
Abstract
Objective:
To report a novel technique of laparoscopic retroperitoneal enucleation-separation surgery for specifically located renal angiomyolipoma (RAML) treated in our institute.
Patients and Methods:
We prospectively analyzed 40 patients who were randomized and received laparoscopic simple enucleation (Group 1) or enucleation-separation (Group 2) from January 2011 to February 2013. Patient characteristics, perioperative outcomes, renal function, and oncologic outcomes were compared between the groups.
Results:
Average age, body mass index, sex distribution, tumor location and size, and operative time showed no significant difference between the two groups (p > 0.05). Average warm ischemia time in Group 1 was longer than that in Group 2 (25.3 minutes vs 17.6 minutes, p = 0.001). No complications except for one postoperative hemorrhage that occurred in Group 1 were observed. An improved early affected renal function recovery was observed in the Group 2 (percentage of glomerular filtration rate reduction for Group 1 vs Group 2, 24.3% vs 18.3%; p = 0.001). No local recurrences were found during the follow-up period.
Conclusion:
Laparoscopic simple enucleation and enucleation-separation technique are safe, efficient, and minimally invasive therapies for selected patients with RAMLs. In addition, the enucleation-separation appears to significantly minimize the warm ischemia injury and results in superior short-term renal function preservation, which could be a nephron-sparing alternative for the treatments of RAMLs.
Introduction
R
Although a latest study showed that sirolimus could decrease the volume of RAMLs, the side effects and the concern for lifetime treatment limited its use. 3 Besides, the rapid growth or blunt abdominal impact injury of RAML might lead to tumor rupture and life-threatening hemorrhage. In the year of 2002, Yamakado and colleagues 4 concluded that the RAML bigger than 4 cm in diameter was an independent prognostic factor for spontaneous bleeding. Although angioembolization is an alternative treatment, regrowth and repeated hemorrhage after embolization remain a concern. Therefore, we usually take surgical intervention to manage the RAMLs with diameter more than 4 cm. The standard surgery is partial nephrectomy. However, Minervini and colleagues 5 confirmed the optimum results of simple enucleation for RAMLs. No patients in their study were found with recurrence or urinary leakage during the follow-up. It was suggested that this surgical approach could guarantee excellent long-term local control.
CT is widely used in the diagnosis of RAMLs. 6 We could obtain precise preoperative images of the size and location of the tumor. While enucleating the tumor, the renal artery needs to be clamped so as to minimize the bleeding and attain clear surgical fields especially during a laparoscopic procedure. As RAML is a benign tumor, urologists should preserve the function of the rest of the normal renal tissue as much as possible while enucleating the RAML. For this purpose, minimizing warm ischemia time (WIT) is mandatory. 7 In terms of single, ventral exophytic RAML, we developed a novel technique to enucleate and separate the tumor with better visualization and less WIT. The aim of the present study was to describe our surgical experience with laparoscopic enucleation-separation for treating these specifically located RAMLs in our institute.
Patients and Methods
Patients
Written consent was given by all patients and their information was recorded. This study has been approved by the Ethics Committee of Central South University. We prospectively analyzed 40 patients who underwent laparoscopic simple enucleation or the modified surgical treatment called laparoscopic enucleation-separation from January 2011 to February 2013. Inclusion criteria for the operations were patients with a single, ventral exophytic RAML of >4 cm (Fig. 1). Patients with any contralateral renal abnormalities, affected with TSC or multifocal lesions, were excluded from this study. Patients were randomly allocated into the laparoscopic simple enucleation group (Group 1) or the laparoscopic enucleation-separation group (Group 2). All patients received CT scanning preoperatively and were performed with biopsy to assure a correct diagnosis during the operation.
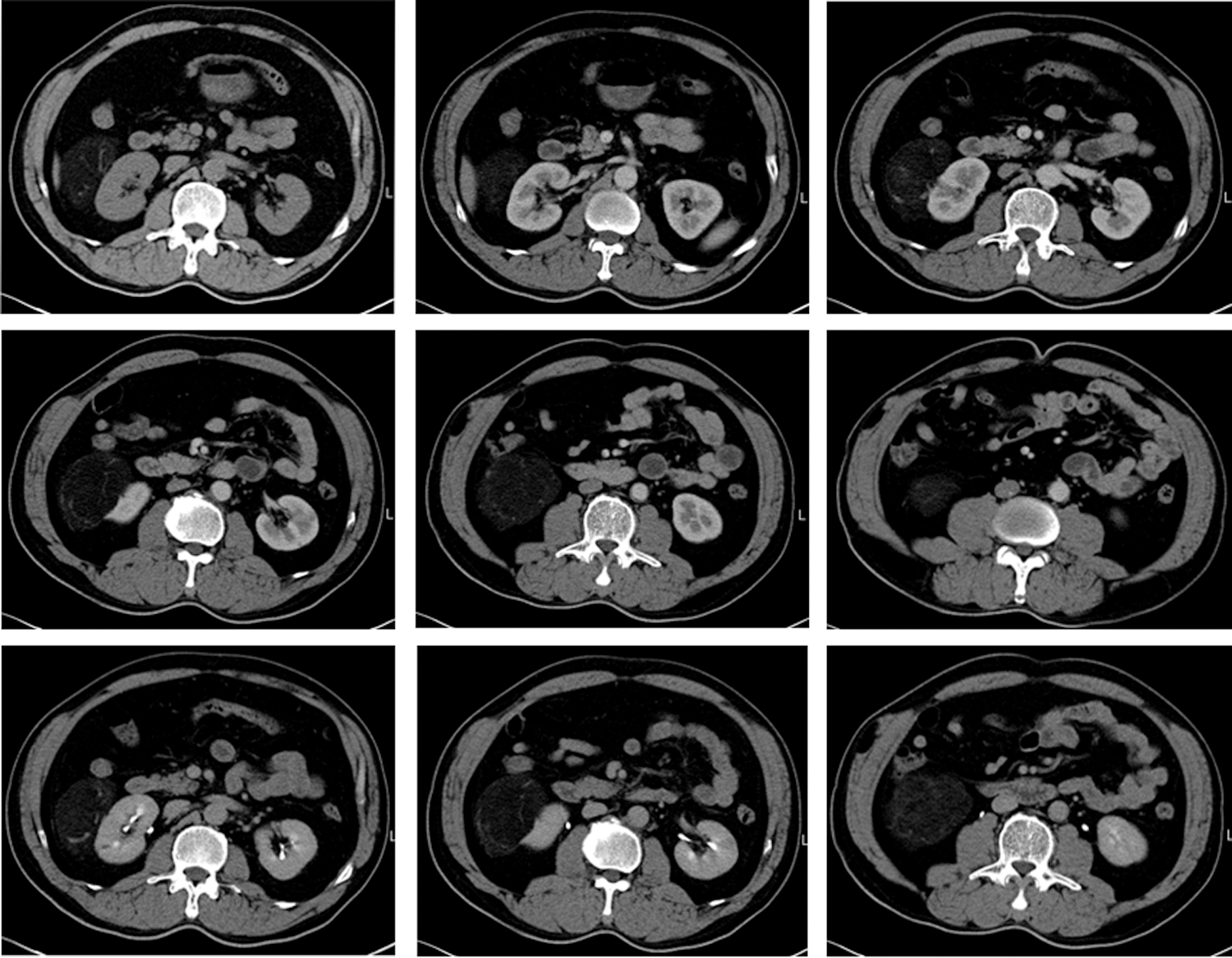
CT scanning from a 41-year-old male patient. The scanning revealed a typical single, ventral exophytic RAML in the right kidney. RAML = renal angiomyolipoma.
The groups were compared for characteristics, perioperative outcomes, renal function changes, and oncologic outcomes using means and percentages. Patient characteristics included age, gender, body mass index (BMI), tumor location (right or left), and tumor size. Perioperative data included operative time, WIT, blood loss, “Broken” peritoneum, and complications. Perioperative complications were categorized according to the Clavien grading system. 8 Renal function was assessed through the glomerular filtration rate (GFR) using technetium-99m diethylenetriaminepentaacetic acid (99mTc-DTPA) before and 3 months after surgery.
Surgical technique
The patients were positioned in the full-flank lateral decubitus position. A retroperitoneal approach was established in all patients. Three 10-mm trocars were usually needed in the procedure. The first trocar was placed below the tip of the twelfth rib. The second one was placed 1 cm above the anterior superior iliac spine for the camera and the third trocar approximately at the cross of the anterior axillary line and subcostal margin of the twelfth rib. An artificial pneumoperitoneum was created by CO2 insufflation at a pressure of 14 mm Hg.
Retroperitoneal fat tissue was removed en bloc. The Gerota's fascia was then longitudinally incised, and perirenal fat was excised to expose the tumor and surrounding normal parenchyma. The tumors were isolated completely in the patients of Group 1. Renal artery was prepared to allow the accommodation of a “bulldog” hemostat for artery blockade. After the artery was clamped by bulldogs, the RAMLs were enucleated by Harmonic Scalpel and suction device under direct visual guidance. The parenchymal defect was closed with continuous sutures of 1-0 absorbable suture with Hem-o-lok clips securing each needle point. After the renorrhaphy was completed, the vascular clamp was removed.
In the patients of Group 2, the surgical technique was modified. As described above, similar position and surgical approach were made. The biggest difference between two groups was the management of the perirenal fat. Extra attention should be paid to preserve the adipose tissue on the tumor surface to keep the tumor attached to the peritoneum (Fig. 2A). Renal artery was isolated and clamped, similar to the steps in Group 1 (Fig. 2B, C). RAML was then enucleated and separated from the parenchyma bed by sharp and blunt dissection with the help of Harmonic Scalpel (Fig. 2D, E), and while doing so, the RAML was attached to the peritoneum and was “pushed away” by the pressure of pneumoperitoneum. The surgical margins and renal surface were inspected with extreme caution to rule out any possible residual tumor. Renorrhaphy was carried out as described above in the patients of Group 1 (Fig. 2F). The vascular clamp was removed (Fig. 2G). Finally, the RAML was separated from the peritoneum en bloc and removed from the body in an Endobag (Fig. 2H).

Major steps included in the enucleation-separation procedure.
Statistical analysis
Continuous variables, categorical variables, and proportions were compared using the t test, chi-squared test, and Z-test, respectively. p-Value <0.05 was considered statistically significant. All calculations were done by SPSS 13.0 statistical software.
Results
All 40 patients were performed with effective laparoscopic operations for pathologically confirmed RAML. The detailed patient demographics are listed in Table 1. Average age, BMI, sex distribution, and tumor location and size showed no significantly difference between the two groups (p > 0.05), which indicated that data from the groups were comparable. The duration of follow-up was 22.6 ± 4.7 and 23.1 ± 5.4 months in Group 1 and 2, respectively (p > 0.05).
BMI = body mass index; GFR = glomerular filtration rate.
Perioperative and oncologic outcomes of patients are presented in Table 2. The operative time (95.3 minutes vs 92.2 minutes, p = 0.278) and estimated blood loss (58.5 mL vs 55.7 mL, p = 0.978) in both groups were comparable. There were slightly higher rates of “broken” peritoneum in Group 1 than Group 2 (3 vs 1, p = 0.605). Average WIT in Group 1 was much longer than that in Group 2 (25.3 minutes vs 17.6 minutes, p = 0.001). One patient had postoperative hemorrhage in Group1 and had received transfusions (Clavien type II). No other severe complications, including hematoma, pneumothorax, and urinary fistula, were observed in both groups. As shown in Table 1, there were no differences between the groups in preoperative GFR levels of the affected kidney, whereas a significantly lower GFR reduction of the affected kidney was found in the Group 2 (Group 1 vs Group 2, 24.3% vs 18.3%; p = 0.001) (Table 2). No local recurrences were found during the follow-up period.
WIT = warm ischemia time.
Discussion
RAMLs were first described in 1900. 9 With the development of diagnostic methods such as high-definition CT scanning, RAMLs can be found and precisely located before surgical intervention. Two traditional treatments, including nephron-sparing surgery (NSS) and selective arterial embolization (SAE), were thought with excellent success. 10 Nelson and Sanda 1 concluded that most RAMLs can be managed with NSS when intervention is required. Nevertheless, Minervini and colleagues 5 believed that NSS remains an extreme curative option at risk of hemorrhage, which cannot be considered the gold standard procedure in most clinical settings. In addition, NSS carries a complication risk of 5% to 23%, 11 –13 with data from Berglund and colleagues 13 showing an increased risk of conversion to radical nephrectomy when performing NSS on RAMLs. SAE also carries a risk of nonfunctional kidneys or development of hypertension and persistent symptoms, which can occur in 14% to 80% of patients 1 after SAE.
In the present series, we utilized the simple enucleation and a modified enucleation-separation technique for the treatment of exophytic RAMLs. Before any new technique is being widely applied, the safety of patients is always the priority to be considered. Only one patient suffered a Clavien type II complication in our study (postoperative hemorrhage), which is similar to 5% to 23% reported in previous NSS articles. 11 –13 Oncologic outcome is another main concern of the surgeons, as well as of patients. Rare published article focused on the long-term oncologic outcome of RAMLs after minimal invasive operations. Chan and colleagues 14 tried to review the long-term outcome of SAE in treating RAMLs and concluded that 4/27 patients required re-embolization and 4/27 patients still need another renal surgery because of recurrence. Boorjian and colleagues 10 used open NSS to treat RAMLs and found 2/58 patients had recurrence during follow-up. In our study, no patient (0/40) underwent recurrence. Similarly, Minervini and colleagues 5 reported that 34 RAML patients underwent simple enucleation and no one had a recurrence during long-term follow-up. Thus, laparoscopic enucleation could guarantee satisfying oncologic outcomes compared with NSS and SAE.
Intact peritoneum and artificial pneumoperitoneum were quite helpful for enucleation-separation. When the tumor was enucleated and separated, the pressure of pneumoperitoneum would “push away” the RAMLs and peritoneum could get “glued” to the tumor. The RAMLs could be dealt with after the renorrhaphy was completed. This technique decreased about 8 minutes of WIT compared with simple enucleation (25.3 minutes vs 17.6 minutes, p = 0.001). Serum creatinine level is inappropriate for estimating renal function changes in the affected kidney because the normal contralateral kidney compensates for function. 15 Thus, we used 99mTc-DTPA to evaluate renal function. Postoperative examination of 99mTc-DTPA/SPECT at 3 months confirmed that enucleation-separation could preserve more short-term renal function (Table 2). Thus, this technique allowed for the maximum preservation of renal functioning tissue in selected patients.
The retroperitoneal approach is needed for the enucleation-separation surgery to treat RAMLs. Fan and colleagues 16 evaluated the efficiency and safety of the retroperitoneal and transperitoneal approaches in laparoscopic radical/partial nephrectomy for renal-cell carcinoma. They believed that retroperitoneal approach might be faster and equally safe compared with the transperitoneal approach.
An intact peritoneum was crucial for this procedure. Although the enucleation-separation technique could be carried on with an incomplete peritoneum, it would influence the surgical fields and expand the surgical time. However, it can be easily avoided by an experienced surgeon if extreme attention had been paid. In addition, low incidences of “broken” peritoneum occurred in the present study.
Some limitations of this study need to be addressed. First, we conclude that laparoscopic enucleation is as safe and efficient as NSS and SAE based on our experience and review of the literature, which might limit the reliability. Second, the sample size is relatively small. A larger sample size would have conferred higher value to the comparison.
In conclusion, laparoscopic simple enucleation and enucleation-separation technique are safe, efficient, and minimally invasive therapies for selected patients with RAMLs. In addition, the enucleation-separation appears to significantly minimize the warm ischemia injury and results in superior short-term renal function preservation, which could be a nephron-sparing alternative for the treatments of RAMLs.
Footnotes
Acknowledgments
This study was supported by the National Natural Science Foundation of China (No. 81001137) and the project (No. 2010sk3102) from China Hunan Provincial Science and Technology Department.
Author Disclosure Statement
No competing financial interests exist.