
Abstract
Introduction:
The costs of flexible ureterorenoscopes (fURSs) and their repair oblige the surgeon to know the proper handling of instruments. There is a lack of evidence in the literature about the safety distance that the laser fiber should have once out from the ureterorenoscope to avoid instrumental damages.
Materials and Methods:
We performed an in vitro observational study. Seven fURSs were tested. The distance from the laser fiber tip and the fURS camera was measured at the first appearance on the endoscopic screen and when the fiber was reaching one-fourth of the screen. Second, to evaluate the impact of the holmium laser bubble according to different fiber distances, an assessment of the size and shape of the bubble created at the tip of the fiber with the laser activated was done, recording the images with a high-speed camera.
Results:
The first appearance on the screen of the laser tip is different in different ureterorenoscopes. In all the ureterorenoscopes, we observed that when the laser fiber was at ¼ of the screen, the bubble was never touching the fURS tip.
Conclusion:
Even if there is a big limitation of this study due to the impossibility to measure and to evaluate the damage of the fURS tip surface, we observed that when the laser fiber tip reaches ¼ of the screen, the bubble generated by laser activation is never rebounding on the camera of the ureterorenoscope, preserving it from laser damages. We can define this position as the safety distance.
Introduction
F
Materials and Methods
An in vitro observational study was performed. Seven fURSs were tested, including both fiber-optic (OU) and digital (DU) fURSs: Olympus P6 (OU), Olympus V (DU), Olympus V2 (DU), Wolf Boa (DU), Wolf Cobra Vision (DU), Storz XC (DU), and Boston Scientific LithoVue (DU). Initially, the laser fiber was loaded into the working channel of the different fURSs. A 273-μm laser fiber and a 30 W holmium laser YAG (Ho:YAG) machine (Rocamed) were used. The distance from the laser fiber tip and the fURS camera was measured with a ruler by a single investigator at the first appearance on the endoscopic screen (D1) and when the fiber reached one-quarter of the screen width (D2) (Table 1 and Fig. 1).
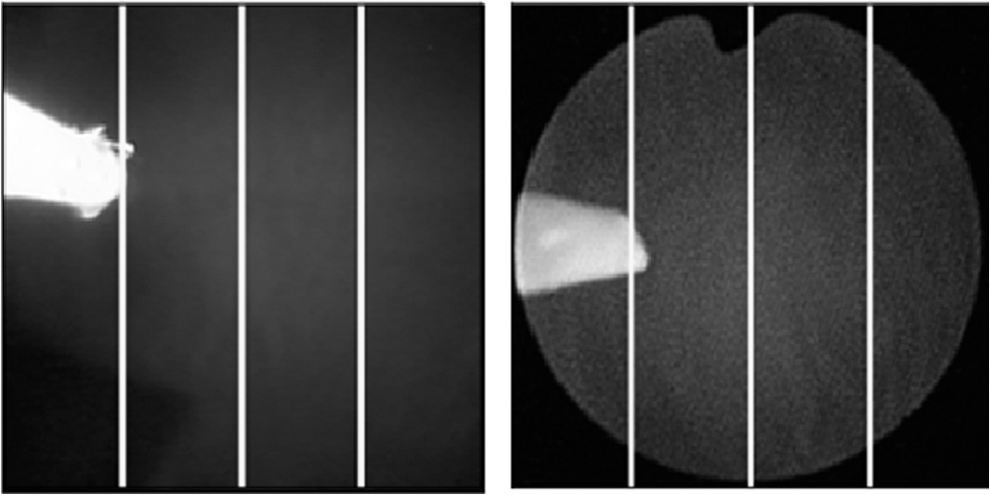
Laser fiber at one-quarter of the screen in a digital (left side) and an optical (right side) fURS. fURS = flexible ureterorenoscope.
To evaluate the effect of Ho:YAG bubbles at different fiber distances, we assessed the size and shape of the bubble created at the tip of the fiber when the laser was activated. Videos were taken of four different scenarios in saline: with no working material, with a sample of pork kidney as soft tissue, with a synthetic hard stone simulating a calcium oxalate monohydrate calculus, and with a synthetic soft stone simulating an acid uric stone. The stone phantoms were prepared using BegoStone powder according to the indications of Esch and colleagues. 6 Images of the laser activation were recorded at the tip of the fiber using a Photron APX-RS 3000 high-speed camera with a setting of 30,000 frames per second (fps) when the fiber was 1 and 2 mm outside the ureterorenoscope and at 15,000 fps when the fiber was 3 mm outside the ureterorenoscope. The different fps settings were needed because when the fiber was at 3 mm, the camera's field of view was not wide enough to capture the entire image with a 30,000 fps capture setting.
The evaluations were performed with the laser fiber tip at 1–3 mm from the fURS camera. Before the laser activation, two investigators checked the distance of the laser fiber from the ureterorenoscope at 1–3 mm with a ruler. The fURS was fixed on a robot arm, and the position of the ureterorenoscope related to the target position was fixed and maintained by the robot (Fig. 2, img. 1). Different laser settings were used to provide a variety of output energy conditions to simulate the dusting and fragmentation of the different kinds of stones and the ablation of pork kidney tissue by using both short and long pulse combinations (Table 2).

Laboratory setting: 2–1 working table with the fURS hanging on the robotic arm on the left side and the high-speed camera in the center of the table; 2–2 bowl with a sample of pork kidney and the fURS coming from the top; and 2–3 table setting.
The settings were recorded at a distance of the laser fiber of 1, 2, or 3 mm.
J = Joule; Hz = Hertz; LP = long pulse; SP = short pulse.
Finally, with the laser fiber at 3 mm, three combinations of joules (J) and hertz (Hz) (0.5 J, 10 Hz; 1 J, 10 Hz; and 2 J, 5 Hz) were tested with no working material and with the synthetic soft stone. These were changed for each setting of pulse length to check for differences in the bubble dimensions between short and long pulses. The two major diameters of the bubbles were measured using ImageJ software. The distance between the stone and the fiber tip was 1 mm. We performed all experiments with the tip of the laser fiber cut to eliminate the distal transparent part. For the laser test, we used the fURS LithoVue system from Boston Scientific.
Results
The first appearance on the screen of the laser tip differed between different ureterorenoscopes. Both the Wolf Cobra Vision and the Wolf Boa had the same D1, which was 1 mm and was the shortest of all ureterorenoscopes tested. The Storz XC had the longest distance at D2: 4 mm. For all ureterorenoscopes, D1 was 1–2 mm and D2 was 3–4 mm. Our recording of the bubble generated by the laser showed that at the 1 mm distance, regardless of the laser setting and the kind of tissue in front of the ureterorenoscope, the energy rebounded on the ureterorenoscope's tip (Fig. 3). The only situation in which the bubble did not return to the ureterorenoscope surface at the 1 mm distance occurred when the laser was activated in 0.9% NaCl solution without anything in front and at low energy (0.5 J) and long pulse duration (Fig. 4). At the 2 mm distance, using different machine settings and different scenarios, we never observed the bubble touching the fURS tip. At the same distance, we observed some stone dust rebound on the fURS camera when the laser was activated with energy >1 J regardless of the length of the pulses. At the 3 mm distance, the bubbles never touched the fURS tip and the return for the stone powder was lower than at 2 mm. Keeping the same frequency and the same energy and changing only the pulse length, we observed that the bubble generated with short pulses was always larger than that generated with long pulses, regardless of the scenario (Fig. 5 and Table 3).
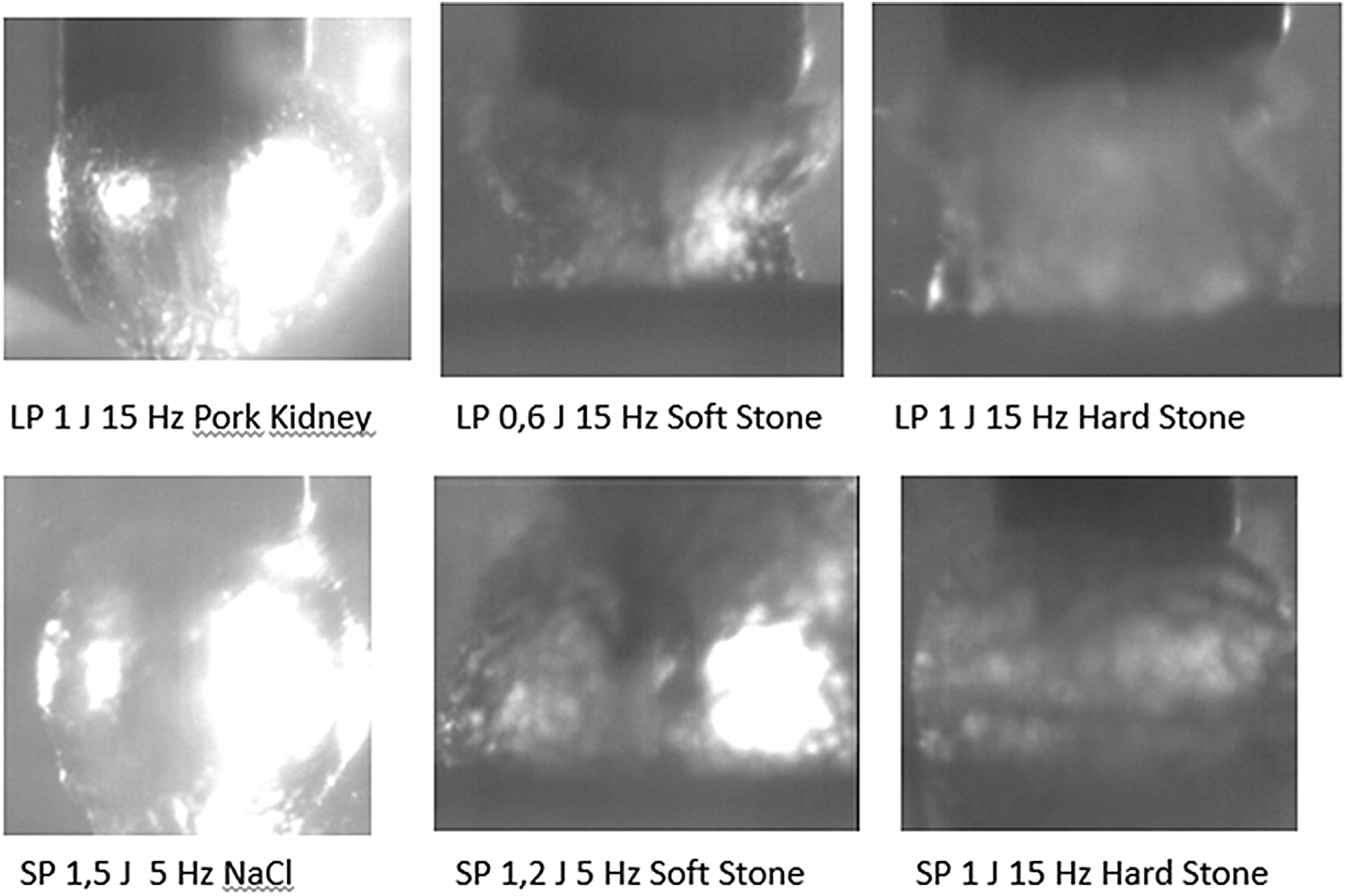
Different laser bubbles touching the ureterorenoscope at a distance of 1 mm.

Bubble created by the 273 μm laser fiber at a distance of 1 mm from the ureterorenoscope in 0.9% NaCl with energy of 0.5 J, frequency of 15 Hz, and long pulse duration. The bubble does not touch the tip of the fURS.
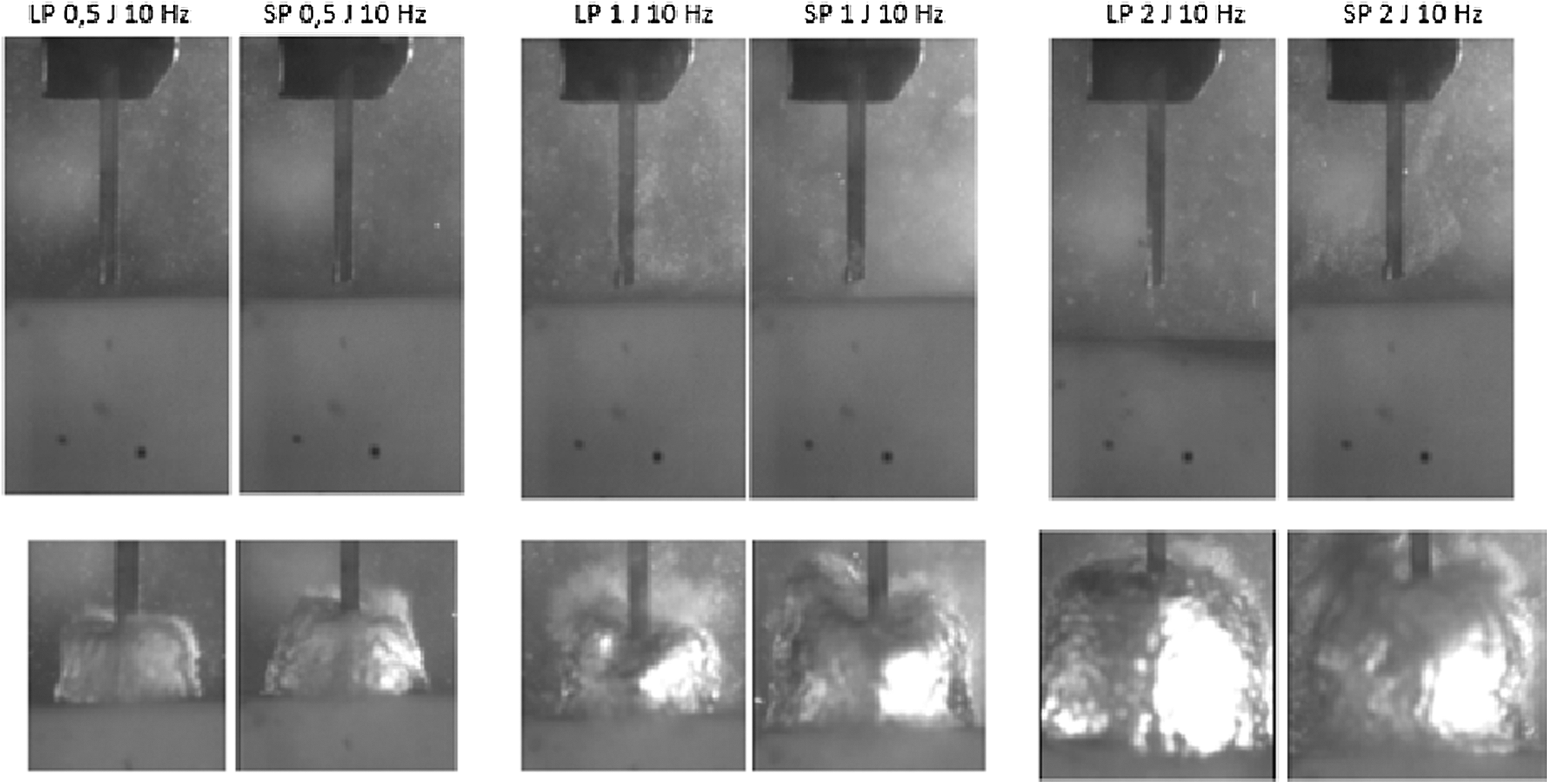
Comparison of bubbles generated at the same energy with different pulse lengths in 0.9% NaCl without any surface in front and with a soft synthetic BegoStone. The laser fiber is 3 mm outside the ureterorenoscope.
The bubble generated with short pulses was always larger than that generated with long pulses. The two major diameters were measured using ImageJ software.
Discussion
The pulses generated by the Ho:YAG laser are capable of cutting the steel wires of a basket, guidewires, and many other materials. The damage to baskets and guidewires induced by the pulses of the Ho:YAG laser is attributed to the high temperatures generated at the tip of the fiber. 7,8 Kang and colleagues demonstrated that greater heat dissipation with a thicker liquid layer reduces ablation efficiency. This means that the closer the laser tip is to the target, the greater the efficiency, and at the same time, the farther the laser tip is from the fURS, the lesser the damage created. 9 We agree with Cecchetti and colleagues who wrote that when using the Ho:YAG laser, it is essential that no procedure should be performed without clear and accurate visual control to ensure that the fiber tip is in contact only with the target and sufficiently far from the ureteral wall to avoid the damage that the cavitation bubble can cause to healthy soft tissues. Cecchetti also noted that an adequate distance is necessary from the baskets and guidewires present in the urinary tract to avoid damage. 10
Canales and colleagues reviewed the data on fURS repairs of their systems from 2000 to 2004. They had 324 repairs: 30% involved the distal part of the ureterorenoscopes, and 4% were repairs to the objective lens, C-cover, and cover glass. 3 In a retrospective study of the reasons for repairs of four instruments after 655 consecutive ureterorenoscopies in a single center, Kramolowsky and colleagues 11 reported the clouded lens to be the most common damage. Several groups have previously reported either institutional or manufacturer data regarding the causes and location of fURS damage. Sung and colleagues reported that more than 50% of the damage occurred in the working channel (laser burn in the working channel) or extreme ureteroscope deflection. 12
Shangguan and colleagues investigated the effects of density, viscosity, and mechanical strength on laser-induced cavitation bubbles formed in absorbing liquids (e.g., blood, contrast medium, or saline). They found that the bubble dynamics strongly depended on physical properties of the absorbing liquid and that cavitation bubbles were larger in saline than in liquid with a higher density. 13 Therefore, we can assume that in the presence of liquid with a higher density than saline, with the same laser settings, the cavitation bubble generated by the laser machine will be smaller.
The appearance on the screen of the laser fiber at different distances depends on the brand of the ureterorenoscope. Given that fURSs have a 0° camera, it is important to be aware that when the fiber becomes visible on the screen, as our data suggest, it is already at least 1 mm out from the ureterorenoscope. This knowledge is fundamental for avoiding accidental trauma to the urothelial epithelium while manipulating the ureterorenoscope. We observed that in four fURSs over seven, the fiber barely appeared on the screen at a distance of <2 mm. In all ureterorenoscopes, when observed at one-quarter of the screen, the fiber was out 3 mm or more (Fig. 6). Matching these results with the observation that the bubble generated by the Ho-YAG when the laser fiber is at a distance of 3 mm from the fURS tip is never touching the camera of the ureterorenoscope even with high energy and short pulse, we can establish this position as the safety distance for avoiding fURS tip damage.
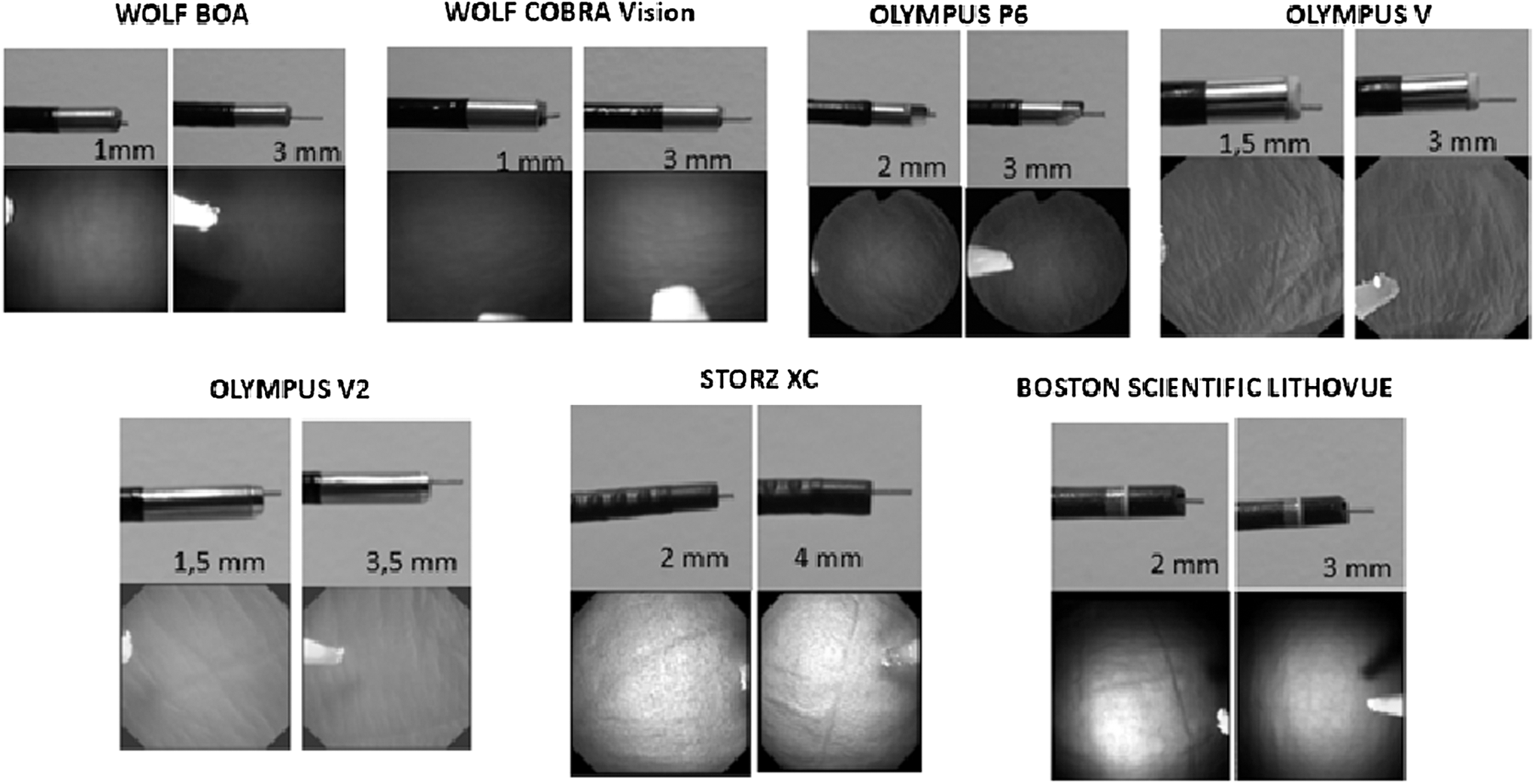
Images of the fiber distance at D1 and D2 in different fURSs: external view and endo view.
Some difficult cases can oblige the surgeon to use the fiber at the first appearance of the endoscopic screen. In this case, we suggest using low energy (≤0.5 J) and long pulse duration because the maximum radius of the bubble is a function of the energy and pulse duration of the laser pulse. 14 If a higher energy is required, we suggest using it for a short time to avoid instrument damage. However, there are few data about camera deterioration. We propose that laser energy hitting the ureterorenoscope using a long distance could damage the fURS tip, including the camera glass and light source. One important limitation of this study was that we could not measure and evaluate damage to the fURS tip surface because several new fURSs would be needed to complete a full evaluation. Further studies are needed to assess the real damage to the ureterorenoscope tip.
Conclusion
The aim of this report is to provide some recommendations for using the fiber laser of fURS systems. Based on our findings, we believe that it is safe to position the laser tip at one-quarter of the distance to the monitor because at this distance, with all ureterorenoscopes tested, the holmium laser energy did not return to the instrument camera. We call this the safety distance. In difficult cases, when it may be necessary to have the laser fiber closer to the ureterorenoscope, it is advisable to use the lowest energy possible and a long pulse duration according to the nature of the tissue being treated.
Footnotes
Acknowledgment
Dr. Esteban Emiliani is sponsored by a European Urological Scholarship Programme (EUSP) scholarship.
Author Disclosure Statement
No competing financial interests exist.