
Abstract
Purpose:
Early urinary control is a major goal for patients undergoing robot-assisted radical prostatectomy (RARP). We report our technique of posterior urethral suspension (PUS) performed at the time of urethrovesical anastomosis.
Patients and Methods:
We prospectively followed men with localized prostate cancer undergoing RARP by a single surgeon from August 2012 to October 2015. Patients before April 2014 underwent only bladder neck preservation (controls), while patients after April 2014 also underwent PUS. Patients were given a modified Expanded Prostate Cancer Index Composite questionnaire, along with questions depicting objective measures of urinary control (type of pad, number of pads, wetness of pad). Time points queried were preoperatively and postoperatively at weeks 1, 2, 4, and 12. Our primary outcome was pad-free survival.
Results:
Questionnaire response rate was 52% (56/107) for controls and 43% (36/83) for PUS. There were no differences in baseline demographics, preoperative urinary control, intraoperative variables, or postoperative complications between groups. There were few subjective improvements in urinary control for PUS compared with controls. More notable, PUS patients had significantly improved objective measures of urinary control, including less protective incontinence products at 1 and 2 weeks after catheter removal (p < 0.03). They also wore fewer pads and had less leakage on each pad that lasted from week 1 to week 4 after catheter removal (p < 0.01). PUS patients had pad-free rates of 37%, 47%, 54%, and 60% compared with controls 15%, 18%, 24%, and 36%, at weeks 1, 2, 4, and 12 after catheter removal (p = 0.07).
Conclusion:
PUS may improve objective measures of early urinary control compared with controls. With no increase in operative time and no change in complication rates, further work in a randomized setting would provide additional weight to our findings.
Introduction
T
The “Rocco stitch” is perhaps the most referenced technique to aid in early recovery of urinary control and involves posterior musculofascial plate reconstruction. 5 Other techniques that have been described include bladder neck preservation (BNP), 6 anterior urethropexy, 7 and utilization of autologous slings. 8,9
In January 2014, Soljanik and colleagues described anatomic differences between continent and incontinent men after RP using functional MRI. 10 They observed a reduced angle of the membranous urethra in relation to the pubic symphysis correlated with urinary control. Shortly thereafter we modified our robot-assisted radical prostatectomy (RARP) technique by adding posterior urethral suspension (PUS) sutures to elevate the pelvic floor and reduce the membranous urethra-pelvic angle. Herein, we describe our technique and initial outcomes.
Patients and Methods
Patients
We prospectively followed men with localized prostate cancer undergoing RARP by a single surgeon from August 2012 to October 2015 in an institutional review board-approved database. All patients provided written informed consent preoperatively. All patients undergoing surgery were included in this study; there were no exclusion criteria. Patients before April 2014 underwent only BNP (controls), while patients after April 2014 additionally had PUS (technique described below). No patient had a posterior musculofacial reconstruction. Patient demographics, preoperative findings (prostate-specific antigen [PSA], prostate volume, clinical T stage), surgical variables (operating time, blood loss, neurovascular bundle preservation), pathologic T stage, and postoperative complications were collected.
Methods
Preoperatively, all patients were given a questionnaire packet and instructed to fill them out at weeks 1, 2, 4, and 12, after catheter removal. The first half of the questionnaire was modified from the Expanded Prostate Cancer Index Composite (EPIC) urinary domain.
11
We adjusted the time component of the EPIC questionnaire from symptoms during “the last 4 weeks” to “the last 3 days” to track the week-to-week recovery of urinary control. To monitor objective measures of urinary control, the second half of the questionnaire queried the type of incontinence product worn, number of products worn, and the wetness of the product, similarly demonstrated in the Society of Urodynamics, Female Pelvic Medicine, and Urogenital Reconstruction (SUFU) Pad Test Study.
12
A sample questionnaire is available online (Appendix A; Supplementary Data are available online at
Surgical technique
After complete removal of the prostate and obtaining hemostasis, bilateral size 2-0 polyglactin sutures are preplaced into posterior urethral rhabdosphincter connective tissue at the 5 and 7 o'clock positions (Supplementary Video S1; Supplementary Data are available online at
Both control and PUS patients have a 16F suprapubic tube and an 18F urethral catheter postoperatively. The morning after surgery, the urethral catheter is removed and the patient is typically discharged home. The suprapubic tube is capped about postoperative day 8 to 10 and the patient begins voiding. The suprapubic tube is subsequently removed at the first follow-up appointment on postoperative day 10 to 12.
Statistics
Statistical analysis was performed with SPSS version 22 (Armonk, NY). Continuous parametric and nonparametric variables were compared using a t-test for independent variables and the Mann–Whitney U test, respectively. Categorical variables were compared using Pearson chi-square analysis or Fisher's exact test, and multiple linear regression was used to assess for variables predictive of achieving pad-free status. Pad-free survival analysis was performed using the Kaplan–Meier method and log-rank test. Significance values were set at p = 0.05.
Results
There were 190 patients who underwent RARP during the study period, 107 controls and 83 PUS. Questionnaire response rate was 52% (56/107) for controls and 43% (36/83) for PUS. Baseline demographics, preoperative factors, and intraoperative outcomes, including neurovascular bundle preservation, were similar between groups (p > 0.05, Table 1).
BMI = body mass index; PSA = prostate-specific antigen; PUS = posterior urethral suspension.
Preoperatively, there were no differences in any measure of urinary control between groups (all p > 0.4). Postoperatively, there were few subjective differences between groups. At week 1, PUS patients had improved leakage of urine (question no. 3) that did not persist at week 2 (p = 0.05). In addition, at week 2, PUS patients had improved daytime urinary control (question no. 1) that did not persist at week 4 (p = 0.02). More notable, PUS patients had significantly improved objective measures of urinary control. PUS patients wore significantly less protective incontinence products (question no. 5) at 1 and 2 weeks after catheter removal (p < 0.03, Fig. 1). They also wore fewer pads (question no. 6) and had less leakage on each pad (question no. 7) that lasted from week 1 to week 4 after catheter removal (p < 0.01, Figs. 2 and 3, respectively). By 12 weeks, these differences between groups had resolved. Pad-free rates for PUS were 37%, 47%, 54%, and 60% compared with controls 15%, 18%, 24%, and 36%, at weeks 1, 2, 4, and 12 after catheter removal, respectively. Figure 4 demonstrates pad-free survival curves for both groups (p = 0.07).
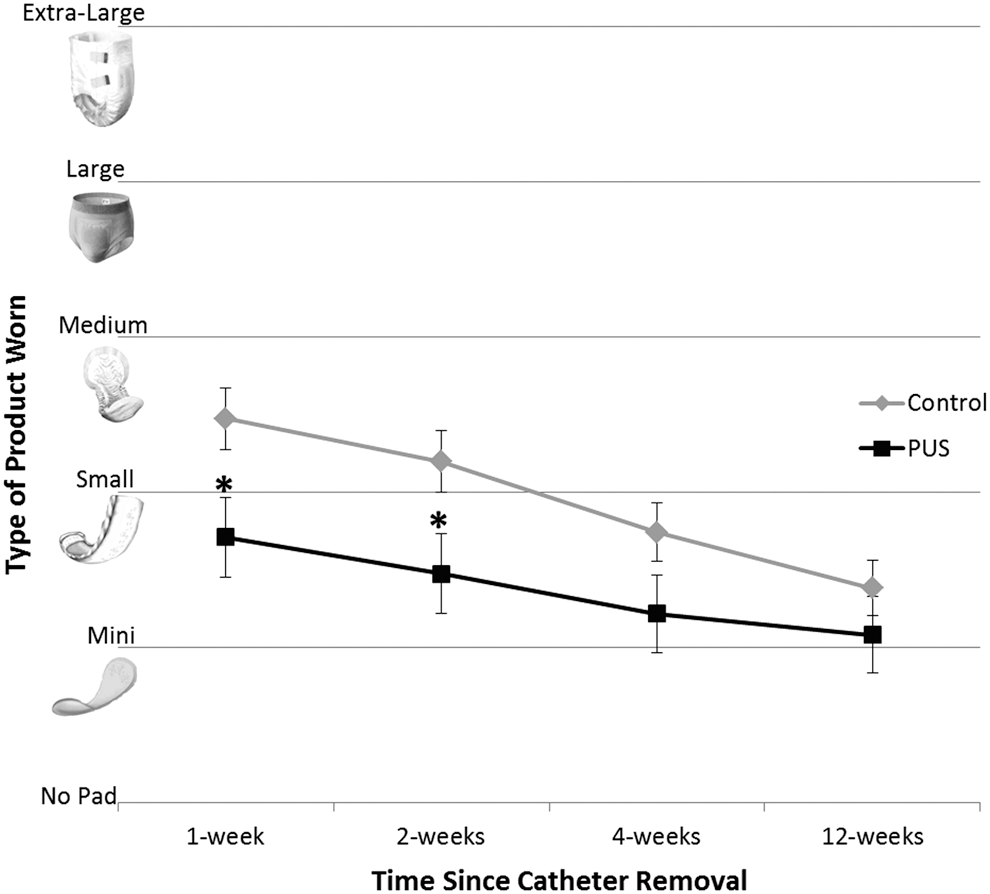
Type of incontinence product worn. Asterisk denotes p < 0.05.
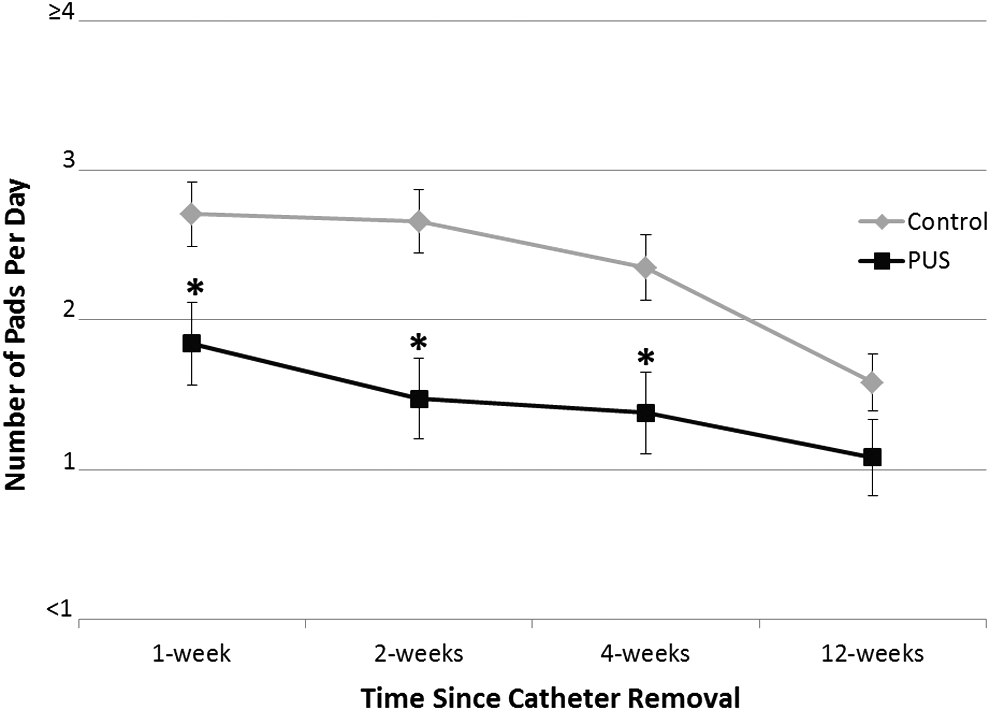
Number of individual pads or adult diapers worn per day. Asterisk denotes p < 0.05.

Average pad wetness. Asterisk denotes p < 0.05.

Kaplan–Meier curves of pad-free survival.
To evaluate whether improved early continence was due to PUS or other independent variables, including surgeon experience over the course of the study, multiple linear regression analysis was performed for pad-free status at each time point (Table 2). Both PUS and patient age remained significant from weeks 1 to 4, while at week 12 only patient age and neurovascular bundle preservation were predictors of pad-free status. Surgeon experience and patient body mass index did not correlate with pad-free status at any time point.
p < 0.01.
p < 0.05.
B = regression coefficient; ns = not significant; SE = standard error.
Postoperative complications were similar between groups (p = 0.7, Table 1). Table 3 lists grade III complications for controls and PUS. There were no grade IV or higher complications. Analyzing only urinary retention, there was no significant difference between groups (p = 0.6). One control patient (0.9%) developed urinary retention postoperatively from a urine leak, misplaced urethral catheter, and subsequent bladder neck contracture. Two PUS patients (2.4%) developed urinary retention. One had endoscopic-confirmed bladder neck edema that resolved after an additional 2 weeks of urethral catheterization, while the other developed a bladder neck contracture that required in-office dilation 3 weeks postoperatively and has not recurred.
IVC = inferior vena cava.
Discussion
Investigations of anatomic and functional changes after RP have improved our understanding of urinary recovery. Ficazzola and Nitti performed postprostatectomy urodynamic evaluation in 1998 and demonstrated that intrinsic sphincter deficiency is the major deficit in the majority of men. 13 Recently, Soljanik and colleagues demonstrated that, by studying postprostatectomy MRI, incontinent men have a wider angle of the membranous urethra and descent of the bladder neck and external urethral sphincter. 10 They later confirmed these results by performing transobturator sling placement in postprostatectomy incontinent men and noted correlation between continence and the decrease in membranous urethral angle. 14 As such, we were motivated to adjust our RARP technique to improve the early return of urinary control.
This prospective single surgeon cohort series demonstrates PUS significantly improves objective measures of urinary control in the early weeks after surgery compared with BNP alone. Although log-rank testing did not demonstrate a significant pad-free survival difference (p = 0.07) between both cohorts, there is demonstrable separation of the curves from week 1 to 12. In addition, PUS remained a significant independent variable in improving urinary control after accounting for other surgical factors, including surgeon experience during the study period. However, as should be expected, younger age and neurovascular bundle preservation were also significant variables in improving urinary control. Unfortunately, our control patients did not complete a Sexual Health Inventory for Men (SHIM) questionnaire at the 12-week time point, so we are unable to report any possible change in erectile function due to PUS. We hope future studies will include this important data.
Intuitively, the most common potential complication concerning PUS is urinary retention, likely from over tensioning causing obstruction. We believe that complications related to PUS are minimal when tensioned properly. The goal is to provide urethral support and prevent pelvic floor descensus, not direct urethral compression. Although there was no significant difference in complication rates between the two groups, PUS did have 2.4% (2/87) urinary retention rate compared with BNP 0.9% (1/107). The specific etiology of these cases is unclear, and further work with our technique will allow us to assess this risk going forward.
The importance of improving QOL outcomes cannot be overstated. In 1995, Litwin and colleagues quantified sexual and urinary function QOL measures after localized prostate cancer treatment and noted worse urinary function QOL after prostate surgery. 1 Further QOL work utilizing the EPIC questionnaire demonstrated the early decline in continence following RP, most notable at 2 months after surgery. 3 These investigators also went on to show that overall patient satisfaction with treatment outcome is independently associated with urinary incontinence, along with sexual and hormonal function.
Multiple surgical techniques have been described to improve early urinary control. First published in 2001, the “Rocco stitch” has been the most studied technique to achieve early urinary control. A 2012 meta-analysis demonstrated significantly improved urinary control at both 3 to 7 days (HR 1.79, 95% CI 1.06, 3.03) and 30 to 45 days (HR 1.57, 95% CI 1.15, 2.14) after surgery compared with controls. 15 However, the results are variable as both randomized trials found no significant difference. 16,17 BNP, which we attempt in all patients, has also been shown to improve early recovery of urinary control. Stolzenburg and colleagues retrospectively compared BNP with bladder neck resection and noted improved continence (0–1 pads) immediately after catheter removal (20% vs 9%, p = 0.04) as well as at 3 months (73% vs 60% p = 0.05). 6 Anterior urethropexy, a technique that utilizes a second dorsal venous complex suture that is placed and secured to the posterior pubic symphysis periosteum, has also been shown to improve EPIC urinary incontinence scores at 3 months. 7 While this technique appears similar to PUS, we believe PUS provides additional support due to the posterior placement (compared with a single anterior suture), thereby altering the vesicourethral angle and preventing bladder/pelvic floor descent. Finally, the improvement in urinary control due to neurovascular bundle preservation 18 and younger age 19 has been previously described.
To our knowledge, there are three prior studies that describe a sling technique at the time of RARP, which could be viewed comparably to our technique. Cestari and colleagues fashioned a sling out of the vas deferens, positioned it under a Rocco reconstruction, and anchored it to pubic symphysis periosteum. 8 They noted no difference in continence at 5 and 10 days, although they were only comparing number of pads per day in a relatively small series (60 total patients) that might not capture an effect. They noted significant improvement by 30 days, including 76% vs 46% who were pad free. Kojima and colleagues performed a bladder neck suspension sling by passing a suture between the bladder neck and Rocco reconstruction and securing to the pubic symphysis periosteum. 9 In the sling group, there was significant improvement over the nonsling group when comparing the EPIC urinary domain at 4 weeks after surgery, but not at 12 and 24 weeks. In addition, they noted lower 1-hour pad weights in the sling group at 4 weeks after surgery, but not at 12 and 24 weeks. Finally, valsalva cystograms were performed 7 days after surgery and showed that the posterior urethrovesical angle was smaller in the sling group, consistent with the prior-mentioned MRI study. 10 Most recently, Bahler and colleagues performed a randomized trail utilizing biologic absorbable mesh at the time of RARP. They positioned the mesh under the bladder neck and secured it to cooper's ligament bilaterally. With a primary outcome of 0 to 1 pad continence at 1 month postoperatively, they noted no significant difference (55.2% sling vs 47.1% controls, p = 0.34) between either group. 20 All three sling techniques differ from PUS in that they inherently pass material proximal to the bladder neck urethral anastomosis, whereas the PUS sutures are secured to the posterior urethral rhabdosphincter connective tissue supporting the actual anastomosis and pelvic floor positions.
Comparisons between techniques have obvious difficulties without a randomized trial. At baseline, surgeons have different approaches to RP, differing skill sets, and differing definitions of their surgical steps. What separates our study from other investigations is threefold. First, we defined our goal continence as pad free, as prior work has shown there is a significant difference in QOL measures between pad free and security or 1-pad usage. 21 Second, we were interested in the week-to-week recovery in the initial 3 months after surgery, so we adjusted the EPIC questionnaire to better capture this data. Third, all of our data were collected prospectively. What this combination provides is granularity to assess significant changes attributable to our technique. We understand that it is possible other surgeons might have differing results with this technique, and we hope that providing our data along with a video of our technique will allow other surgeons to attempt PUS and publish their results.
Our study does have multiple limitations. First is the single surgeon series, which requires reproduction by others. Although multiple linear regression did not identify surgeon experience as an independent variable in outcomes, and even with a plateaued learning curve after 15 years of experience and over 900 laparoscopic and RARP, there is still a potential for bias as patients underwent PUS later in the experience than controls. It is unlikely that surgeon skill with other steps of RARP that may impact continence (e.g., bladder neck preservation) has improved. However, we might not be capturing other surgeon-specific or case-specific variables, including differing techniques related to bladder neck dissection, neurovascular bundle preservation, urethrovesical anastomosis, and placement of a suprapubic catheter. Given PUS is the only major change in our operation over the study period, we would expect all other factors to be relatively equal between groups. In addition, there is potential bias in the respondents of our questionnaire. There was a 9% lower response rate in the PUS cohort, the result of which is hard to interpret. One would expect any potential negative response bias to carry through both the controls and PUS groups, but potentially more so in the control group. In addition, our questionnaire has not been wholly validated like other well-described questionnaires. We combined the most pertinent elements from EPIC, 11 and the SUFU pad test study 12 demonstrated that objective patient answers correlated well with actual urine loss. By keeping the questionnaire brief, we hoped patients would not be discouraged from completing.
Conclusions
PUS may improve objective measures of urinary control in the first 12 weeks after RARP compared with BNP alone. While there is minimal subjective patient improvement, our technique has few negative effects without prolonging operative time or increasing the risk of postoperative urinary retention. Further investigations in a randomized setting to validate this technique are warranted.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.