
Abstract
Introduction:
The Nanopulse Lithotripter (NPL; Lithotech Medical, Israel) is a novel intracorporeal device that uses a nanosecond duration electrical discharge through a reusable flexible coaxial probe to endoscopically fragment urinary stones. This device was compared with a holmium laser lithotripsy (HoL) with regard to stone fragmentation efficiency (SFE) and its impact on flexible ureteroscope (URS) deflection and flow of irrigation.
Methods:
Using a custom bench model, a 6 mm BegoStone cylindrical phantom (mixture 5:2) was confined under 0.9% saline atop sequential mesh sieves. The SFE of two NPL probe sizes (2.0F, 3.6F) and two HoL fibers (200, 365 μm) was evaluated using concordant settings of 1 J and 5 Hz. URS deflection and irrigation flow with NPL probes in the working channel were tested in five new fourth generation flexible URS and compared with other adjunct endourologic instruments.
Results:
The 2.0F NPL showed improved SFE compared with the 200 μm laser (86 mg/min vs 52 mg/min, p = 0.014) as did the 3.6F NPL vs the 365 μm laser (173 mg/min vs 80 mg/min, p = 0.05). The NPL created more 1 to 2 mm fragments; the laser created more dust. URS deflection reduced by 3.75° with the 2.0 NPL probe. URS irrigation flow reduced from 36.5 to 6.3 mL/min with the 2.0F NPL probe.
Conclusion:
NPL shows improved SFE compared with HoL. Flow with the 2.0F probe is akin to a stone basket. NPL offers an effective alternative to HoL.
Introduction
A
Despite the similarities in appearance, NPL is functionally different than EHL. Notably, NPL uses a significantly higher voltage and shorter discharge time than EHL, which likely accounts for the differences seen in both its functionality and side effect profile. NPL delivers a 10 kV discharge over 0.25 to 0.50 μsec, and this short high voltage pulse fragments stones by multiple mechanisms, including dielectric breakdown (the electrical charge enters the stone directly) in addition to traditional mechanisms associated with EHL such as cavitation erosion and creation of a shock wave. 1 Importantly, the NPL device has been shown to be safe to surrounding tissue in both ex vivo human tissue and in vivo canine studies, which clearly distinguishes it from EHL. 2,3 NPL probes are also reusable, an added cost-saving benefit, when comparing it to other modalities such as Holmium Laser Lithotripsy (HoL). Table 1 provides a more complete comparison of NPL to EHL and HoL. Of note, HoL works by a completely different mechanism, whereby stone fragmentation is achieved by a photothermal and relatively weak photoacoustic effect. 4
With an understanding of the potential benefits of NPL for treating urinary stones, we sought to investigate its clinical utility by direct comparison with HoL, the gold standard for endoscopic management of ureteral and renal calculi. The purpose of this study is to evaluate the stone fragmentation efficiency (SFE) of this novel intracorporeal lithotripter compared with HoL and to evaluate the effect of the smallest probe (2.0F) on the dynamics of the flexible ureteroscope (URS) in comparison with other commonly used ancillary tools.
Materials and Methods
Stone fragmentation efficiency
Cylindrical Phantom stones measuring 6 × 4 mm and 6 × 5 mm were created using a 5:2 mixture of BegoStone and Water (equivalent in hardness to Calcium Oxalate Dihydrate) and then dried and weighed. One 6 × 4 mm BegoStone was placed within a polyurethane holder to confine the stone. The holder and stone were placed in a 0.9% saline bath atop sequential sieves measuring 3, 2, and 1 mm (Fig. 1). NPL was performed with the Urolith-105 M device (Lithotech Medical, Israel) first using a 2.0F NPL probe at settings of 8 (equivalent to 1.0 J) and 5 Hz, with the probe in light-pressure direct contact and perpendicular to the stone. Fragmentation was complete when all stone materials passed through the 3 mm sieve. Time was measured between the first impulse, first break, and passage of final fragment through the sieve. The fragments were then collected from each chamber, dried separately, and weighed. Stone “dust” was measured as the initial weight less the weight from all stones within the collection chambers after fragmentation. This was repeated for five trials, to achieve a power of 0.8. Each trial was performed with a new probe. The Swiss LaserClast (Electro Medical Systems, Switzerland) 20 W laser with a 200 μm laser fiber was then used to fragment the same stone size at settings of 1 kJ and 5 Hz for five trials. The 3.6F NPL probe and 365 μm holmium laser fiber were also tested in the same manner with the same settings, using a 6 × 5 mm BegoStone, each for five trials. All stone pulverizations were performed by the same urologist, who was experienced with both techniques. A Student's paired t-test with a two-tailed distribution was performed between groups. Alpha was set at 0.05 to determine statistical significance. Statistical analysis was performed with JMP (SAS Institute, Cary, NC).

Experimental setup showing 6 × 4 mm BegoStone confined within a polyurethane holder at under 0.9% saline, atop sequential sieves of 3, 2, and 1 mm.
URS deflection and flow
URS deflection was tested in five new fourth generation URSs, including the Flex-Xc (Karl Storz, Germany), URF-P6 (Olympus, Japan), URF-V2 (Olympus, Japan), Cobra (Richard Wolf, Germany), and LithoVue (Boston Scientific, United States). The 2.0F probe was tested along with the 200 μm Flexiva TracTip Laser fiber (Boston Scientific) and 1.9F Zero Tip Nitinol basket (Boston Scientific). The URS was placed on a 1/10" grid and photographed in the straight, fully upward-deflected and fully downward-deflected position with no instruments in the working channel followed by placement of the adjunctive instruments. The angle of the tip to the shaft of the instrument was measured as the maximal deflection.
Irrigation flow through each of the URSs was tested with an empty channel, the 2.0F NPL probe, the 200 μm laser fiber, and a 1.9F wire basket. Physiologic saline was run at maximum flow at a pressure of 100 cm above the URS. Time to reach 10 cc of total flow, as measured by 10.0 g weight in the collection container, was recorded.
Results
Stone fragmentation efficiency
NPL with the 2.0F probe required significantly less energy than the HoL with the 200 μm fiber to make the initial fracture of the stone (46.2 J vs 368.0 J, p = 0.026) and trended toward requiring less time to do so, although this was not significant (30.6 seconds vs 86.4 seconds, p = 0.104). The final fracture of the stone occurred earlier with NPL (151.8 seconds vs 248.8 seconds, p = 0.008), with less total energy required (167.2 J vs 940.0 J, p = 0.0004). The 2.0F NPL probe showed an overall SFE of 86 mg/min, which was significantly greater than the 200 μm laser fiber at 52 mg/min, p = 0.014 (Fig. 2).
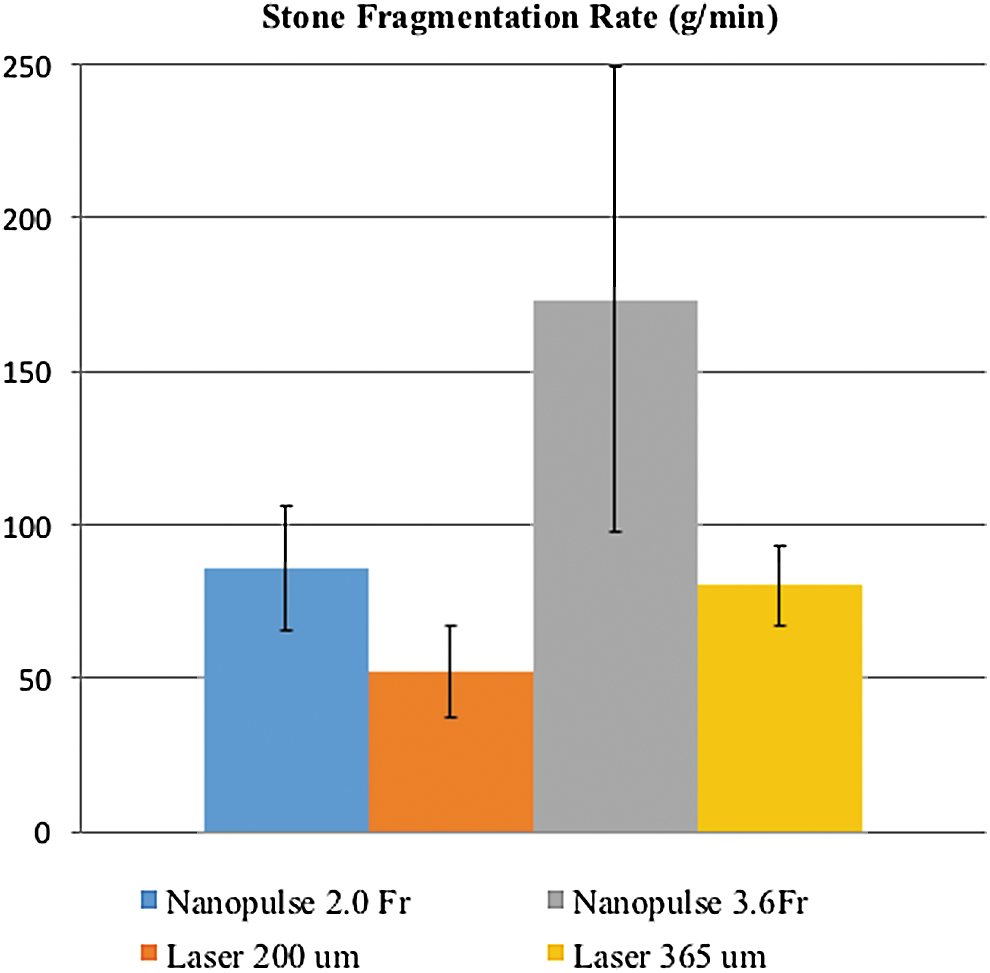
The 2.0F NPL showed improved stone fragmentation efficiency compared with the 200 μm laser (86 mg/min vs 52 mg/min, p = 0.014) as did the 3.6F NPL vs the 365 μm laser (173 mg/min vs 80 mg/min, p = 0.05). NPL = Nanopulse lithotripsy.
The 3.6F NPL probe, compared with the 365 μm laser fiber, showed similar results to the smaller probes with regard to time to first fracture, time to final fracture, and energy usage. The 3.6F NPL probe had a fragmentation efficiency of 173 mg/min, which was significantly more than the 365 μm laser fiber (80 mg/min, p = 0.05).
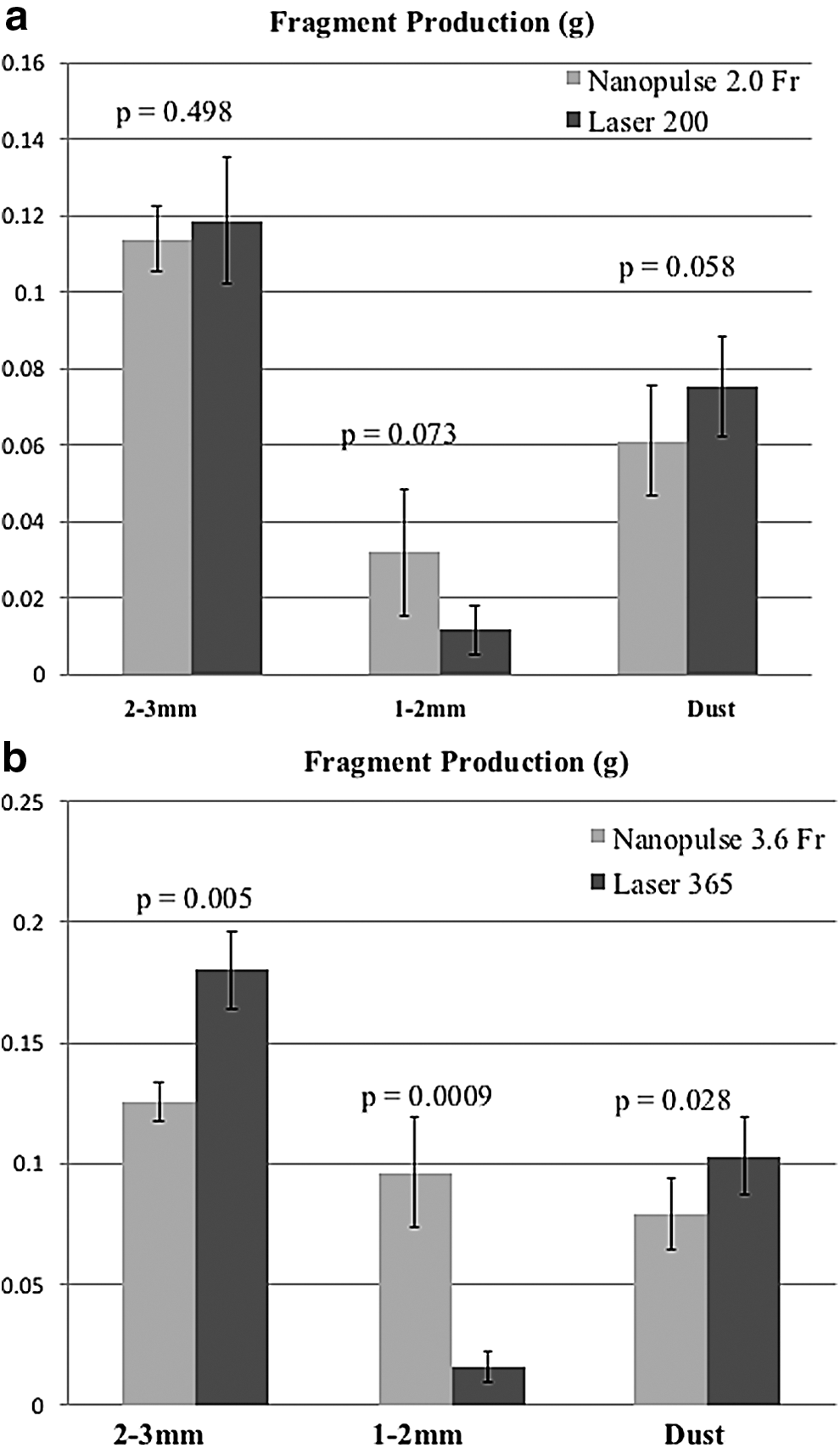
The fragment sizes differed between the two modalities (Fig. 3a, b). NPL with the 2.0F probe tended to create more 1 to 2 mm fragments than the HoL with the 200 μm fiber while the laser created more dust; the difference was statistically significant between the 3.6F NPL probe and 365 μm laser fiber (p = 0.0009 for 1 to 2 mm fragments and p = 0.028 for dust).
URS deflection and flow
In the five URSs tested, maximal URS deflection reduced by an average of 3.75° with the 2.0 NPL probe, compared with 3.5° with a 200 μm laser and 4° with a 1.9F basket (Table 2).
HoL = Holmium laser lithotripsy; NPL = Nanopulse lithotripsy.
The average flow with an empty channel among the tested flexible URSs was 36.5 mL/min. This was reduced to an average of 18.3 mL/min with the 200 μm laser fiber and to 6.3 mL/min with the 2.0F NPL probe.
Discussion
NPL aims to distinguish itself from EHL and find a position in the market dominated by HoL as an efficient, more cost-effective and reusable probe lithotripter. To do so, it must show a sharp difference from its EHL counterpart with regard to efficacy, complication rate, and noninferiority to HoL, the modality with which most urologists are comfortable. 5,6 NPL indeed offers a compelling alternative to the holmium laser lithotripter. The SFE of NPL was clearly superior to the laser for a confined stone in the in vitro setting. The URS deflection was not altered in a clinically significant way compared with the laser, although the flow through the URS diminished with NPL to about 1/3 that of the flow with the laser in place, similar to other devices 2F to 2.4F in diameter.
Further inquiries into its exact mechanism of action may further distinguish it from EHL, which has the unfortunate reputation of poor safety in the upper urinary tract. 7 Some authors have suggested that the mechanism of action of NPL is strictly dielectric breakdown, a technique discovered in the 1960s whereby a strong current can be used to fragment geologic materials. 6,8 The device generates an electric field so intense that the current passes directly from the probe into the urinary stone (which is typically nonconducting), thereby causing a plasma channel to form and a microexplosion at the point of contact. A crater forms on the stone surface; microcracks develop around the crater that, after successive pulse, combines to fragment the stone.
Our inquiries into its mechanism of action have not led to such straightforward conclusions. In fact, there appears to be a mix of dielectric breakdown with the more conventional mechanisms typically seen with EHL such as shock wave and cavitation erosion. 1 The role each plays in the fragmentation of stones is not completely understood, but suffices it to say, it is clearly distinct in some ways from EHL.
The safety profile of NPL appears reasonable. A study of tissue effects in ex vivo human ureters and kidneys showed morphologic changes into the submucosal layer of the urothelium after 10 direct-contact pulses at 1.0 J, but there was no extension into the muscle layer and no evidence of ureteral perforation. 2 A canine study of direct-contact NPL in ureters and bladders showed only superficial morphologic changes at 0.1 to 0.7 J. While energy ≥0.8 J caused injury to all layers of the bladder or ureter, these changes appeared reversible, and there were no ureteral strictures on follow-up at 1 year. 3 One clinical study of its efficacy and safety has been performed. The study included 879 patients in three centers in Tomsk, Russia, who underwent NPL for stones of differing sizes and compositions in the ureter, kidney, and bladder. The study showed reduced complication rates compared with historical data on HoL, without an additional risk of ureteral perforation. Stone-free rates (all fragments ≤1.5 mm) were reported at 96%. These results, along with number of pulses required and operative time, appeared to show improved efficiency compared with HoL. 9 The device has not yet been used in the clinical setting in the United States.
The other remaining issue is that of cost. In the markets where it is currently available, the device is significantly less expensive than a holmium laser, including capital and disposable costs. The 2.0F probes are less expensive and reusable between patients for a total of 400 pulses (the larger probes have more pulses available), which should last for multiple cases. Indeed, in the clinical study, the number of pulses required was far less than 400. On average, a ureter stone was fragmented with 35 ± 31 pulses and a renal stone required 60 ± 23 pulses. 9 However, we have noticed that the inner probe degrades with each pulse, shortening over time compared with the outer sheath. This effect worsens the probe's contact with the stone, making the discharges appear less effective over time.
The NPL device may be able to replace the HoL in many Operating Rooms (ORs), but there will be differences in how each is used. The NPL will best serve surgeons aiming for stone fragmentation rather than dusting. Maintaining direct soft-pressure contact with the stone may be challenging for attempts to “popcorn” stones. Flow will also be limited compared with the holmium laser in the flexible URS as expected with other devices >2.0F in diameter. But the NPL device may certainly prove useful for many bladder, ureter, and kidney stones as it has in other countries. Overall, the authors were impressed with the fragmentation capabilities of the NPL and welcome the development of safe, efficient, and cost-effective technologies in the operating room.
Conclusion
The Nanopulse lithotripter showed improved SFE compared with the holmium laser with more fragmentation and less dust creation. The 2.0F and larger NPL probes limit flow as expected with other devices >2.0F in diameter, but the 2.0F probe does not limit URS deflection. NPL offers an effective alternative to HoL.
Footnotes
Author Disclosure Statement
No competing financial interests exist.