
Abstract
Introduction:
Recently, the role of “live” surgical broadcasts (LSB) as an educational tool to demonstrate surgical techniques at conferences has been challenged, with concerns surrounding the well-being and safety of the patient as well as the surgeon. There have been notions that “as-live” surgical broadcasts (ALSB), prerecorded unedited videos showing either the whole procedure or key features, may be educationally superior. Our study was hence conducted to determine which was deemed better by a diverse group of international urologists.
Methods:
All participants of the World Congress of Endourology held in October 2015 in London were invited to complete an electronic survey using the conference app regarding LSB demonstrations compared with ASLB, before the congress and again after the congress. Only ALSB videos were used in the congress.
Results:
Both pre- and postconference surveys showed that 76.9% and 78.2% of the participants, respectively, perceived that more teaching could be achieved in less time using ASLB. 52.8% and 60.3% of respondents indicated ALSB as being superior to LSB before and after the conference, respectively. Furthermore, 52.8% and 54.5% of respondents regarded ALSB videos as having more educational value than LSB before and after the conference, respectively.
Conclusion:
There was little perceived difference between ALSB and LSB, showing that ALSB are at least noninferior as an educational tool. In view of the numerous ethical and logistical issues with LSB, we would advocate ASLB as the educational tool of choice for future surgical demonstration at conferences.
Introduction
T
In recent times, advances in telecommunication and information technology have enabled surgery to be broadcasted in real time. Such surgical broadcasts are known as “live” surgical broadcasts (LSB). Shimizu and colleagues first described the use of LSB across international borders, broadcasting high-definition live surgery from an operation theatre in Seoul, Korea, to a surgical congress in Fukuoka, Japan, in 2007. 2 Marescaus described the first telesurgical operation with the surgeons based in New York, USA, while the patient was in Strasbourg, France, using a Zeus surgical robot in 2001. 3
The use of LSB remains popular in surgical conferences and frequently the highlight of the meeting. 4 The opportunity to view a world-renowned expert in a field at work, or to see first-hand an innovative new technique, is understandably one that surgeons seldom turn down. Furthermore, such LSB also create a platform to educate a large audience and for expert moderators to peer review their surgical methods and techniques. 5 Finally, spectators of LSB could also watch and learn how an expert makes impromptu decisions in overcoming unplanned complications intraoperatively in a pressured environment. 6
However, the wisdom and safety of LSB have recently been called into question. A patient in Japan whose cardiothoracic surgery was broadcast live died subsequently. 7 In addition, an Indian patient also died while undergoing a live laparoscopic liver surgery. 8 Hence, there have been questions raised about the ethical use and the true educational value of LSB. 5,8 –12 It is interesting to note that a recent study performed by Duty and colleagues revealed that more than 70% of the American Association of Genito-Urinary Surgeons members would not consent to be a patient in LSB. 13
Today, a number of medical associations such as the American Association for Thoracic Surgery, the American College of General Surgeons, and the American College of Obstetrics and Gynecology have ceased LSB in their conferences. 14 Moreover, although the Royal College of Surgeons, the Japanese Society for Cardiovascular Surgery, the Japanese Society for Vascular Surgery, the Japanese Association for Thoracic Surgery, the American Urological Association (AUA), and the European Association of Urology (EAU) have not prohibited the use of LSB, they have placed strict regulations on using LSB in conferences. 15 –19
Smith 20 and Philip-Watson and colleagues 9 have explored the use of prerecorded unedited videos, called “as-live” surgical broadcasts (ALSB). These show either the whole procedure or salient features as alternatives to LSB in surgical conferences. As clearly described by Smith, ALSB may be superior to LSB, as ALSB not only overcome many of the ethical issues associated with LSB and patient safety but may also be a better educational tool. Unlike LSB, ALSB can be paused at various key points of the procedure for questions, with the added benefit that the surgeon will be able to answer with full concentration, not distracted by the simultaneous requirements of performing surgery. 20 Similarly, these crucial parts of the procedure can be played repeatedly until the audience has had all questions answered.
To our knowledge, there has not been any published literature in urology regarding the use of ALSB vs LSB. We describe a novel study gathering surgeon thoughts on ALSB during the World Congress of Endourology 2015 in London.
Methodology
A congress-dedicated iOS and Android app were developed for the World Congress of Endourology held in London from October 1, 2015, to October 4, 2015. At the registration booths, all participants were encouraged to download the app onto their smartphones and tablets. Subsequently, participants were then invited to complete an electronic survey through the conference app regarding LSB demonstrations compared with ALSB videos before the congress and again after the congress.
There were 15 questions in the survey: 1. Have you observed a live surgical demonstration at a congress previously? 2. I watched live surgical demonstrations (at congress and in general) to: a. Watch a complicated procedure perform safely b. Watch how other surgeons operate c. Learn a new approach/technique to a conventional procedure d. Learn new intraoperative tricks/tips e. Watch an intraoperative complication or difficulty f. Learn how to manage intraoperative complications g. Be able to contribute new ideas for the operation surgeon if he/she is unsure on what to do next h. Be able to ask the surgeon questions i. Critique the surgeon's skills j. Reflection on my own practice 3. Do you believe that more teaching can be achieved in less time with ALSB compared with “live” surgery broadcasts? 4. Which mode of surgical demonstration do you think is more educational? 5. How do you rate ALSB vs LSB? 6. Would you be the patient for “live” surgical broadcast?
Throughout the 4-day congress, three urolithiasis procedures, six treatments for benign prostate hyperplasia, and five robotic surgery ALSB videos were presented.
A two-tailed Fisher's exact test was used to calculate the statistical difference between the pre- and post-congress opinions.
Results
In total, there were 1940 delegates at the WCE 2015.
Before the congress, there were 222 responses. However, 10 responses were disregarded because they answered the questions more than once. One hundred ninety (89.6%) respondents indicated that they have observed a live surgical demonstration at a congress before, while 22 (10.4%) respondents claimed that they had not. After the conference, a total of 166 responses to the post-congress survey were received. Ten responses were invalid as they answered the questions more than once.
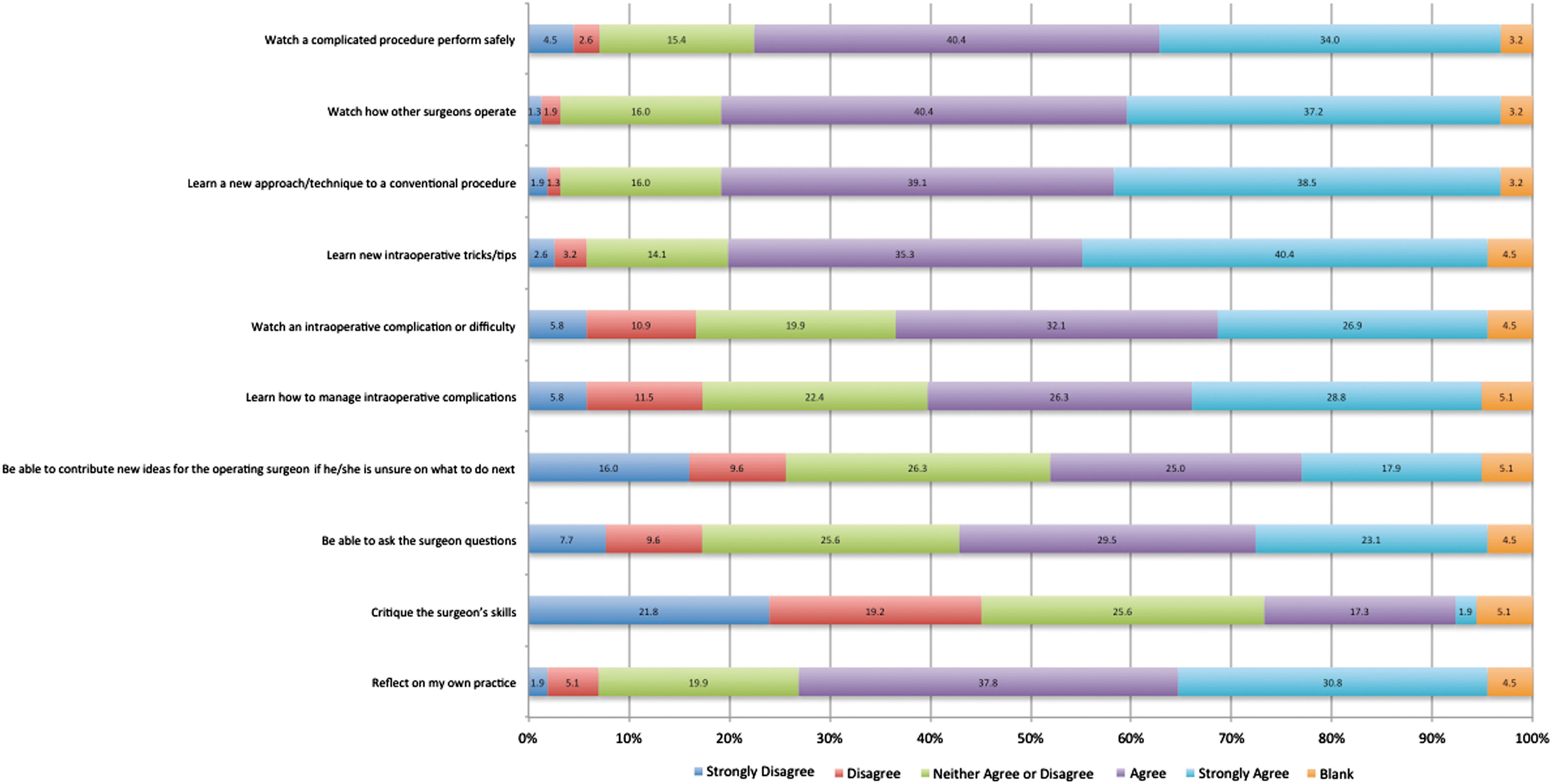
The reasons why respondents wanted to watch LSB and their previews (Fig. 1) and postviews (Fig. 2) are tabulated below:

Reasons why respondents wanted to watch LSB preconference. LSB = “live” surgical broadcasts.
Reasons why respondents wanted to watch LSB postconference.
The majority of the cohort pre- and postconference indicated that the reasons for attending LSB were to watch a complicated procedure performed safely, to watch how other surgeons operate, to learn a new approach/technique to a conventional procedure, to learn new intraoperative tricks/tips, to be able to ask the surgeons questions, and to reflect on their own practice.
After the exposure of ALSB during the conference, more respondents believed that more teaching could be achieved in less time with ALSB (Fig. 3).

Do you believe that more teaching can be achieved in less time with ALSB compared with LSB? ALSB = “as-live” surgical broadcasts.
There was no difference in views that ALSB are a more educational tool than LSB before and after the conference (Fig. 4).

Which mode of surgical demonstration do you think is more educational?
There was minimal difference in views that ALSB are better than LSB before and after the conference (Fig. 5).

How do you rate ALSB vs LSB?
The preconference survey revealed that 60.4% of the respondents would not subject themselves as patients in LSB (Fig. 6).

Would you be the patient for LSB?
Discussion
The use of LSB remains an intensely polarizing subject in the surgical community, with avid proponents and opponents of its continued use. There have been relatively few reported catastrophes during LSB, 7,8 but the live aspect of the procedure has been implicated as a direct cause of the poor outcome. In the cited case 8 above, a laparoscopic procedure that was clearly running into complications was not converted to an open procedure, despite repeated urging from the audience. Others, however, cite evidence that the long-term outcomes of patients undergoing live surgery are still excellent in other specialties. 21 –24
In the preconference survey, 76.9% of the respondents thought more teaching could be achieved in less time with ALSB. The percentage increased slightly to 78.2% in the postconference survey, suggesting that the perception of the participants on ALSB had not changed much after being exposed to ALSB. After the exposure to ALSB in the conference, a total of 60.3% respondents indicated ALSB as being superior to LSB vs 52.8% respondents who felt that way before the conference (p = 0.05). Furthermore, comparing the educational values of ALSB and LSB, there was a nonsignificant increase of respondents from 52.8% to 54.5% who regarded ALSB videos as having more educational value than LSB.
One of the interesting points gathered during the survey was that 22.6% and 28.2% of the respondents pre- and postconference indicated that their reason for watching LSB was to be able to critique the operating surgeon's skills.
In recent studies, Duty and colleagues found that more than 70% of the American Association of Genito-Urinary Surgeons members, 13 while Elsamra and colleagues found that 58% of the delegates in AUA 2012 national meeting in Atlanta, USA, and the second International Challenges in Endourology (CIE) meeting in Paris, France, would not subject themselves or their family member as patients in LSB. 12 Similarly, in our study, the pre-congress survey revealed that 60.4% of the respondents would not subject themselves as patients in LSB. However, contrary to what we would have expected, the percentage dropped to 32.1% after the conference in our survey. We could only speculate that respondents were anticipating they would participate in an ALSB video and thus felt “safer” if indeed their procedure were to be recorded to be shown later as ALSB videos. Perhaps the surgeon respondents appreciated that ALSB are theoretically technically safer than LSB, as the operating surgeons are operating in their home theatres, abolishing factors such as the need to overcome tiredness and jetlag and operating in an unfamiliar theatre environment with unfamiliar team members and unfamiliar equipment, which are faced by visiting operating surgeons in LSB.
During the congress, there were several plenary sessions on debates between LSB and ALSB. The moderators asked which mode of broadcasts the audience preferred. Unfortunately, the data from these plenary sessions were not saved, and hence, we were not able to retrieve those results and compare them to our survey.
Elsamra and colleagues had previously surveyed 253 urologists in live surgery sessions at the AUA and the second CIE meeting in Paris, France, in 2012. 12 In their survey, they found that 61% and 72% of the respondents felt that the opportunity to ask questions and having access to full unedited demonstrations as the key benefits of live case demonstrations over recorded case demonstrations. In comparison, our survey showed that 31.1% “agreed” and 21.2% “strongly agreed” before the congress, while 29.5% “agreed” and 23.1% “strongly agreed” after the congress that the key reason for them to watch LSB was the ability to ask questions.
Furthermore, Elsamra and colleagues found that 78% of the respondents also felt that live case demonstrations were ethical. 12 Similarly, Salami and colleagues also found 79% of their respondents considered LSB ethical as well. 25 More interestingly, 95% of the respondents in the study also indicated that they would agree to participate in other LSB.
Khan and colleagues did a survey on how surgeons felt when they were performing LSB. 26 They found that visiting surgeons felt significantly more anxious when they were operating in an unfamiliar operating room with a foreign team as they had to overcome various factors such as jetlag, different scrub teams, different assistants, different equipment, and language barrier to perform LSB. Furthermore, as mentioned by Chowbey and Smith, the operating surgeon is distracted by the constant dialogue between the surgeon and the audience during LSB. 4,20 The same reasons have also been found in the survey conducted by Salami and colleagues. 25
More often than not, visiting surgeons do not remain after conferences to look after the patients on whom they have operated. If these patients develop any complications, it is the local team, devoid of the experience of the responsible surgeon that has to deal with the resulting problem. Indeed, as mentioned by Smith, 16 the visiting surgeon seldom learns about their patient's complication as the conference organizers often do not wish to disturb or upset the guest visiting surgeon.
Given the controversy surrounding LSB, it is not surprising that several medical associations such as the American Association for Thoracic Surgery, the American College of General Surgeons, the American College of Obstetrics and Gynecology, and the Japanese Association of Urology have banned LSB from their conferences. 13 Despite the controversy surrounding LSB, the Japanese Society for Cardiovascular Surgery, the Japanese Society for Vascular Surgery, the Japanese Association for Thoracic Surgery, the AUA, and the EAU have elected to continue the practice although under an extensive set of strict guidelines. 16 –19 To air LSB in EAU conferences, operating surgeons need to adhere to the 31 criteria, which include surgeon selection, patient selection, preoperative planning, preoperative checks, and postoperative care. Interestingly, as part of the programme in EAU Robotic Urology Section (ERUS) meetings, the convener presents the outcome on all the LSB patients who were operated in the previous meeting. 27 Thus far, to our knowledge, ERUS has not reported any detrimental outcome on the patients who underwent LSB.
Philip-Watson and colleagues explored the ethical issues and dilemmas of LSB extensively. 7 While LSB are recognized as an impactful teaching tool, surgeons should not put educational benefits above patients' safety. They made several recommendations to reinforce this notion, such as having an independent surgeon who will act in the best interest of the patient and have the power to stop the case at any time, and a detailed and dedicated consent form for LSB patients. The authors suggested the use of ALSB as an alternative effective educational tool to LSB. Not only does it remove all the aforedescribed performance factors such as overcoming jetlag, operating in a different environment, operating with different scrub teams and assistants, and using different equipment, which invariably might affect the outcome of the operations, ALSB also offer an enhanced learning experience as they can be paused at various key points of the procedure so that the audience can ask the surgeon additional questions, which he/she will be able to answer with full concentration and not distracted by the simultaneous requirements of performing surgery. Furthermore, as Smith has mentioned, specific sessions regarding the management of intraoperative complications could be held through the usage of ALSB, in which such complications were noted and managed effectively. 16
Leavitt and Kavoussi believed that LSB still have advantages over ALSB, such as LSB are still the only educational modality that could demonstrate a surgeon's intraoperative decision-making, which could not be replicated in ASLB. 6 However, they have called for strict guidelines to be set in place in various conferences such as what EAU has done to use ensure that LSB can be safe for patients and educational for other fellow surgeons. Similarly, this sentiment has also been echoed by Salami and colleagues. 25
Our study has several limitations. First, the response rate to our survey was low. Of the 1940 attendants, we only managed to gather 212 responses (10.9%) to the pre-congress questionnaire and 156 (8.0%) after the congress. The lower response rate after the congress was likely because some attendants had left the congress before it ended. Second, there is a huge selection bias involved in this survey. We could only speculate that attendants who are genuinely strict on ethics or those who prefer ALSB are more likely to respond to this survey. Another major limitation of this survey is that there were no LSB shown in WCE 2015. Therefore, delegates were not given an opportunity to make a fair comparison between LSB and ALSB. Our survey was not able to identify the respondent's demographics, subspecialties, region of their practice, and so on. It would be interesting to analyze if their backgrounds have any influence on their responses. Last but not least, it would have been ideal to have all parts of the survey answered; some respondents, however, elected to leave parts of the questionnaire response blank, thereby making objective analysis of all the parameters being evaluated somewhat difficult.
Conclusion
The results of our survey suggest that even before exposure to ALSB, the majority of surgeons sampled felt that ASLB had greater educational value than LSB, and could achieve more teaching in a shorter period of time. These perceptions were reinforced after exposure to ASLB during the world congress. If, from an educational perspective, ALSB are considered equivalent or superior to LSB, then what is the justification for continuing with LSB regardless of restrictions and precautions?
Footnotes
Author Disclosure Statement
No competing financial interests exist.