
Abstract
Introduction:
Despite the potential clinical advantages of holmium laser enucleation of the prostate (HoLEP), there has been reluctance of the urologic community to adopt the procedure, as a result of a perceived steep learning curve. Thus, we sought to design and develop a transurethral endoscopic robotic platform for HoLEP.
Materials and Methods:
We developed a novel transurethral, concentric tube robotic platform for HoLEP. We conducted magnetic tracking experiments to compare movements of the end effectors of the robot with those of a rigid endoscope. Additionally, we tested the robot on an HoLEP simulator and with a human cadaveric prostate to assess its ability to maneuver within a small working space.
Results:
In the prostate scanning experiment, the area reached by the robot represents a 65% improvement vs the area accessible by a rigid endoscope without tissue deformation. Additionally, the robot performed well within the confines of the prostatic urethra and was able to successfully complete prostate lobe enucleation, on both the HoLEP simulator and with a human cadaveric prostate.
Conclusions:
We have developed a concentric tube robotic platform that is passed through a standard endoscope that is capable of producing complex movements of the end effectors. We have shown that these movements of the concentric tube manipulators are capable of performing tasks that may eventually translate into improved ease of performing HoLEP.
Introduction
B
Recent evidence has shown that HoLEP is at least as effective as TURP, with less perioperative morbidity, including shorter length of catheter use, lower transfusion rates, and shorter hospital stay. 2,3 HoLEP does have a potential therapeutic advantage compared with other modalities for treatment of BPH, as it allows true anatomic enucleation of prostate adenomas of any size. 4 This has resulted in durable long-term outcomes and low retreatment rates. 5 Despite the potential clinical advantages of HoLEP, there has been a general reluctance of the urologic community to adopt the procedure. A prolonged and challenging learning curve is considered one of the main disadvantages of HoLEP and has been cited as one of the main causes for delayed dissemination of this effective surgical procedure. 6 –9 The reasons for the challenging initial learning period have been varied. Some authors have identified a lack of accessible mentorship as a prominent explanation. 7 Others have suggested that operative challenges such as a small working space, close working distance, and complex scope movements required for enucleation are also responsible. 6,10
There has been recent interest in developing robotic technology to assist with transurethral surgery. Some early work with transurethral robotics focused on TURP, with the goal of improving safety and accuracy of prostate resection. 11 –13 Although they are interesting technologies, none of these robotic platforms garnered much clinical interest. This is likely a result of the wide dissemination of TURP and the coinciding rise of laser technology for treatment of BPH. Not surprisingly, newer transurethral robotic technologies have incorporated use of lasers. Pickens and colleagues described a continuum, snake-like transurethral robot that is capable of simultaneous deployment of working instruments that allows en bloc resection of bladder tumors with a holmium laser in an experimental model. 14 Additionally, Russo and colleagues recently reported on a robotic platform that is compatible with a traditional endoscope that is capable of steering a laser fiber. 15 However, these new robotic platforms remain experimental and have failed yet to approach the realm of clinical practice. Accordingly, HoLEP with its obvious clinical advantages, limited dissemination, and steep learning curve would be an ideal procedure for robotic technology. Thus, we sought to conceptualize, design, and develop a robotic system with the goal of increasing utilization of HoLEP by decreasing the difficulty in performing this highly effective operation.
Materials and Methods
An intensive clinical collaboration between Vanderbilt University engineers and urologists was undertaken to develop a robot to pass through a rigid endoscope. The initial concept of the system was to create a hand-held robotic system, such that the same basic setup and workflow of standard transurethral surgery could be maintained. 16 However, with incorporation of robotics, we sought to add the ability to perform precise and complex movements of working instruments within a small operating space. This project was partially funded by NIH EB017467 and the Vanderbilt Initiative for Surgery and Engineering (VISE).
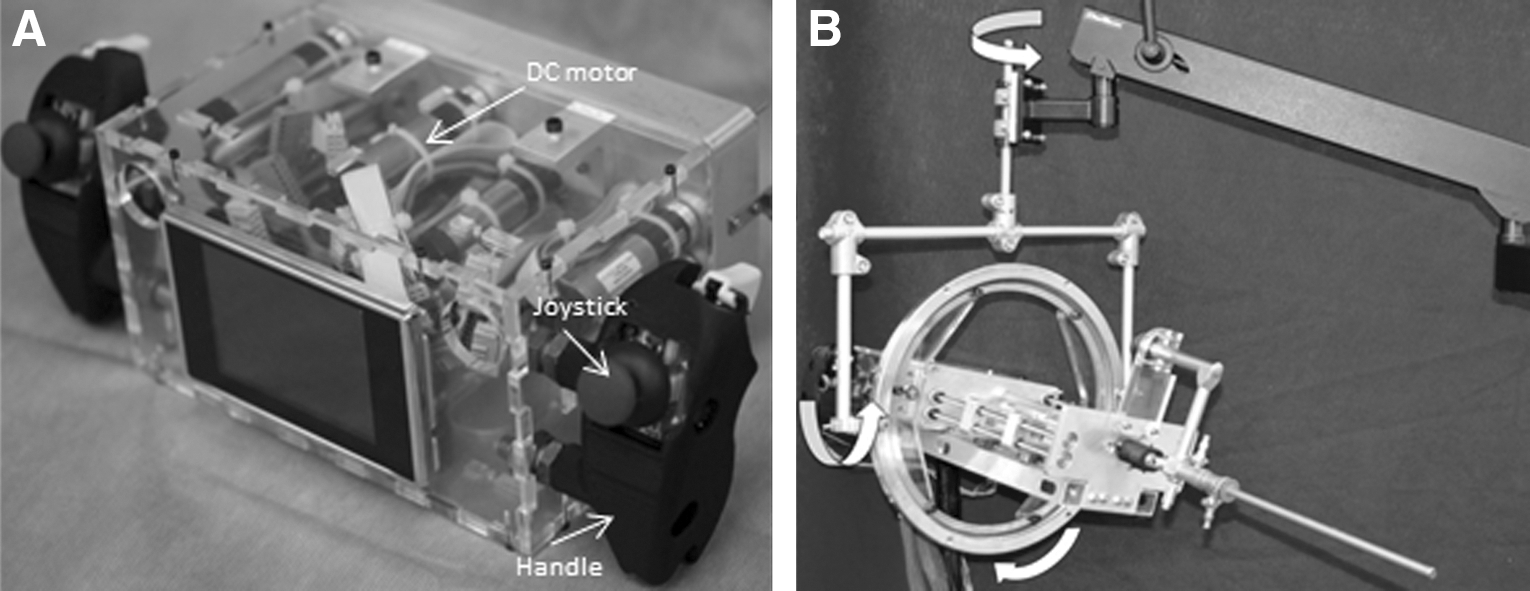
The overall system design is based on the premise of concentric tube robots that utilize concentrically nested, precurved elastic tubes as the end effectors. The basic robotic system consists of three main modules: the user interface, the transmission, and the endoscope (Fig. 1). The user interface is the portion of the robot with which the surgeon directly interacts. This consists of two handles, each with an embedded joystick and a trigger that are linked to motors that are responsible for driving the concentric manipulators. Maneuvering the trigger and joysticks produces corresponding fine motions of the concentric tube manipulators (Fig. 2A). Gross movement of the endoscope is accomplished by using coordinated motions of both hands to manually manipulate the entire unit. The robot is suspended on a counterbalanced arm to assist the surgeon in supporting the weight of the robot (Fig. 2B).
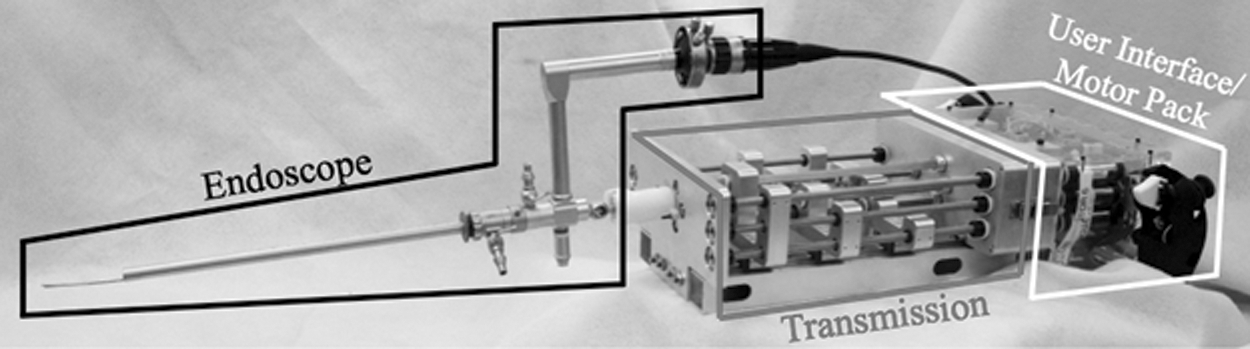
The current configuration of the robotic platform consists of a user interface and a transmission module that is passed through an offset rigid nephroscope.
Within the transmission section, the motion of the motors is converted into translation and rotation of the tubes. This is accomplished by a series of lead screws that are responsible for linear motion and square shafts that are responsible for rotational motion of the concentric tubes (Fig. 3). The current endoscope utilized is a continuous-flow 26F rigid nephroscope (Storz, Inc.) that was chosen, as the offset lens design allows passage of the robot through the working channel. The endoscope contains integrated light sources and optics, a 5 mm working channel through which two concentric tube manipulators are introduced (Fig. 4). Each concentric tube consists of a straight outer tube and a superelastic nitinol inner tube that is preshaped into a curved configuration. When these tubes are translated and rotated, their elastic interaction creates a “tentacle-like” motion.
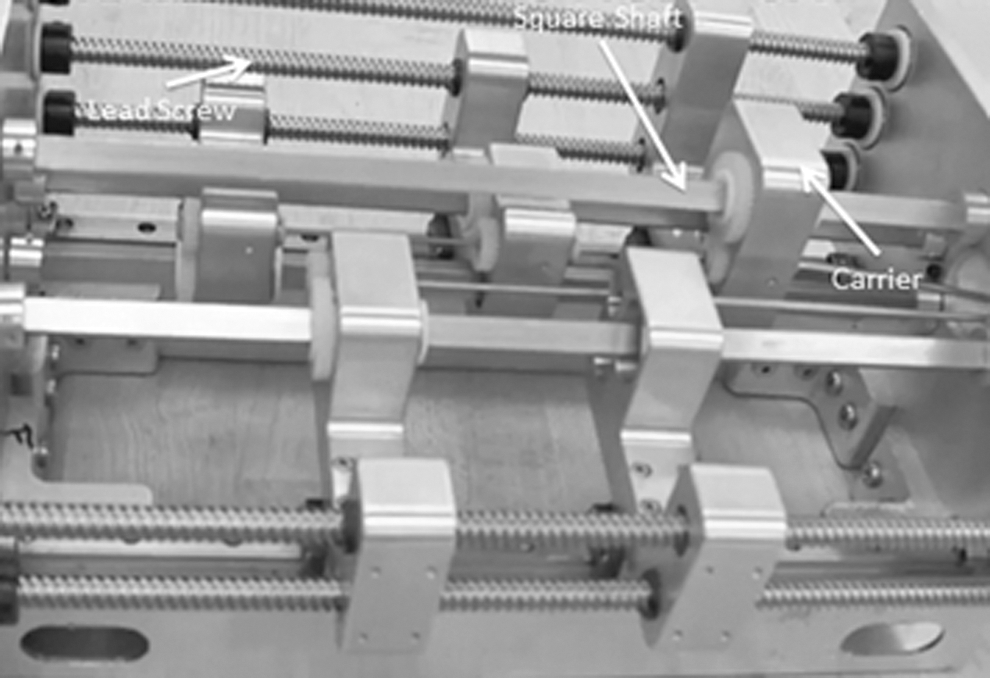
In the transmission section, carriers grasp each concentric tube at its base and apply linear and translational motions originating from the motors.

Distal end of endoscope showing concentric tube manipulators, lens, light sources, and working channels for flow of irrigation fluid.
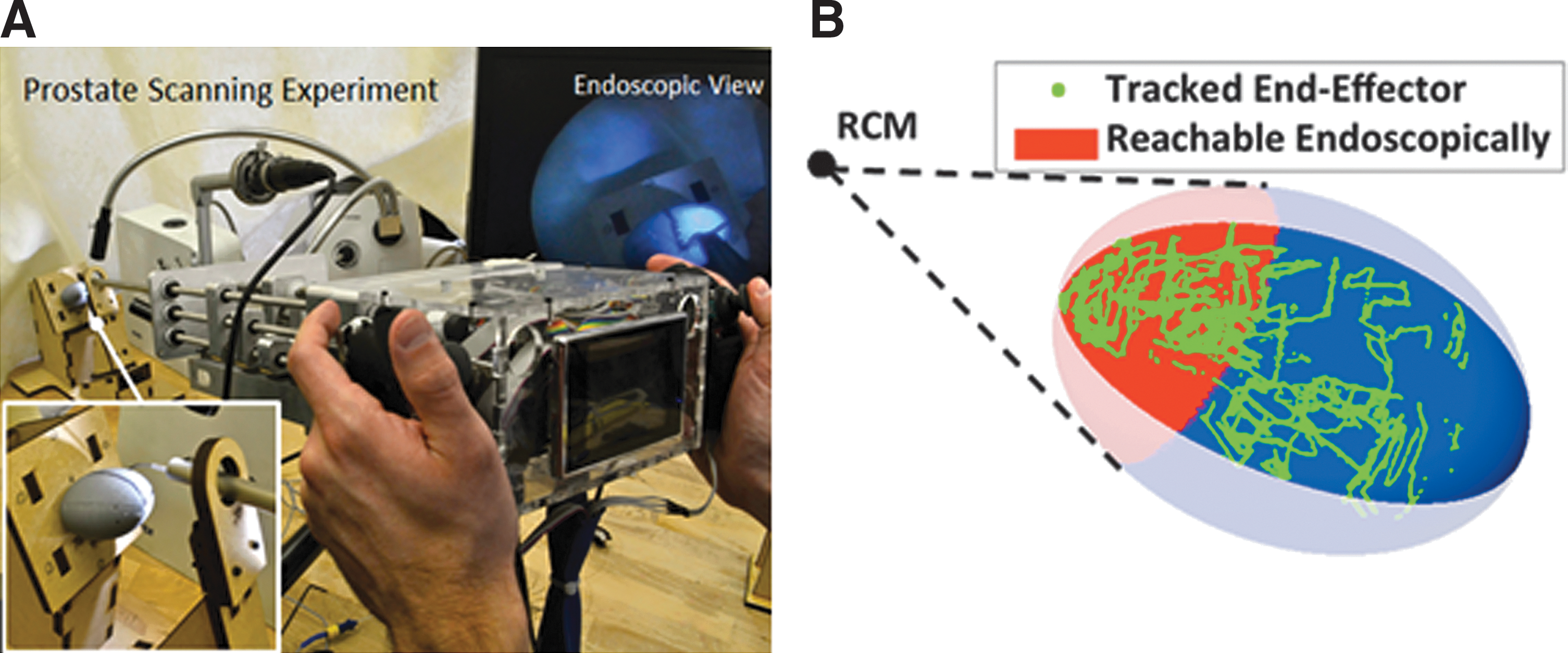
After robot development, we sought to investigate the motion of the concentric tube robots compared with the end effectors that are passed through a rigid resectoscope. To that end, a model was developed in which an ellipsoid with dimensions similar to a prostate (30 × 42 × 47 mm) was affixed to a wooden platform. The endoscope was passed through a rigid mount to serve as a center of motion, similar to that encountered when passing a rigid scope through the genitourinary diaphragm. An Aurora electromagnetic measurement system (Northern Digital, Inc.) was utilized to perform electromagnetic tracking of the tip of the concentric tube manipulator, with a location considered to be successfully scanned if the cannula tip was 2 mm or less from the surface of the prostate model. Two experienced urologic surgeons then scanned the surface of the model to compare the ability of the robot to reach various areas of the prostate model vs a standard rigid instrument without tissue deformation (Fig. 5A). Next, we performed laser resection of a prostate phantom to assess the ability of the robot to function within the confines of a simulated male urethra. We utilized the commercially available TruLase HoLEP Simulator (TruCorp Ltd.), which is an anatomic representation of the male penile and prostatic urethra with synthetic prostate lobes that are able to be lasered in a fluid environment. Lastly, we performed a feasibility study for lateral lobe enucleation of a human cadaveric prostate. A prostate and bladder specimen was harvested from a fresh male cadaver with care taken to preserve a long urethra stump. A custom fiberglass mount was constructed to secure the specimen, such that the robot could be placed within the prostatic urethra. This mount allowed for the prostate to be kept in a fixed position while allowing the bladder to freely fill and empty.
Results
Experimental results are shown in Figure 5B. A total of eight trials with the robotic platform were performed with results of reachable surface area calculated and used for analysis. The surgeons were able to consistently scan a greater surface by using the robot compared with the best case scenario reachable by a conventional straight endoscope, without tissue deformation. This was calculated by using tangent lines to the ellipsoid that pass through the fixed center of motion for the endoscope. The area reached by the robot represents a 65% improvement vs the area accessible by a rigid endoscope. This experiment showed that the robot was capable of reaching anatomically relevant locations for prostate enucleation without requiring tissue deformation to achieve these tasks. This finding is clinically relevant, as these same locations would not be accessible with a standard resectoscope aiming at a holmium laser fiber without significant manipulation of the prostate tissue.
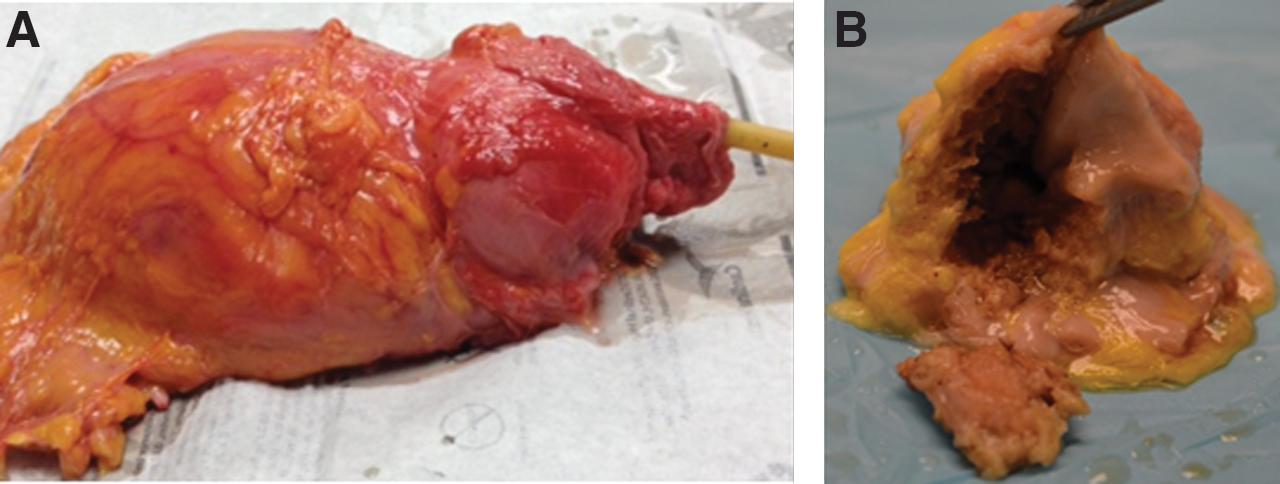
Next, the TruLase HoLEP simulator was used to attempt prostate lobe enucleation by using two concentric tube manipulators. A 550 μm holmium laser fiber was passed through the inner lumen of the right manipulator, and the left manipulator was available for exposure/retraction. The robot performed well within the working space of the prostatic urethra, as there was sufficient room for the manipulators to be maneuvered freely. Prostate lobe enucleation was successfully completed in a similar fashion to standard HoLEP; however, less exposure/enucleation with the beak of the scope was utilized when using the robot. With the robotic platform, the additional working element proved valuable, as the left concentric tube manipulator was used to provide exposure for the laser to be directed toward the desired location (Fig. 6). We found that very little gross manipulation of the robot was required, as the steerable manipulators could easily access a broad range of locations within the prostate. Finally, we attempted a proof-of-concept experiment for prostate lobe enucleation of a human cadaveric prostate. Ultimately, we were able to complete successful enucleation of the left lateral lobe, which was subsequently displaced into the bladder, similar to HoLEP. The final specimen after gross sectioning is shown in Figure 7. A sizeable defect was created in the left lateral lobe, with the enucleated tissue remaining as one single piece. Again, we found that coordinated movements of the end manipulators of the robot made exposure of the laser targets possible.

Discussion
We developed a novel concentric tube robot designed for transurethral prostate surgery that is capable of performing complex movements of the end effectors within a small working space. We believe that our initial work has shown that this robot has the ability to effectively perform tasks that could potentially decrease the technical challenges encountered during laser enucleation of the prostate.
Multiple randomized trials have shown that HoLEP is at least comparable to TURP, open simple prostatectomy, and Greenlight laser photo selective vaporization of the prostate. 3,17 –20 However, HoLEP remains underutilized and comprises only a minority of surgeries performed for BPH. Using the National Surgical Quality Improvement Program Database, Bhojani and colleagues. recently found that HoLEP only comprised 1.6% of surgeries performed for BPH. 21 Although the reasons for the apparent underutilization of HoLEP are likely complex, a recurring explanation cited in the literature is the steep learning curve associated with the procedure. 6 –10 Furthermore, intraoperative challenges such as the small working space and complex movements of the resectoscope required likely play a role. We believe that with robotic assistance, the distal dexterity and complex movements achievable by the end effectors will help alleviate some of these challenges. We have shown that with the new robotic platform, one arm can be used to retract the prostate tissue, whereas the other arm is able to precisely direct the laser fiber. Additionally, the curved configuration of the concentric manipulators allows access to more areas within the prostate with less need to grossly maneuver the endoscope. Importantly, the handheld nature of the robot allows for a similar workflow that is currently utilized during HoLEP and we have found that the same surgical principles for enucleation remain applicable with use of robotic assistance. We believe that this would help create a smooth transition into clinical practice should this technology prove to be valuable for performing HoLEP.
Our initial work to develop a transurethral robot has produced encouraging results; however, many areas for improvement have been identified. We plan to significantly decrease the size, weight, and profile of the next-generation robot. Accordingly, we anticipate that the counterbalanced arm would no longer be required in the future. Furthermore, we have found that the 6° lens within the nephroscope, while providing excellent visualization for median lobe and apical dissection, is suboptimal for working on the lateral lobes. These finding have led to planned design modifications for future versions of the robot. Ultimately, we plan to pursue comparative studies of robotic vs standard HoLEP in future studies involving live models. We acknowledge that our work remains very preliminary and far from reaching clinical utilization at this time.
Conclusions
We report a novel transurethral concentric tube robotic platform that is capable of performing complex movements of the end effectors. We have shown that these movements of the concentric manipulators are capable of performing tasks that may eventually translate into improved ease of performing HoLEP.
Footnotes
Author Disclosure Statement
No competing financial interests exist.