's fascia was identified and incised longitudinally with a harmonic scalpel. The tissue was dissected medially along the psoas muscle until the ipsilateral great vessel was revealed (the abdominal aorta on the left side and the IVC on the right side). The primary tumor located caudal to the renal pedicle was recognized, and it was necessary to fully expose the great vessels nearby the tumors. A harmonic scalpel was used to gently dissect the adjacent tissues around the tumor to avoid the breach of tumor capsule. In addition, some major or multiple vessels supplying the tumor should be ligated in different ways, such as hem-o-lock, titanium clips, and harmonic scalpel.
After complete mobilization from the retroperitoneal bed, the tumor was retrieved in a specimen bag and extracted through the camera port (corresponding to trocar A). Finally, a drainage tube was placed into the retroperitoneal space before wound closure. The histopathologic examination was available in a few days.
Follow-up
Patients were planned for annual follow-up for the first 10 years after the operation. A follow-up examination included clinical examination (blood pressure and ECG among others), biochemical tests, and an abdominal CT scan.
Results
The resection of retroperitoneal mass was effectively performed by using the retroperitoneoscopic technique as described for all 27 patients. The basic clinical characteristics of the 27 patients are shown in Table 1. There were 14 men and 13 women, with ages ranging from 36 to 66 years (mean age ± standard deviation, 49.0 ± 6.4 years). The mean tumor size was 3.6 ± 0.8 cm.
Seventeen of the cases were performed by a right-sided approach. The mean operation time (defined as the time from the initial skin incision to the final closure of the incision) was 98.3 ± 12.8 minutes, and the estimated blood loss during the operation was 94.4 ± 42.5 mL. There were four patients suffering from intraoperative complications, one with the IVC injury, one with the lumbar vein injury, and other two with the peritoneum breach. During the operations, there were no instances of ureter injury. Neither the trunk nor the branches of the renal pedicle were injured in these cases.
A total of five patients required blood transfusion during the operative procedure, all of whom were diagnosed as having paragangliomas (also called the ectopic pheochromocytoma) on histopathology. All patients got out of bed on the second day after operation. The median bowel function recovery time (defined as the time to passing flatus) was 2 (1–3) days. The mean length of stay (LOS) was 2.9 ± 1.0 days. In the postoperative period before their discharge, no one experienced the position-related morbidities (PRM), such as local pain or pressure sores.
Postoperatively, pathologic results revealed paragangliomas in 5 patients, schwannomas in 10 patients, and ganglioneuromas in 12 patients. All resected specimens showed a negative incisional margin. No recurrences have been identified till date in the duration of follow-up ranging from 12 to 72 months.
The data were stratified according to the anatomic regions mentioned earlier. There were 9, 10, 5, and 3 tumors located in regions A, B, C, and D, respectively. The detailed clinical and operative information is presented in Table 2. Compared with tumors in region B, region A experienced longer operative time (p = 0.02). There was no significant difference between region A and region B in the aspect of tumor size, estimated blood loss, bowel recovery time, and LOS. In addition, two cases of vein injury (IVC and lumbar vein) during operation happened in region A, and two cases of peritoneum breach happened in region C.
Bold value represent that there is a significant difference between Region A and Region B in operative time. The symbol “/” means that we didn't do the comparisons in these items.
Discussion
With recent advances in the laparoscopic technique, laparoscopic surgeries are increasingly performed for the resection of retroperitoneal tumors. Ohigashi and his colleagues first reported laparoscopic resection of retroperitoneal benign schwannoma using a transperitoneal approach, 8 and since then, the transperitoneal approach has remained as the main technique globally for primary retroperitoneal tumors, or for tumors originating from the adrenal gland, kidneys, or ureters. Several researchers considered the broad working space and maximal tumor exposure as the advantages with this approach. 9,13 –16 In 2006, Walz et al. reported endoscopic resection of 27 paragangliomas, of which 11 were performed through a retroperitoneoscopic approach. Their results proved the safety and feasibility of retroperitoneoscopic removal of retroperitoneal paragangliomas and suggested the superiority of the retroperitoneal approach owing to its “no touch technique.” 17
Retroperitoneoscopic technique in the supine position was reported to be effective in retroperitoneal lymph node dissection and ureterolithotomy. 18,19 In our center, we previously reported 15 effective cases of retroperitoneal lymph node dissection with low operative complications and short postoperative hospitalization by using this method. 12 As a part of the present study, we used the retroperitoneoscopic method in the supine position, in 27 patients, for resection of primary retroperitoneal tumors, without any obvious complications.
Several aspects of the surgical protocol followed by us, in performing this technique, need emphasis. The first one pertains to the distribution of the four trocar ports in the modified method. The placement of the ports is determined based on the specific anatomical region that contains the tumor. Specially, the right-sided approach is recommended for tumors located between the aorta and IVC (region C). Pneumoperitoneum created and maintained at pressures of 15 mmHg results in flattening of the IVC and enables easier access to the tumors in this region. The placement of the ports should be modified for tumors located in regions D, as shown in Figure 2.
The second noteworthy factor is to avoid peritoneal breach during the operation. The biggest shortcoming of the retroperitoneal approach is the relatively smaller working space compared with the transperitoneal approach. In our experience, blunt finger dissection and balloon dilation at the beginning of the procedure were essential steps in avoiding peritoneal breach. Furthermore, there was no need to extensively isolate the peritoneum, and as described, dissection along the psoas provided a quick and safe access to the tumor; this may have further contributed to preventing peritoneal injury. Unfortunately, two cases in our study suffered from the peritoneal breach, which resulted in contraction of the working space. In these two cases, hem-o-lock clips were used to close the defect, and a fan-shaped retractor was introduced to maintain the retroperitoneal space.
Third, when dissecting around the tumor, there are certain region-specific precautions to be observed. As the retroperitoneal tumors are in proximity to the large vessels, it is necessary to extensively dissect the aorta or vena cava nearby the mass. This enables clear delineation of tumors before they are resected. In addition, tumors in region A always located posterior to the IVC, which could make it more difficult for surgeons to perform resection. As a result in our study, the tumors in region A experience longer operation time than the tumors in region B. For this reason, when dealing with the tumors in region A, the complexity and variation of lumber veins should be recognized and they should be adequately controlled to avoid the risk of serious bleeding.
If the tumors are located near the renal pedicle (for these tumors located in region A, B, and C), the renal vessels and their branches should be preserved. For tumors in regions A and B, ureters should be protected from injury during dissection. Region D includes presacral vessels and the root of the IMA, which may be associated with complications of severe bleeding and bowel ischemia if injured. Therefore, care should be taken to preserve these important structures during resection of tumors in region D.
Finally, during the dissection of the tumors, some amount of fatty tissue on the surface of tumors should be retained, as it is helpful in grasping, retracting, and removing the tumor. In addition, for pheochromocytomas, this method of grasping results in reduced direct tumor handling, thus avoiding blood pressure fluctuations. This aspect of the operation was also shared by Jiaji et al. 13
Compared with the transperitoneal approach, our modified technique has several strengths. First, if the peritoneum is intact, this technique offers direct access to the primary lesion without interference from intra-abdominal organs and reduces risk of injury to adjacent organs, including the stomach, bowel, and liver. Thus, it can decrease the incidence of postoperative complications, including ileus, peritoneal adhesion, and peritonitis, and result in shorter LOS after operation. This is confirmed by our data demonstrating a short LOS of 2.9 ± 1.0 days. Second, the retroperitoneal approach is associated with the additional advantages of avoiding the respiratory and hemodynamic effects of carbon dioxide (CO2) pneumoperitoneum. Reiner and his colleagues reported on the evidence for the Starling resistor concept of abdominal venous return in transperitoneal and retroperitoneal carbon dioxide insufflation during surgical procedures, and suggested that the transperitoneal approach could impair cardiac filling at higher insufflation pressures. 20
Third, our modified technique performed in the supine position offered an easier access for retroperitoneal tumors located below the level of renal pedicle, compared with the decubitus position. Walz and his colleagues reported 27 paragangliomas (ectopic pheochromocytomas), which were treated by laparoscopic surgery through retroperitoneal (n = 11) or transperitoneal approach (n = 16). In Walz's study, all the operations were performed in the decubitus position, with different approaches depending on the location of the retroperitoneal tumor. Tumors located cranial to the renal pedicle were excised through a retroperitoneal approach, while tumors located caudal to the renal pedicle were removed by transperitoneal laparoscopy. The authors suggested that by using the transperitoneal approach with the patient in the decubitus position, tumors located below the level of the renal pedicle could be easily accessed after mobilization of the mesocolon and the mesentery. 17
Combining with Soga's results, it is obvious that if the retroperitoneal tumor is located below the level of the renal pedicle, it is difficult to reach through the retroperitoneal approach if the patient is in the decubitus position. However, if the operation was performed with the patient in supine position, the available operative field with retroperitoneoscopic surgery is wider, enabling easier access to these tumors.
PRM, such as pressure sores and pain, are common in patients undergoing prolonged operations in the decubitus position. Chien-Hui Ou and Wen-Horng Yang suggested that the supine position could be associated with lesser risk of PRM when compared with the decubitus position. 21 The supine position provides the largest contact area between the patient's body and the operating table resulting in even pressure distribution. The supine position is, therefore, beneficial as it avoids postoperative pressure sores and pain and facilitates early discharge from hospital.
Vascular injuries and severe bleeding are major complications expected during the procedure. In our experience, adequate hemostasis can be achieved with a harmonic scalpel when dissecting around the large vessels. There may be a need to use titanium clips for some branches of these large vessels to prevent severe bleeding. There was one case of IVC injury and another case of lumbar vein injury in this study. Both the tumors in these two cases were located in region A. The bleeding was temporarily controlled by compressing with gauze. With the help of an aspirator, the location of injury on the IVC was exposed and effectively closed by suturing with 4-0 polypropylene. In addition, the bleeding from the lumbar vein can be totally controlled by titanium clips.
Conclusion
Our modified retroperitoneoscopic technique in supine position was proven to be safe and effective for the treatment of primary retroperitoneal tumors, especially suitable for the tumors located below the level of the renal pedicle.
Footnotes
Acknowledgment
Six Talent Peaks Project in Jiangsu Province (No. 2014-WSW-001).
Ethical Standard
The study was approved by the Local Ethics Committees of the First Affiliated Hospital with Nanjing Medical University, Nanjing, China. Written informed consent was obtained from all participants involved in this study.
Author Disclosure Statement
No competing financial interests exist.