
Abstract
Objective:
We compared postoperative outcomes and quality of life (QoL) between patients who received a nephrostomy tube vs a ureteral stent following percutaneous nephrolithotomy (PCNL) in a prospective, double-blind, randomized manner.
Materials and Methods:
Between September 2015 and March 2016, we randomized 30 patients undergoing PCNL to receive nephrostomy drainage (Group 1: 8F or 10F) or Double-J ureteral stent (Group 2) at conclusion of surgery. Nephrostomy tubes were removed within 48 hours (before discharge) and ureteral stents were removed at least 2 weeks after surgery. Patients' QoL was assessed with the Wisconsin StoneQOL questionnaire preoperatively and then 7 to 10 days and 30 days following surgery. Inclusion criteria included an uncomplicated procedure, normal preoperative renal function, and clinically insignificant residual stone fragments on postoperative imaging. We calculated the preoperative and postoperative QoL score difference between the two groups. We also evaluated perioperative characteristics, inpatient analgesic requirements, length of stay (LOS), and postsurgical complications.
Outcome:
Patient characteristics between Groups 1 and 2 were comparable with similar age (58.3 vs 54.7, p = 0.534), gender ratio, and stone burden (276.6 mm2 vs 259 mm2, p = 0.84) and composition. There was no significant difference between perioperative outcomes, including stone-free rate (93.3% vs 86.7%), operative times (125.7 minutes vs 115 minutes, p = 0.29), estimated blood loss (103.3 mL vs 100.7 mL, p = 0.9), LOS (3.2 days vs 1.9 days, p = 0.1), and complications (2 in each group). Inpatient analgesic requirements were also the same (both 21.1 mg, p = 1.0). Assessment of QoL using the Wisconsin StoneQOL questionnaire showed significant differences between preoperative and postoperative health-related QoL in 18 of the 28-question instrument at 7 to 10 days. Patients in Group 2 had significantly worse QoL change and a multitude of negative responses on the StoneQOL assessment, not only those commonly associated with stent irritation. Eighty percent of participants in Group 2 also attributed their complaints to having a stent placed. Both groups had similar QoL status at 30 days after surgery.
Conclusion:
Despite the literature advocating “tubeless” PCNL with ureteral stent placement at conclusion of surgery, our randomized prospective study shows that QoL is significantly worse with stent placement than with temporary nephrostomy drainage in the immediate aftermath following PCNL, using a validated QoL assessment instrument specific for nephrolithiasis.
Introduction
P
The Wisconsin StoneQOL has been validated as a disease-specific instrument that is capable of assessing the health-related QoL of patients with nephrolithiasis by capturing the symptoms and challenges associated with stone formers. 6 What has been shown by Penniston and Nakada is that this QoL assessment tool could qualify patients' functional capacity and perceptions of their own health within the disease-specific domain of urolithiasis and especially after intervention. We choose to use this QoL instrument as opposed to a general measure of QoL assessment specifically for this reason.
Materials and Methods
Between September 2015 and March 2016, 30 patients with nonobstructing renal calculi undergoing PCNL were randomized in a 1:1 manner under institutional review board (IRB) protocol to receive a cope loop nephrostomy drain (10F or 12F) (Group 1, 15 patients) or a Double-J ureteral stent (Group 2, 15 patients) at completion of surgery. Randomization was performed immediately before tube insertion using a blinded preselected schedule. Study inclusion criteria included normal preoperative renal function, uncomplicated procedure without significant intraoperative blood loss, no history of
Patient characteristics in both groups were comparable with similar age (58.3 vs 54.7, p = 0.534), gender (seven females and eight males in Group 1 vs six females and nine males in Group 2), American Society of Anesthesiologists (ASA) class, overall stone burden (276.6 mm2 vs 259 mm2, p = 0.84) and composition (Table 1). They were also largely asymptomatic without any obstruction from their stone burden preoperatively.
EBL = estimated blood loss; PCNL = percutaneous nephrolithotomy.
Standard technique for PCNL was used after obtaining our own percutaneous access into the collecting system. All procedures were performed with the patient under general anesthesia lying in the prone position and with a ureteral catheter inserted in a retrograde manner on the ipsilateral side. Retrograde pyelogram provided visualization and optimal calix selection for fluoroscopic percutaneous access using a bull's eye technique with an 18-gauge diamond-tip needle into the desired calix. A 0.038-inch Sensor wire (Boston Scientific, Marlborough, MA) or Safety-J wire (Cook Medical, Bloomington, IN) was coiled in the collecting system and an X-Force balloon dilator (Bard Medical, New Providence, NJ) was used to dilate the tract to accommodate a 30F sheath. Lithotripsy and stone disintegration were accomplished with a CyberWand dual ultrasonic lithotripter (Olympus America, Center Valley, PA) and fragments removed with a two-prong peanut grasper. At time of tube placement, an enclosed envelope with predetermined indication for nephrostomy or stent was opened and the indicated drainage choice was placed. The 10F or 12F cope loop nephrostomy tube (Cook) was placed directed through the sheath and the 6F Percuflex Plus ureteral stent (Boston Scientific) was advanced via either antegrade or retrograde approach over a wire. Eight of the 15 patients in Group 2 had fibrin sealant (FloSeal, Baxter, Deerfield, IL) injected into the access tract and 7 patients had a 2-0 Vicryl suture placed after the access sheath was removed. No patients had fibrin sealant in the nephrostomy group. Fibrin sealant usage was solely based on attending surgeon preference (D.M.H.). Appropriate positioning of either the nephrostomy tube or stent was confirmed with fluoroscopy before returning the patient to the supine position for extubation. All patients had a Foley catheter placed for bladder drainage that was removed the next morning.
The nephrostomy tubes in Group 1 patients were removed before discharge, usually 48 hours after surgery, while the stents were left in place for at least 2 weeks and removed via cystoscopy in the office. The nephrostomy tract site was covered with a dressing without any additional sealant or suturing after tube removal. All patients underwent a CT of abdomen/pelvis (CTAP) to assess for residual stones the day after surgery before discharge; those patients who required second-stage procedures had postoperative imaging at completion of their stone removal. We considered stone free to be completely cleared of fragments and clinically insignificant residual stone fragment to be less than 4 mm.
We assessed patients' QoL using the Wisconsin StoneQOL questionnaire. Patients were asked to complete the 28-question instrument before their surgery, either during their initial office visit or a few days before surgery over the telephone. All answers were collected and recorded at time of assessment. Patients were then called at home 7 to 10 days after their surgery to reassess their QoL using the same questionnaire and again at 30 days after PCNL. All patient answers were collected in this manner except for one whose hospitalization was prolonged because of placement issues (he came from a nursing facility and there were some logistical issues in preparing for his return). Patients were also asked what they thought was the most unfavorable part of their postsurgical experience at time of the final QoL assessment.
Because patient baseline answers on the Wisconsin StoneQOL were different, we assigned numerical numbers to the various answer levels from questionnaire: “very true” was 1, “mostly true” was 2, “somewhat true” was 3, “a little true” was 4, and “not at all true” was 5. We compared the differences between the QoL answers of the two groups before and after surgery to come up with a difference quotient. All statistical analysis was done with the paired t-test for categorical and continuous variables. We considered p < 0.05 to be statistically significant.
Results
There was no significant difference between perioperative outcomes of Group 1 and 2, including stone-free rate (93.3% vs 86.7%), operative times (125.7 minutes vs 115 minutes, p = 0.29), estimated blood loss (EBL: 103.3 mL vs 100.7 mL, p = 0.9), LOS (3.2 days vs 1.9 days, p = 0.1), and complications (2 in each group). Inpatient analgesic requirements were also the same (both 21.1 mg IV morphine equivalent, p = 1). Results are summarized in Table 1. Hg drop from preoperative to immediately after surgery in the recovery unit showed no difference (1.3 mg/dL vs 1.4 mg/dL, p = 0.76) and similar transfusion rates (one patient in Group 1 and two in Group 2), consistent with the similar mean EBL of both groups.
Two patients in Group 2 required second-stage PCNL for large initial stone burden and one patient in Group 1 required second-look ureteroscopy. Determination was based largely on CTAP after initial surgery. These patients were randomized at the conclusion of the repeat operation to determine postoperative drainage. Stone composition was mostly calcium oxalate or mixed calcium based and did not appear to significantly alter operative times. There was one struvite stone in Group 1. Complications in Group 1 included one patient with postoperative systemic inflammatory response syndrome and bacteremia (Clavien 2) who required additional IV antibiotics (which increased LOS to 5 days), and one subcapsular perinephric hematoma patient (Clavien 2) who presented 2 weeks later requiring transfusion but no additional intervention. In Group 2, one patient required a small chest tube for decompression of pleural effusion (fluid was negative for creatinine) (Clavien 3), and another presented after discharge with fevers and chills and was admitted for evaluation (Clavien 2) and blood cultures (ultimately negative).
The frequency of responses before and after surgery to the various elements of the Wisconsin StoneQOL questionnaire is displayed in Table 2. We also evaluated the mean difference between preoperative and postoperative scores for each answer between the two groups. Assessment of QoL using the questionnaire showed significant differences between preoperative and postoperative health-related QoL in 18 of the 28-question instrument at 7 to 10 days. Patients in Group 2 had significantly worse QoL change and a multitude of negative responses on the StoneQOL assessment, not only those commonly associated with stent irritation (nocturia, frequency, and urgency). The analysis showed that patients with stents, at a week after surgery, were more fatigued and had trouble sleeping. They also attended less social events, were less motivated and focused at work, and even missed work or family time. Patients in Group 2 had some amount of physical pain or discomfort (worse than before surgery) and were less interested in sex or socializing. They were also more frustrated, worried, annoyed by inconveniences, and more irritable than usual. A visual interpretation of the QoL difference is displayed in Figure 1. All data points outside of line 0 denote improvements in QoL condition, while those inside of line 0 show worsening QoL condition after surgery. These symptoms and complaints improved as recovery time increased and patients' ureteral stents were removed—both groups had similar or improved QoL status relative to their baseline at 30 days after surgery.
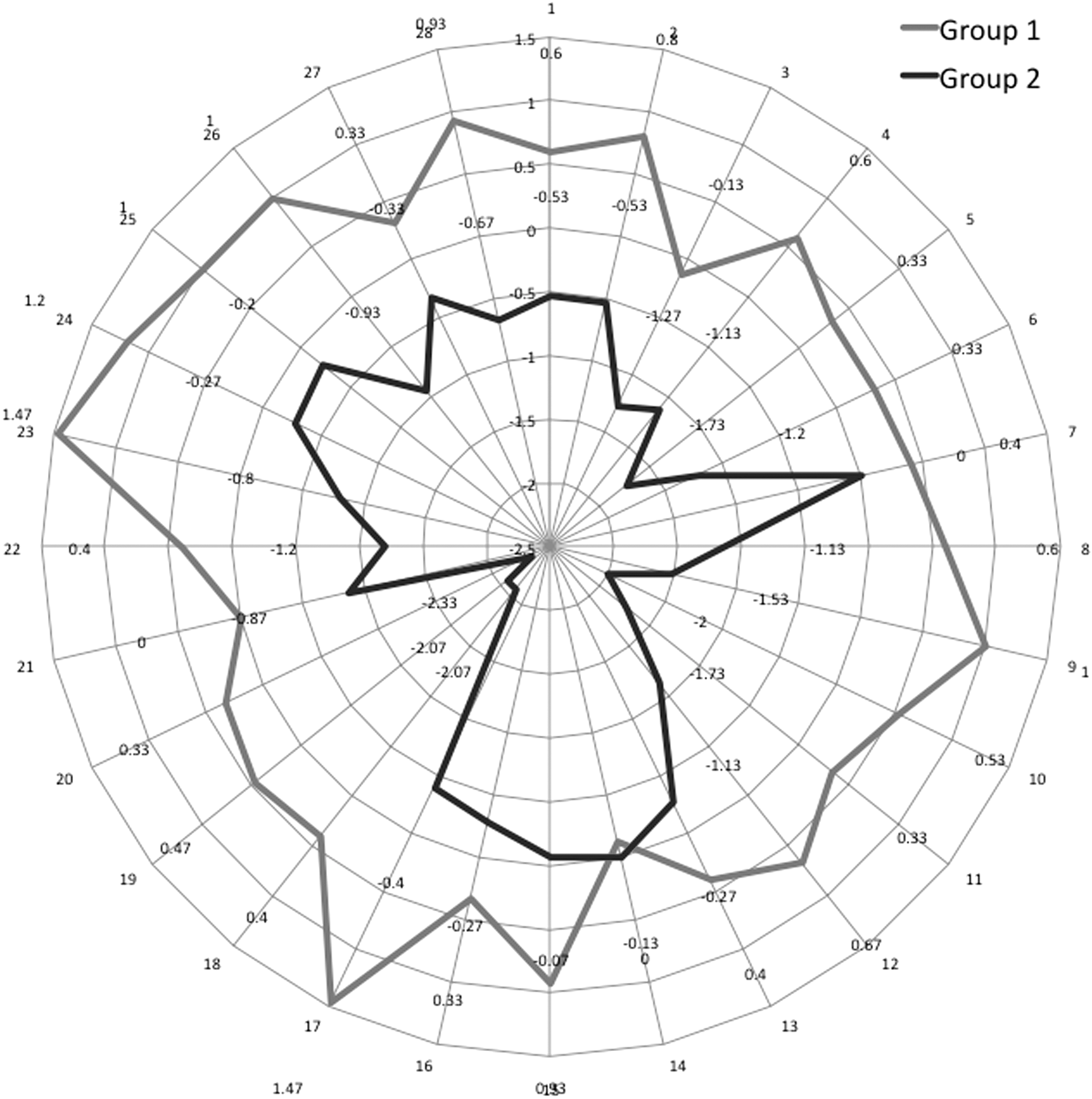
Visual interpretation of QoL score differences between Groups 1 and 2.
QoL = quality of life.
Twelve patients (80%) in Group 2 directly described having the stent as the “worst” part of the surgical and postoperative experience.
Discussion
There are benefits to placing a nephrostomy tube after PCNL—specifically improved drainage of the kidney and tamponade of the access tract to stop any potential bleeding. The literature has shown some drawbacks of nephrostomy tube drainage after PCNL in the sense of prolonged hospital stay and increased demand for analgesics. 7 –9 Because of Bellman and colleagues 10 success in the 1990s with the first reported “tubeless” PCNL, this technique had gained popularity and has become the standard approach, when appropriate, for many endourologists, not just those in the United States but also throughout the world. Our study did not show any statistically significant improvements in LOS or analgesic use between the two groups, but differences between the two groups (3.2 days vs 1.9 days) may have reached statistical significance with a larger cohort.
Analgesic use is the same between the two groups, although this may be partially attributed to one patient who had significant and atypical pain after PCNL requiring 89.6 mg of IV morphine equivalent narcotics over the course of her 3 days of admission. However, even after excluding this patient from analysis, the mean narcotic use between the two groups was still not statistically significant over this cohort size. This study differs from prior reports by decreasing the size of postoperative nephrostomy tube to 10F or 12F, and may account for the relatively equivalent narcotic requirements in our two groups. Prior studies included the use of large-bore nephrostomy tubes (>18F) postoperatively, and several studies have shown that postoperative pain is closely associated with tube size. 11
Our study echoes several recent studies, which have also found no significant difference in analgesic requirement between tubeless and small-bore nephrostomy after PCNL. 12,13 LOS difference also did not reach significance, although if we exclude the two patients with the longest LOS from each group, the results do become statistically significant (Group 1: 2.54 days, Group 2: 1.38 days, p < 0.05). In addition, as previously discussed, a larger cohort size would also be more likely to show statistical significance in terms of LOS.
Our stone clearance rates were similar between the two groups—93.3% for Group 1 and 86.7% for Group 2. These results are comparable to those of other large PCNL cohorts. 14 –16 We did not use a direct vision endoscopic access or dual ureteroscopy and nephrolithotomy approach as advocated by others in the field. 14 –16 There approaches are all valid and effective at achieving stone-free status (>90%) but require two separate visualization platforms—one for retrograde and one for antegrade approach, and also two separate pairs of experienced hands to tackle the stones from both direction, resources that are not available at all urologic centers at all times. No other perioperative parameters or postsurgical outcomes were found to be significantly different between the two groups. Fibrin sealant injection demonstrated no difference in outcomes between the patients in Group 2, consistent with outcomes in the literature where sealants have been used to help close the access tract. 17,18
In today's healthcare environment, patient satisfaction and QoL are increasingly becoming goals of care in addition to surgical safety and outcomes. In urology, QoL and treatment impact on patient satisfaction are huge factors in prostate cancer that have been well documented. 19,20 However, the literature on QoL in stone disease is severely lacking. In fact, there is only one study on QoL status post-PCNL. 21 We felt it was important to address this aspect of patient perception of outcome in a manner that also allowed us to examine one of the trends in endourology—the shift toward “tubeless” PCNL. That being said, limitations of this study include the smaller sample size and the recognition that QoL changes postoperatively were not measured on a daily basis. We selected 7 to 10 days postoperative for the QoL assessment to provide for reasonable expectations of improvement from surgical site pain. We also did not alter surgeon preferences with respect to time indwelling for either nephrostomy tubes or stents, and it could be argued that an earlier stent removal with strings rather than cystoscopy would demonstrate an earlier improvement at the 7- to 10-day QoL scores.
What we have found is that “tubeless” does not entail an improvement in QoL as it does in some of the other surgical outcomes that we discussed, and this is likely due to the lower tract symptoms associated with the indwelling stent. The Wisconsin StoneQOL has been validated in heterogeneous groups of stone formers and demonstrated to detect meaningful improvements and decreases in patients' QoL over time. In our study, we demonstrate a significant decrease in QoL in Group 2, and it raises questions as to whether this goes beyond the normal stent symptoms. Understandably, stent colic and lower urinary tract symptoms are well correlated with stents and represent significant clinical problems for many patients after intervention. 22 Despite this, we were surprised to see responses that did not fall specifically within the domain of stent colic, including trouble sleeping and poor sleep quality, decreased motivation, and less interest in socializing and attending social events. In fact, many of the QoL elements decreased by more than one level.
Specifically, there were four response elements with a mean negative score of 2 or more, indicating the response worsened by two levels (e.g., from “not at all” to “somewhat true” or from “somewhat true” to “very true”). These responses were all statistically significant between the two groups and included (1) missed work/family time; (2) urinary frequency; (3) urinary urgency; and (4) less interest in sex/intimacy. These are important contributors to general well-being especially in the immediate time frame following surgery, not to mention decreases to social productivity. In fact, the majority of patients (80%) in Group 2 attributed a significant amount of their discomfort and QoL disruption directly to the stent, based on their follow-up assessment at 30 days.
Originally, we performed a sample size calculation with a confidence level of 95% and a confidence interval of 10 (28 questions on the Wisconsin StoneQOL and 1 to 5 points per questions with a total range of 28 to 140 points for each patient). Using the central limit theorem, we felt a 10-point difference in either direction of the mean (56 points) would be sufficient to cover the margin of error. The sample size obtained using these parameters was 96 patients in total. Interestingly, we were able to realize statistical significance in the QoL difference even with the relatively small number of patients we enrolled (30 patients), indicating that the QoL disparity between the two groups appears profound. The interval when the first postoperative QoL assessment is performed could have been deferred to the 2-week mark immediately before the ureteral stent was removed to show that QoL differences are attributable entirely to the stent. In addition, due to heterogeneity, some preexisting conditions or home situation may have existed in Group 2 that confounded the degree of QoL difference between the two groups. Still, the data are of interest because they underscore the significant contribution of the indwelling stent to patients' overall well-being, and they provide a target for future studies to assess post-PCNL results.
We are still in the process of recruiting additional patients to this study with the goal of 50 patients in each arm to meet our original sample size. However, because patients do have some preconceptions about having a nephrostomy tube vs having a stent, some of them have refused to consent to the randomization, introducing an element of selection bias into the study. The study is ongoing and we hope to submit an update when we have an analysis of a 100 total patients.
Conclusion
In our randomized prospective study, “tubeless” PCNL with ureteral stent placement did not significantly reduce hospital LOS or inpatient analgesic requirements compared with nephrostomy tube drainage for 48 hours after surgery. When assessing for health-related QoL using the Wisconsin StoneQOL, we found the group with stents performed significantly worse 7 to 10 days after surgery in 18 of the 28-questionnaire elements compared with the nephrostomy group. Not only did participants respond negatively about stent-related symptoms but they also had significant detrimental effects, including increased fatigue; loss of sleep and sleep quality; less motivation, interest, and focus for work and daily activities; need to change their daily schedules and implement travel arrangements; and were seemingly more frustrated, worried, annoyed, and irritable.
Through reduction of the nephrostomy tube size, we appear to see an improvement in the immediate postoperative pain following PCNL. It is likely that earlier removal of an indwelling stent may mitigate some of these QoL concerns. Certainly, additional randomized trials on QoL following PCNL and other endourologic procedures will be needed to help define and balance the optimal management of these patients in terms of minimizing pain, bother, and hospital LOS, while maintaining excellent stone clearance, patient well-being, and rapid return to preoperative function and QoL.
Footnotes
Author Disclosure Statement
No competing financial interests exist.