
Abstract
Aim:
Wide resection of the ureteral orifice (UO) may result in scarring and stenosis of the ureterovesical junction (UVJ). We aimed to describe a technique of endoscopic spatulation of the intramural ureter in patients undergoing resection of the UO at the time of transurethral resection of bladder tumor (TURBT) and compare the surgical and oncological outcomes of this procedure with those of patients undergoing conventional UO resection.
Methods:
The clinical records of patients who underwent TURBT at a single institution were retrospectively analyzed. Patients who underwent conventional UO resection or UO resection followed by endoscopic spatulation of the intramural ureter were included in the analysis. The two groups were compared in terms of intra- and postoperative outcomes.
Results:
A total of 227 patients were included in the final comparative analyses. Of them, 104 underwent conventional UO resection and 123 underwent UO resection followed by endoscopic spatulation of the intramural ureter. The two groups were comparable for demographic and clinical features. There were not statistically significant differences in terms of mean operative times. The incidence of transient postoperative hydronephrosis as well as UVJ scarring and stenosis was significantly lower in patients undergoing endoscopic spatulation of the intramural ureter. The two groups were similar in terms of incidence of vesicoureteral reflux (VUR) and upper urinary tract cancer recurrence.
Conclusion:
Endoscopic spatulation of the intramural ureter after UO resection is a safe and quick procedure that significantly reduces the incidence of transient early postoperative hydronephrosis and late UVJ stricture if compared with UO resection alone. This procedure is quick to perform, safe, and does not increase the risk of VUR.
Introduction
B
To date, the use of pure cutting current during the resection of the UO and the avoidance of extensive coagulation are considered the only technical measures recommended to reduce the risk of scarring and stenosis. 3 Despite these technical measures, the incidence of scarring and stenosis of the UVJ may occur, and patients require careful upper urinary tract monitoring. Ureteral spatulation is described in open surgery to prevent ureteral stenosis. 4 We developed an endoscopic technique of spatulation of the intramural ureter after UO resection to prevent stenosis of the UVJ.
The objectives of this study were to describe the surgical technique and the results of endoscopic spatulation of the intramural ureter and compare the surgical and functional outcomes of this procedure with those of conventional UO resection.
Materials and Methods
We performed a retrospective comparative study. The clinical records of patients who underwent TURBT for BCa at a single institution between January 2008 and March 2015 were reviewed. Patients with BCa covering the UO or involving its close vicinity were included in the analysis. Patients with preoperative hydronephrosis, previous UO resection, previous upper tract involvement, prior ipsilateral nephrectomy, and incomplete data were excluded from the analysis.
The following variables were recorded: age, gender, number and diameter of the tumors, operative time, duration of hospital stay and catheterization, intra-, early (within 30 days from surgery) and late (>30 days from surgery) complications, pathological grade and stage, BCa recurrence, and upper urinary tract cancer recurrence. Postoperative complications were classified according to the modified Clavien–Dindo classification. 5
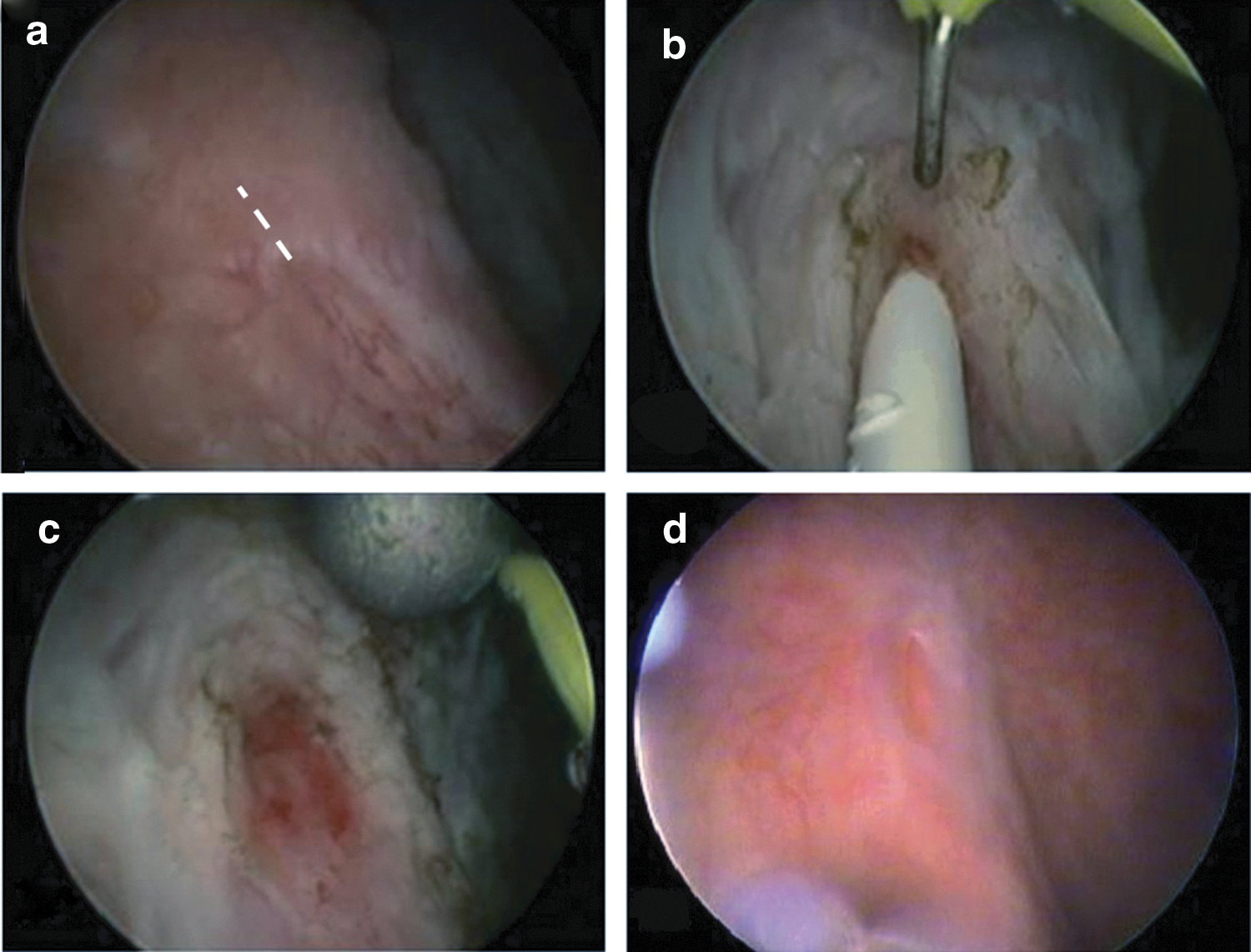
All the surgical procedures were performed by a single expert surgeon. In all cases, the UO was resected using monopolar pure cutting current. Selective coagulation of bleeding sites was performed. Since 2010, an endoscopic technique of spatulation of the intramural ureter was introduced at our institution. Briefly, a ureteral catheter is inserted before TURBT, the tumor is resected, and a Collins knife activated by a pure cutting current is used to make an incision of the intramural ureter at the 12 O'clock position (Fig. 1a–c). A ureteral stent is not placed at the end of both simple UO resection and UO resection followed by spatulation of the intramural ureter.
Renal ultrasound was performed on postoperative days 7 and 30 and then every 3 months. Computed tomography urography (with voiding cystography) was performed 1 month after surgery and then yearly. Cytological and cystoscopic evaluations were performed according to individual bladder cancer risk. The surgical and oncological outcomes of patients who underwent conventional UO resection (group 1) were compared with those of patients who underwent UO resection followed by spatulation of the intramural ureter (group 2).
Descriptive data of continuous variables are expressed as mean and range values and compared using the Student's t tests. Proportions were compared using the chi-square test or the Yates or Fisher test when appropriate. The analyses were considered significant for a p-value <0.05. All statistical analyses were performed with SPSS version 17.0 (SPSS, Inc., Chicago, IL) software. The study was performed in accordance with the ethical standards laid down in the Declaration of Helsinki. Verbal informed consent was obtained from subjects.
Results
Overall, a total of 750 patients underwent TURBT within the selected time frame. Two hundred twenty-seven patients (30.2%) met the inclusion criteria and were analyzed. Of them, 104 (45.8%) underwent conventional UO resection, and the remaining 123 (54.1%) underwent UO resection followed by spatulation of the intramural ureter. The demographic and clinical characteristics of patients are presented in Table 1. Specifically, the two groups were homogeneous for demographic and clinical features. Intraoperative and early postoperative data are depicted in Table 2. There were not statistically significant differences between the two groups in terms of operative times and length of hospital stay and catheterization.
TURBT = transurethral resection of the bladder tumor.
The incidence of complications was low in both groups, and no major complications were reported. Overall, two patients in group 1 and three patients in group 2 had intraoperative bleeding. In all cases, bleeding was secondary to extraperitoneal bladder perforation due to obturator nerve stimulation and abductor contraction. No intraoperative complications secondary to UO resection or intramural ureter spatulation occurred. Moreover, the two groups were similar in terms of BCa pathological characteristics. The need for additional therapy, including restaging procedures and adjuvant intravesical instillations, was based on pathological findings.
The incidence of early postoperative transient hydronephrosis was significantly lower in the subgroup of patients undergoing endoscopic spatulation of the intramural ureter. In all cases, this complication was managed conservatively with anti-inflammatory drugs. Mean follow-up was 63.2 months (range, 6–93 months).
Table 3 describes the incidence of late postoperative complications as well as oncological outcomes. The incidence of UO scarring and stenosis was significantly lower in the group of patients undergoing spatulation of the intramural ureter. This finding was confirmed endoscopically and radiologically. The relative odds of obstruction due to UVJ scarring indicated an 89.5% reduction of this complication in the group of patients receiving spatulation of the intramural ureter (odds ratio: 0.0984, 95% confidence interval: 0.012, 0.77; p = 0.030). All patients with UVJ stricture were treated by endoscopic surgery. No patients had permanent loss of renal function. Figure 1d shows the endoscopic appearance of the UVJ after endoscopic spatulation at 1-year follow-up.
BCa = bladder cancer; UO = ureteral orifice; UVJ = ureterovesical junction; VUR = vesicoureteral reflux.
Discussion
TURBT is one of the most common endoscopic urologic procedures. It is crucial for diagnosis and staging of BCa, and its goal is to achieve a complete tumor resection when possible.
Resection of the UO is required in as much as 35% of patients undergoing TURBT. 3 According to literature data, tumors involving the UO or its close vicinity should be treated with wide deep resection, including the entire orifice area. 3,6 –8 UO resection may result in vesicoureteral reflux (VUR) or stenosis of the UVJ, which can lead, respectively, to tumor cells seeding along the upper urinary tract or to upper urinary tract obstruction. 3 Reports specifically addressing the outcomes of patients undergoing resection of the UO are scarce.
According to available literature data, UVJ obstruction has been reported in as much as 16% of patients undergoing UO resection during TURBT (range, 0%–16%). 3,6 –13 Mano and colleagues assessed the risk of upper urinary tract obstruction and tumor recurrence following UO resection during TURBT. 3 The study included 65 men and 14 women in whom a total of 84 UOs were resected. 3 Hydronephrosis was observed in 13% of patients during a median follow-up of 15 months. Hydronephrosis was secondary to muscle invasive disease in 6% of patients, and it resolved spontaneously in 4%. 3 In the remaining patients, overt stricture was detected at the UVJ, requiring endoscopic intervention. 3
Ureteral obstruction may cause acute flank pain during early postoperative convalescence, but it may also develop insidiously during a longer period, leading to decreased renal function without preceding symptoms. 3,14 Fibrosis generally begins 3–4 weeks after surgery. 3,15 After resection of the UO, a close follow-up of patients is advisable, including upper tract imaging.
To date, the only recommendations to minimize the risk of UO scarring and stenosis include the use of pure cutting current during resection, careful “spot coagulation” of apparent bleeding sites, and avoidance of multiple coagulations of large areas. 3,6 –13 According to literature data, adjuvant intravesical therapy as well as endoscopic restaging procedures do not impact the likelihood of stricture formation. 3 Routine ureteral stenting immediately after UO resection is optional. However, its role is controversial, and it is generally avoided. 3,6 –8 According to some authors, although ureteral catheterization may prevent acute ureteral dysfunction caused by edema and spasm, it has little impact on late fibrosis and may be even harmful in some cases. 3,15
The surgical technique of ureteral spatulation is commonly used in open urologic surgery to allow wide anastomosis and thus prevent strictures. 4 Following the principles of open surgery, we adopted, for the first time, the technique of endoscopic spatulation of the intramural ureter. In our opinion, this technique may help prevent the stenosis of UVJ by widening the ureteral opening and thus avoiding its scarring.
Results from the present study demonstrate that endoscopic spatulation of the intramural ureter is associated with a significantly lower incidence of transient early postoperative hydronephrosis, UVJ scarring, and late postoperative upper urinary tract obstruction with respect to conventional UO resection. This procedure is easy to perform and does not prolong significant operative times. Moreover, it does not increase intra- and early postoperative morbidity.
Interestingly, the incidence of VUR was similar between the two groups and within the published ranges.
The incidence of upper urinary tract transitional-cell carcinoma in primary BCa patients ranges from 0.7% to 24%. 16 The incidence is strongly related to the primary tumor risk stratification. 16 The incidence is as low as 0.7% in the low-risk group followed a median of 10 years to as high as 24% in high-risk groups followed 3–4 years. 16 According to literature data, the incidence of upper tract tumor recurrence in patients undergoing UO resection ranges from 0% to 42%. 3
The role of VUR following the disruption of normal UVJ anatomy is a matter of debate. 3 It remains unclear if UO resection may confer an increased risk of tumor cells seeding along the upper urinary tract. 3 According to some authors, VUR may have even a protective role by allowing intravesical instillations to reach the upper urinary tract. 3 According to literature data, the incidence of VUR in patients undergoing UO resection ranges from 11% to 77%. The incidence of VUR in both the groups of the present study is within the published ranges. Interestingly, the spatulation of the intramural ureter does not increase the incidence of VUR. Results from the present study demonstrate a low incidence of upper urinary tract cancer recurrence without statistically significant differences among groups.
Major strengths of the present study include the originality of the procedure described, the size of the series, and the presence of a control group. Considering the high prevalence of BCa and the consequent need for TURBT in urologic practice, the results from this study have potentially relevant clinical implications.
However, some weaknesses should be addressed: The study is retrospective and not randomized. In our clinical experience, preoperative hydronephrosis is not a contraindication to endoscopic spatulation of the intramural ureter. However, patients with preoperative hydronephrosis were excluded from the present study to make more homogeneous the study population and avoid potential biases that could affect the interpretation of results. In consequence, findings from the present study cannot be extended, at this point, to patients with preoperative hydronephrosis, and further prospective randomized studies are required to confirm our findings, even in patients excluded from the present study.
Conclusions
Endoscopic spatulation of the intramural ureter after UO resection is a safe and quick procedure that significantly reduces the incidence of transient early postoperative hydronephrosis and late UVJ stricture if compared with UO resection alone. This procedure is quick to perform, safe, and does not increase the risk of VUR.
Footnotes
Acknowledgments
The study was performed in accordance with the ethical standards laid down in the Declaration of Helsinki. Verbal informed consent was obtained from subjects.
Author Disclosure Statement
No competing financial interests exist.