
Abstract
Radiological imaging remains the cornerstone of follow-up of patients with urolithiasis. Plain abdominal X-ray (XRKUB) of these patients is largely becoming obsolete in favor of noncontrast computed tomography of the abdomen and pelvis (CTKUB), which offers superior sensitivity and specificity. Contentiousness exists, however, related to the radiation doses associated with CT. Calcium oxalate remains the most common stone composition across most populations. These calculi are radiopaque and thus follow-up with XRKUB may be appropriate in some settings, avoiding the higher radiation doses associated with standard protocol CT. With the emergence of low-dose CT, however, and the modest accuracy of XRKUB, the ongoing role for XRKUB in the management of urolithiasis is debatable. In this study, we assessed the proportion of pure calcium urolithiasis visible on XRKUB to assess the utility of XRKUB for follow-up of pure calcium urolithiasis. Hospital laboratory databases were analysed to identify patients who had undergone urological intervention and extraction of urolithiasis composed of pure calcium salts, who had undergone CTKUB and XRKUB during the same episode for diagnosis of the calculus. One hundred five calculi were included and the imaging for each patient analyzed. 79/105 calculi (75%) identified on CT were visible on XRKUB. The median calculus visible on XRKUB was 7.0 mm (interquartile range [IQR] 5.0–10.0 mm), the median calculus not seen was 4.25 mm (IQR 3.5–7.0 mm) as measured on CT (p < 0.01). XRKUB accuracy varied according to calculus position within the renal tract. Calculi were most often visible in the renal pelvis and proximal ureter (86%), 50% of mid-ureteral and 72% of distal ureteral calculi were visible (p = 0.01). Until low-dose CT protocols become widely adopted, XRKUB still has a limited role in the management of pure calcium urolithiasis in selected patients. Due to its modest accuracy in many settings, this role is limited mainly to larger proximal urolithiasis.
Introduction
U
Objects and anatomical structures composed of calcium compounds can be readily viewed on X-ray (XR). Urolithiasis composed of noncalcium-containing compounds such as uric acid and cysteine is radiolucent on XRKUB, and therefore, other forms of imaging are required for diagnosis and follow-up of such calculi. Calcium oxalate remains the most prevalent urolithiasis composition across most populations, and these calculi, as well as those composed of other calcium compounds, such as calcium phosphate, are visible on XRKUB in the absence of an obstructing artifact or other tissues obscuring view. 9,10
Effective radiation exposure from XRKUB is lower compared with standard protocol CTKUB (0.04–1.1 mSv vs 3.5–25 mSv), and for this reason, XRKUB is an attractive option for the follow-up of calcium urolithiasis in selected patients. 11 XRKUB is also a lower cost, faster, and more accessible modality of imaging in comparison to CTKUB. The cost of a single CTKUB varies across different healthcare systems, but exceeds five times that of an XRKUB in the Australian healthcare system. 12 XRKUB is, however, far inferior to CTKUB in terms of sensitivity and specificity for identification of urolithiasis. 13
We aimed in this study to identify the proportion of urolithiasis, composed of pure calcium salts, visible on CTKUB that are also visible on XRKUB, to assess the feasibility of using XRKUB alone for the follow-up of known calcium urolithiasis.
Materials and Methods
Pathology databases from two hospitals were searched to identify patients who had undergone urological intervention and extraction of urolithiasis, which was subsequently confirmed to be composed of pure calcium salts, following laboratory analysis. Calculi were deemed “pure calcium” if they were composed of >85% of the calcium salt, and such calculi were included in the study. All other calculi were excluded. Imaging from all the remaining patients was then reviewed. The acquisition of these data, and their subsequent analysis, did not require human research ethics committee (HREC) review on the basis that the project was categorized as a quality activity in accordance with the definition of research outlined in the Australian National Statement. An HREC number was provided for publication purposes, HREC/15/QGC/220.
Patients who had both a CTKUB and XRKUB at first presentation to hospital were included, and all others were excluded. In each case, an XRKUB was carried out as the initial radiological investigation following presentation to the emergency department with acute abdominal pain, and a CTKUB was performed within the subsequent 4 hours. XRKUB for each patient was reviewed, with the reviewer having prior knowledge of the size and the side of the calculus, as one would if reviewing a follow-up image. The reviewer, however, had not viewed the CTKUB. Two separate reviewers independently reviewed each image. In the setting that the independent assessments were discordant, the reviewers reviewed the images together and consensus was reached. Reviewers included two urologists, two radiologists, and two urology trainees. It was noted whether or not the calculus was visible on XRKUB, and the position in the urinary tract was also noted. The CTKUB was then reviewed separately, the size of the stone was measured and the position recorded. Findings from the XRKUB and CTKUB for each patient were compared. Positioning in the ureter was divided into three categories; proximal ureter/renal pelvis, mid-ureter, and distal ureter. These were defined as follows: proximal ureter was measured from the renal pelvis to the top edge of the sacrum, the mid-ureter from top edge of the sacrum to the lower edge, and the distal ureter measured from the lower edge of the sacrum to the bladder. HU value of each calculus was calculated from the CTKUB.
Differences between patients with visible calculi and those without were analyzed with the chi-square test for categorical variables or the Wilcoxon rank-sum test for continuous variables due to expected deviations from normality of the explanatory variable. Tests were two sided with significance set at 0.05. The relationship between XRKUB visibility and the continuous variables of stone size and HU value was expressed graphically using a scatterplot with overlaid predictor line and 95% confidence interval derived from a univariable logistic regression. Analysis was performed using Stata v.12.0 SE, College Station, TX.
Results
In total 105 patients met the inclusion criteria. Seventy-nine (75%) of these patients had a visible calculus on XRKUB. As all patients had a calculus visible on CTKUB, this value represents the sensitivity of XRKUB compared to CTKUB. The majority of patients were male (73%) and the greater proportion had stones in the proximal third of the ureter (48%). Details of the patient cohort are shown in Table 1.
p-Value indicative of difference in characteristics between the two groups.
Eighty-four patients with these data available. No difference in missing data between visible and not visible groups (p = 0.7).
IQR = interquartile range; XR = X-ray; XRKUB = X-ray of the kidneys, ureters, and bladder.
No difference in the stone visibility on XRKUB was observed for male versus female patients. There was a statistically significant difference in XRKUB sensitivity observed according to position in the renal tract (p = 0.012). Calculi were most often visible in the renal pelvis and proximal ureter (86%), followed by the distal ureter (72%). Only half of mid-ureteral calculi were visible on XRKUB.
As expected, larger calculi were more frequently visible on XRKUB. The median calculus seen on XRKUB was 7.0 mm, and the median calculus that was visible on CTKUB, but not seen on XRKUB, was 4.25 mm as measured on CTKUB (p < 0.001). The relationship between XRKUB visibility and stone diameter is illustrated in Figure 1. The predicted visibility on XRKUB for 5 mm stones is 68% (95% CI 58%, 79%), which increases to 85% (95% CI 76%, 95%) for 10 mm stones. The predicted XRKUB visibility for a 500 HU stone is 62% (95% CI 47%, 76%) (Fig. 2), but this rises to 91% (95% CI 82%, 99%) for 1000 HU stones.
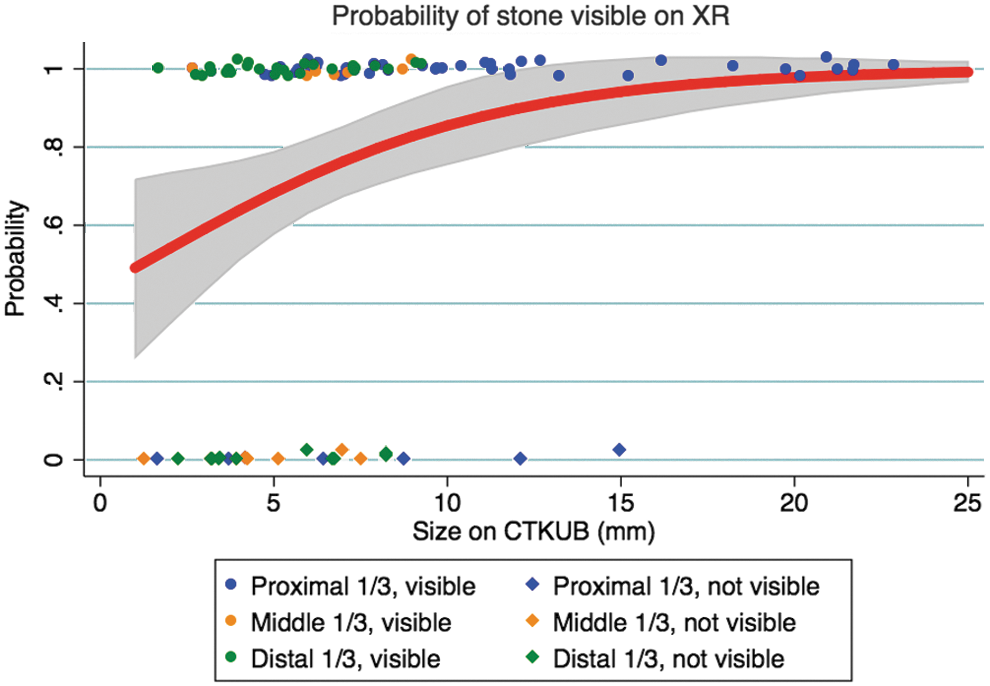
Probability of stone visibility on XRKUB vs stone size as measured on CTKUB. Red line indicates a predicted visibility probability with gray 95% confidence interval. XRKUB = X-ray of the kidneys, ureters, and bladder.
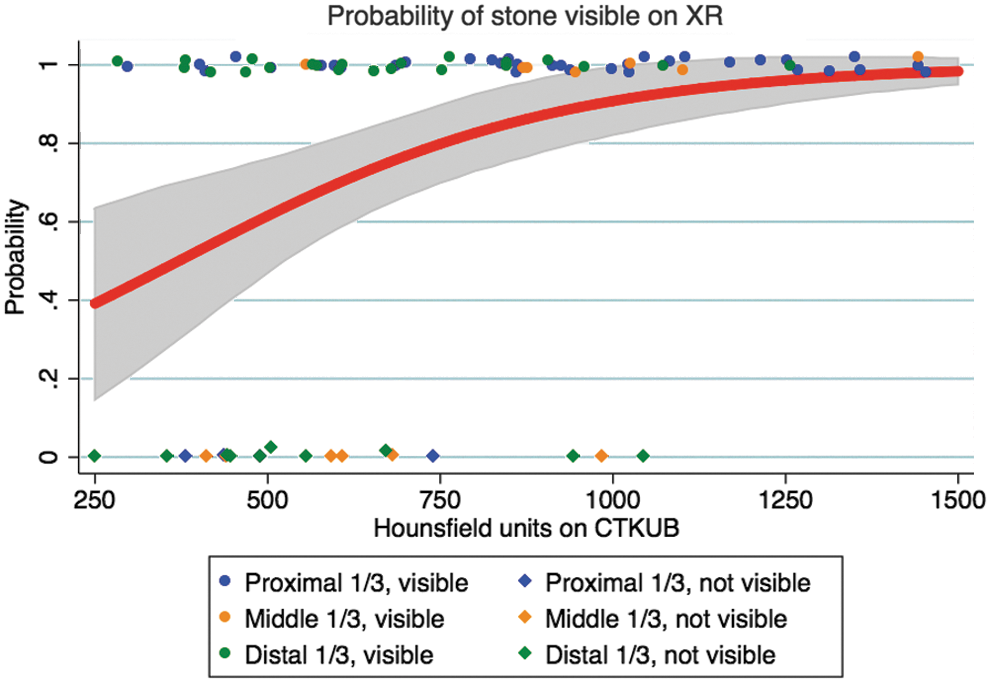
Probability of stone visibility on XRKUB vs HU value on CTKUB. Red line indicates a predicted visibility probability with gray 95% confidence interval.
All stones >10 mm were located in the proximal third of the ureter or renal pelvis, and this contributes to the finding of proximal stones being more visible on XRKUB. However, the positive relationship between size and visibility described in Figure 1 holds when stratified by stone position (Fig. 3). Although for any given size, a stone in the middle third of the ureter is less visible on XRKUB than one in the upper or lower third. The predicted XR visibility for a 5 mm stone is 78% in the proximal ureter, 71% in the distal ureter, but only 41% in the middle ureter.
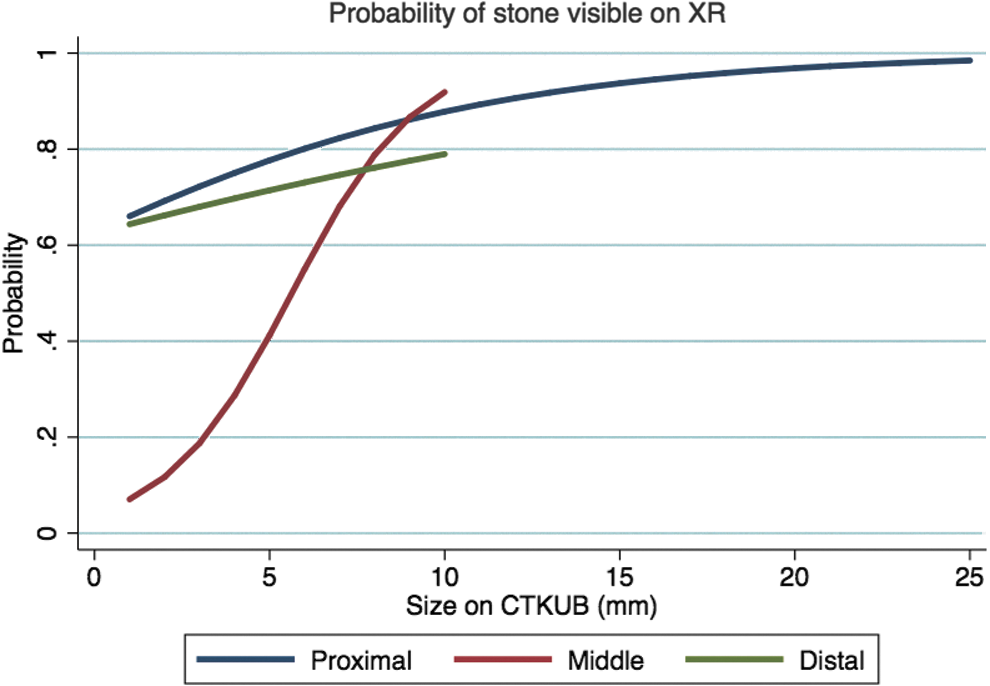
Probability of stone visibility on XR vs stone size as found on CT stratified by subsequently noted stone position. All lines are the predicted visibility probability from individual univariable logistic regressions.
Discussion
XRKUB is still commonly adopted as the initial radiological examination for the investigation of acute abdominal pain, including that caused by urolithiasis. Some authors have disputed the utility of XRKUB in this context, and studies have suggested that XRKUB as an initial diagnostic investigation rarely changes patient management in the setting of acute abdominal pain. 14 Some argue that baseline XRKUB in the setting of urolithiasis identified on CTKUB, even after reporting of a CT scout film, can aid with the interpretation of subsequent XR follow-up imaging, and therefore should be recommended. 15 XRKUB is commonly used for the follow-up of known calcium urolithiasis, although its modest reported sensitivity leads some clinicians to abandon this modality in favor of more sensitive options such as CTKUB. CTKUB has excellent sensitivity and specificity for the diagnosis of urolithiasis, and as a result, it is widely utilized for this function. 16 CTKUB, however, is associated with a higher radiation exposure dose than XRKUB, if low-dose protocols are not adhered to, and it has been shown that only a small percentage of hospitals in the United States utilize low-dose or ultralow-dose CT protocols for investigation of urolithiasis. 17,18 The increase in numbers of CT images performed worldwide has been marked in the last decade, and some authors have signaled this as a significant public health concern. 19,20 Fallout from nuclear disasters has provided data highlighting the risk of carcinogenicity related to radiation exposure above threshold levels. 21 CTKUB is also a more costly and time-consuming imaging modality when compared to XRKUB. USKUB is another commonly utilized imaging modality for the follow-up of urolithiasis, but it is also subject to limitations. The ability of USKUB to observe mid-ureteral urolithiasis is a major limitation. Surrogate markers suggesting the presence of urolithiasis can be used, such as presence of hydronephrosis, but such markers have not proven to be completely reliable. 22 USKUB is also a more labor-intensive investigation and associated with operator variability. XRKUB in certain clinical contexts may be appropriate and where utilized appropriately can result in lower radiation exposure to the patient and lower cost and time burden on healthcare systems.
The inferior sensitivity and specificity of XRKUB for the diagnosis and follow-up of urolithiasis when compared with CTKUB in particular is well documented. Sensitivity of XRKUB to identify urolithiasis has been reported to be as low as 45% to 58%. 23,24 XRKUB has no utility in visualizing uric acid or cysteine stones and is limited for visualization of variant calcium urolithiasis. However some of the literature on this topic may be misleading in the context of follow-up of known calcium urolithiasis. Studies investigating the utility of XRKUB as a stand-alone diagnostic tool in urolithiasis have correctly reported low sensitivity, however, radiolucent stones and variant composition stones are included in the analyses of such studies. Studies reporting the accuracy of XRKUB for all urolithiasis are confounded by the prevalence of noncalcium-based urolithiasis in the study population. A major limitation of XRKUB in this context is that variable stone compositions are ubiquitous and often involve the combination of a calcium salt with a radiolucent compound such as uric acid. 25 This means that although calcium oxalate is the most common compound seen in urolithiasis across the globe, the relative proportion and distribution of the calcium salt present in a given urinary tract calculus will greatly affect the radiopacity of the calculus on XR. Furthermore, calculi that are composed primarily of calcium are not always visible on XRKUB. The presence of anatomical structures such as the vertebral column and boney pelvis, as well as overlying bowel contents and other artifacts, may obscure the view of an existing urinary tract calculus.
Stone-specific as well as patient-specific factors play a major role in the decision-making process for the treatment or follow-up of urolithiasis. In the setting that calculi are to be followed up radiologically in lieu of prompt urological intervention, the modality of imaging is chosen based on these individual factors. In contemporary cohorts, the initial diagnosis of urolithiasis is commonly reached with CTKUB, thus giving precise information on stone burden and positioning. 26 This information can guide decisions on appropriate modalities of radiological follow-up. HU value on CT has been used with reasonable accuracy to predict the likelihood of calcium-based urolithiasis, thereby aiding to predict the likelihood of subsequent visibility on XRKUB. 27 Such information is also attainable using low-dose CT protocols. 28 Alternatively, an XRKUB performed at the time of diagnostic CT can show definitively whether a stone is visible, thereby potentially facilitating the use of XRKUB for subsequent follow-up. XRKUB has been shown to be more sensitive than scout CT (SCT) for this function, and as such, a negative SCT does not negate the potential benefit of a concomitant XRKUB to help guide management planning. Although sensitivity of SCT imaging to identify urolithiasis has improved with modern scanners, it is still reported that such imaging visualizes only 75% of urolithiasis that are visualized on XRKUB. However, reports suggest that if a stone is observed on SCT, this can potentially negate the need for concomitant XRKUB. 29 Lamb et al., however, reported that XRKUB lead to a significant change in the management of 17% of their study cohort when compared to CT, including SCT, and this was largely related to the relative radiopacity of calculi on XRKUB and their resultant amenability to extracorporeal shockwave lithotripsy (SWL). 30 In our cohort, we found that, in fact, HU value on CTKUB was the most sensitive predictor of stone visibility on XRKUB.
When ordering plain XR imaging for follow-up of variant calcium urolithiasis, it is important for clinicians to be aware of the accuracy of such imaging to identify a stone if present. In the setting that XRKUB fails to highlight the presence of a persistent calculus, or an anatomical artifact makes for an unsatisfactory image, a patient may be subjected to further imaging and resultant delays in definitive management planning. This may lead to patient frustration and dissatisfaction, as well as inefficiencies in outpatient waiting lists, if patients have to return for further imaging following equivocal XRKUB. Such practice, although aiming to reduce patient radiation exposure by utilizing plain XR, leads to further radiation exposure when further imaging is required to confirm a diagnosis. Avoiding plain XR imaging in the setting that an equivocal result is likely may avoid unnecessary delays and wasted radiological tests. The use of oblique plain abdominal films has been suggested as a strategy to improve the accuracy of plain imaging beyond that of conventional anteroposterior XRKUB for mid-ureteral and distal ureteral calculi. 31 The accuracy of these techniques is not widely established, however, and is likely to be affected largely by patient selection and associated with many of the inherent issues with plain XR for this indication. It has been suggested that clinicians should be cautious of the fact that adjunctive XR imaging techniques such as these may lead to cumulative radiation exposure approaching or exceeding that of low-dose CT protocols. 32
It must be stressed that the findings of this study are based on “pure” calcium urolithiasis, thereby reported accuracy does not relate to all stone types. Although accuracy reported in this study may appear greater than others in the literature, these data are more applicable when considering follow-up of calculi that are known to be visible on previous imaging. We are thus reporting on the proportion of stones that “should be visible” and that actually “are visible” on XRKUB. Clinicians should be reassured that results from XRKUB for large calculi composed primarily of calcium are almost always unequivocal in the setting of a good-quality XRKUB.
This information can be used to guide further follow-up imaging or indeed treatment planning. For example, these data may support the use of XRKUB as an initial imaging modality after SWL for large proximal calculi. However, smaller calculi of the same composition may not be so definitively visible on XRKUB, and therefore, clinicians should consider carefully the use of XR in this setting and the potential need for alternative or adjunctive imaging. The question of course of whether patients with asymptomatic ureteral calculi measuring <5 mm should require follow-up imaging is much debated and is outside the scope of this article.
The authors acknowledge that this study is subject to a number of limitations, particularly given the relatively small sample size and the retrospective nature of the analysis. The requirement for an initial XRKUB before CTKUB for inclusion in this study may have introduced some selection bias into the sample studied. This may have lead to a higher proportion of patients with a more obvious clinical picture of renal colic being selected out because they bypassed an XRKUB in favor of a CTKUB, which may have appeared to be a more high-yield modality in the clinical context. This may have lead to exclusion of more distal calculi and affected the distribution of patients. Despite this, the authors feel that some very useful and clinically relevant information can be gleaned from this study, which highlights specifically the visibility of calcium stones in this clinical context, something that has not been widely reported on previously.
Conclusion
XRKUB has reasonable accuracy for urolithiasis >5 mm composed of pure calcium salts, particularly those of the upper renal tract. We suggest that the use of XRKUB alone for follow-up of large calcium urolithiasis of the upper renal tract may be used with confidence in the correct clinical setting. The radiopacity of urolithiasis on initial XRKUB or the HU value on CTKUB can help to predict the likely visibility of such calculi on follow-up XRKUB. The accuracy of XRKUB for urolithiasis <5 mm is modest, however, particularly for those in the mid-ureter. Such calculi may require alternative imaging modalities such as CT for accurate follow-up. Until the use of low-dose and ultralow-dose CT protocols become widely adopted, XRKUB still has a legitimate role in the management and treatment planning of calcium urolithiasis in selected patients. Due to the modest accuracy of this modality in many settings, however, this role is limited mainly to larger proximal stones.
Footnotes
Acknowledgments
A preliminary and condensed analysis of these data was presented at the 32rd World Congress of Endourology, and the accompanying conference abstract has been published. 33
Author Disclosure Statement
No competing financial interests exist.