
Abstract
Purpose:
Urologists and radiologists should be aware of the CT scan appearance of laparoscopic partial nephrectomy (LPN) with the various hemostatic agents since they may confound the interpretation of these radiographic findings. We report the various postoperative CT scan appearance and changes after LPN.
Materials and Methods:
We reviewed CT scans retrospectively (within 3 months) of 86 patients who underwent LPN using various hemostatic agents between March 2008 and July 2014. We analyzed the CT findings after LPN, including postoperative changes, tumor recurrence, and complications. We also discuss changes in abnormal features, such as mass-like lesions and gas formation, on follow-up CT scans.
Results:
To categorize the postoperative changes, we classified them according to their specific CT findings: (1) a combination of perinephric stranding and postsurgical fluid collection (n = 46), (2) mass-like lesions (n = 35), (3) a parenchymal defect (n = 2), (4) local recurrence at the surgical site (n = 1), (5) a large hematoma as a complication after LPN (n = 2), (6) gas pockets, which may be a response to postsurgical fluid collection around soft tissue (n = 35), (7) fat at the excision site (n = 2; Fig. 7), and (8) contrast extravasation in the delayed phase (n = 1). Mass-like lesions were visible in 35 cases. The average change in size of bolster masses was −1.19 mm/month. However, the overall change in enhancement of mass-like lesions was not significant over time. Foci of gas were noted in 16 patients at the resection site in the first follow-up period (<3 months), as late as 40 days after the procedure.
Conclusions:
Knowledge of CT imaging features and changes in hemostatic agents following LPN is important in interpreting postoperative CT scans, as postoperative changes can be confused with tumor recurrence and can mimic abscesses.
Introduction
P
Imaging surveillance after PN is usually performed using CT. CT findings after laparoscopic partial nephrectomy (LPN) differ from those after conventional open procedure. After OPN, a wedge-shaped defect, perinephric stranding with hematoma, or perirenal fluid collection in the kidney is typically seen. 1
LPN is considered to have a steep learning curve and the potential for fatal complications, such as postoperative hemorrhage, compared with OPN and radical nephrectomy. 2,3 To maximize hemostasis following the excision of the tumor and to reduce the rate of postoperative hemorrhagic events, various hemostatic tools, such as oxidized regenerated cellulose, gelatin matrix hemostatic sealant, and fibrin sealant, have been used in laparoscopic surgeries. These agents cause changes in the kidney and retroperitoneal space, such as postoperative granuloma, bolster-related mass-like lesions, perinephric stranding, and gas formation, which are visible on CT images. 4,5
These postoperative changes on CT scans can be interpreted as tumor recurrence, an abscess, or complications caused by morphologic and enhancement characteristics because of poor understanding of CT imaging features and changes in hemostatic agents following LPN.
The purposes of this study were to describe CT appearances following LPN for small renal-cell carcinoma (RCC) and the evolution of follow-up imaging findings.
Materials and Methods
Institutional review board approval was obtained before the initiation of this retrospective study. We reviewed CT scans retrospectively (within 3 months) of 86 patients who underwent LPN using various hemostatic agents between March 2008 and July 2014. We analyzed the CT findings after LPN, including postoperative changes, tumor recurrence, and complications. We also discuss changes in abnormal features, such as mass-like lesions and gas formation, on follow-up CT scans.
LPN surgical technique
A single surgeon (T.S.K.) performed LPN in all patients. The operation was performed with a transperitoneal approach. Main renal arterial clamping or en bloc of the renal hilar vascular pedicle was performed to decrease bleeding and provide a clear surgical field. After masses were excised with laparoscopic scissors, gelatin matrix hemostatic sealant (FloSeal; Baxter Healthcare Corporation, Irvine, CA) was applied to the resection bed to achieve hemostasis. The collecting system defects were repaired with absorbable sutures. A rolled bolster, consisting of oxidized regenerated cellulose (Surgicel; Ethicon, Somerville, NJ), was placed in the parenchymal defect and renorrhaphy was performed on healthy renal parenchyma. Then, fibrin sealant (Tisseel VH Kit; Baxter Healthcare Corporation) was placed to cover the renorrhaphy site. Finally, after the reconstruction was finished, the vascular clamp was released to restore circulation.
Radiologic evaluation methods
Our stage-based surveillance protocol is an abdominal CT scan at 3 months postoperative for patients treated with PN to evaluate the residual renal appearance, but it is optional. With abnormal CT findings, such as mass-like lesions, gas foci, or suspicion of tumor recurrence at 3 months, or risk factors such as margin-positive histopathologic results, abdominal CT is recommended at 6, 12, 24, 36, 48, and 60 months. Recommended surveillance includes a clinical assessment, blood biochemistry, and a chest X-ray every 6 months for 3 years, then yearly. Otherwise, abdominal CT scans are performed yearly for 5 years in patients with low risk (pT1, N0, margin negative) or nonspecific findings on the CT scan at 3 months.
In total, patients with a clinical indication for abdominal CT were enrolled in the study using a DS-CT scanner (Siemens SOMATOM Definition Flash; Siemens Healthcare, Forchheim, Germany). All patients were scanned using the standard abdominal scan parameters with real-time automatic exposure control and a quality reference tube current time product of 200 mA. The tube current was partitioned equally on both X-ray tubes of the DS system, operated at 120 kV.
Two radiologists (J.G.P. and H.K.) and two urologists (T.S.K. and P.M.K.) reviewed by consensus each CT scan to assess a predetermined set of radiologic variables. Attributes assessed on preoperative CT images included the axial dimensions of the mass and pre- and postenhancement attenuation values. Postoperative CT radiologic variables included the size and shape of the postoperative mass and enhancement. At least three regions of interest (ROIs) were evaluated, and ROIs were placed at the same locations on pre- and postoperative CT images. Additional findings relevant to image interpretation, such as collection of gas, fat interposition, and contrast leakage at the excision site, were noted. Postoperative CT radiologic variables included the nature of mass-like lesions. Using subsequent follow-up CT examinations, we evaluated whether the largest dimension and enhancement attenuation values in the axial plane changed over time. Postoperative imaging studies were divided into three groups according to the time elapsed following the procedure: those from the first (≤3 months), second (3–9 months), and third (10–13 months) follow-up periods.
Statistical analyses
Statistical analyses were performed using MedCalc (ver. 14.8.1; MedCalc Software, Mariakerke, Belgium). Group comparisons were made using the Mann–Whitney U test for continuous variables and Fisher's exact test for categorical variables. The significance level was set at p < 0.05.
Results
The mean preoperative renal tumor size, measured in the greatest axial dimension, was 2.5 (range 1.0–4.9) cm.
Appearance on CT scans performed within 3 months postoperatively
Postoperative changes on CT differed among cases. To categorize the postoperative changes, we classified them according to their specific CT findings as follows (Table 1): (1) a combination of perinephric stranding and postsurgical fluid collection (n = 46; Fig. 1); (2) mass-like lesions (low-attenuated linear postsurgical stranding, indicating the formation of a pseudocapsule or bolster-related mass; n = 35; Fig. 2); (3) a parenchymal defect (n = 2; Fig. 3); (4) local recurrence at the surgical site (n = 1; Fig. 4); (5) a large hematoma as a complication after LPN (n = 2; Fig. 5); (6) gas pockets, which may be a response to postsurgical fluid collection around soft tissue (n = 35; Fig. 6); (7) fat at the excision site (n = 2; Fig. 7); and (8) contrast extravasation in the delayed phase (n = 1; Fig. 8). (9) Hem-O-lok clips (Weck Closure Systems Research, Triangle Park, NC) on the parenchymal closure (n = 32; Fig. 9).
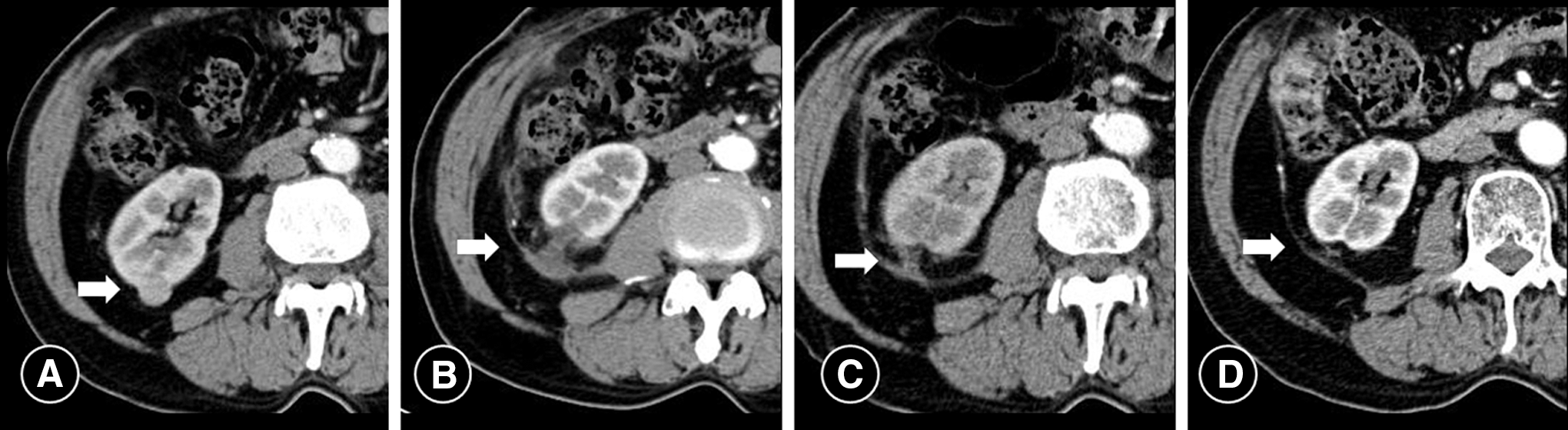
Combination of perinephric stranding and postsurgical fluid collection in a 78-year-old man after LPN for RCC.
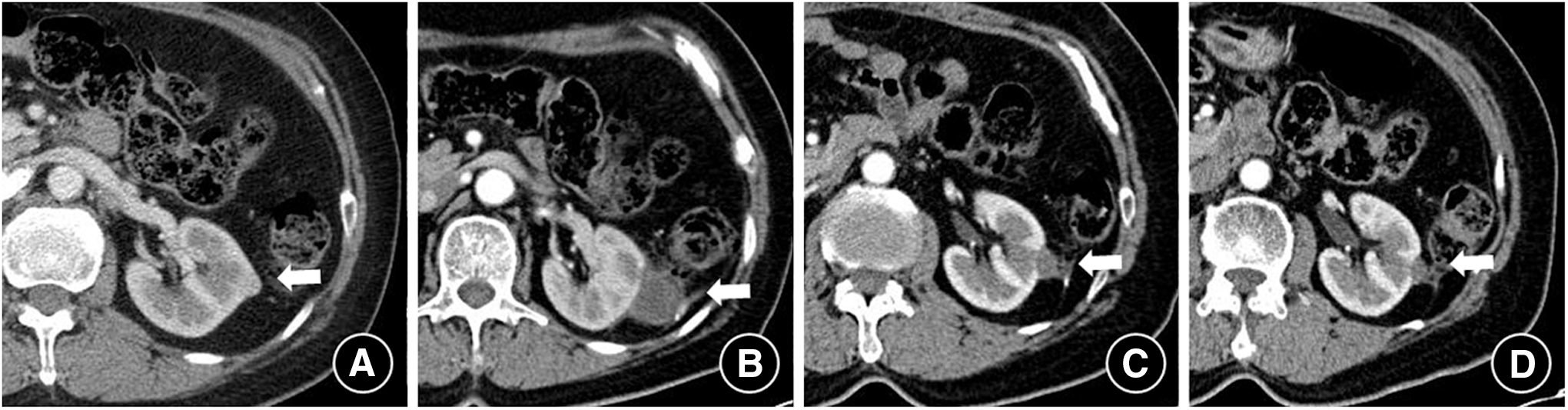
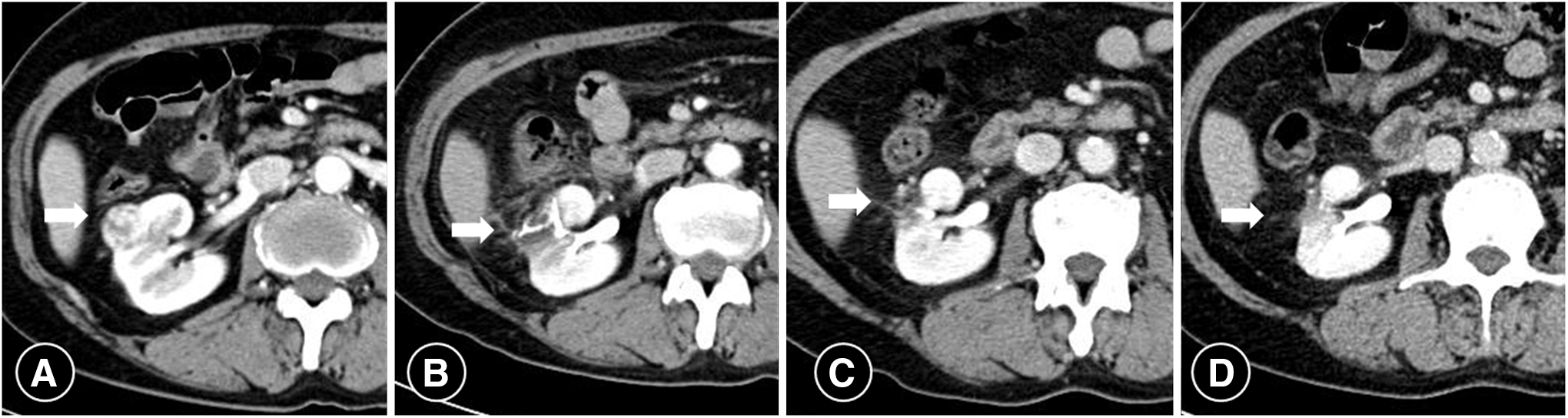
Mass-like lesion (low-attenuated linear postsurgical stranding, indicating the formation of a pseudocapsule or bolster-related mass) in a 59-year-old woman after LPN for RCC.
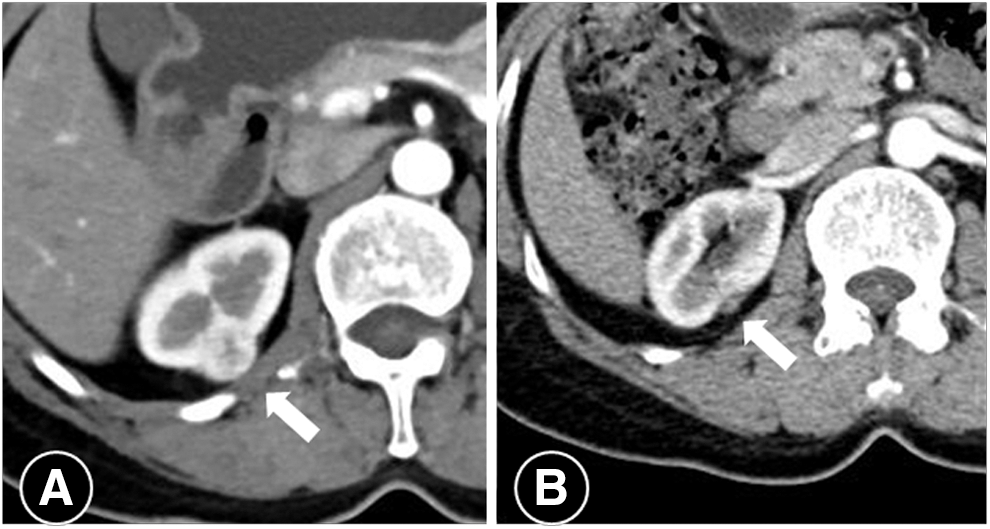
A parenchymal defect in a 58-year-old woman after LPN for RCC.
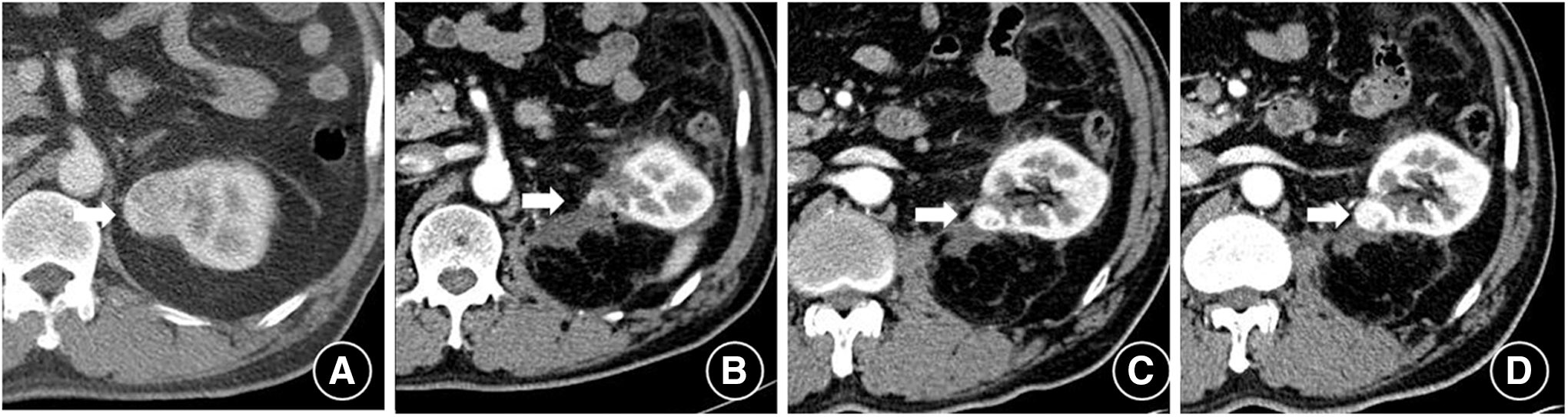
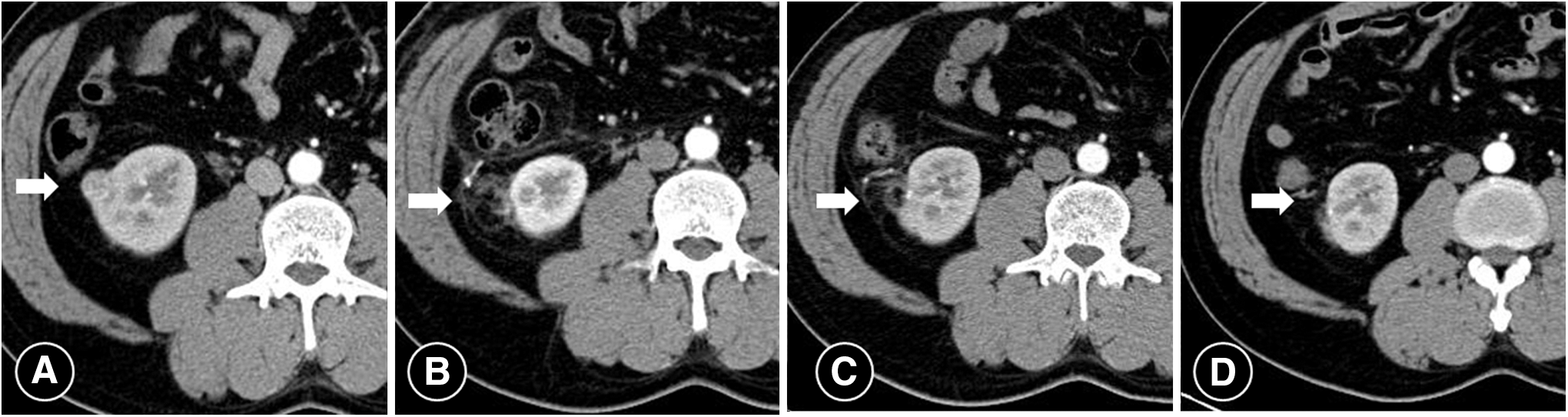
Local recurrence at the surgical site in a 64-year-old man after LPN for RCC.

A large hematoma as a complication after LPN in 42-year-old man after LPN for RCC.
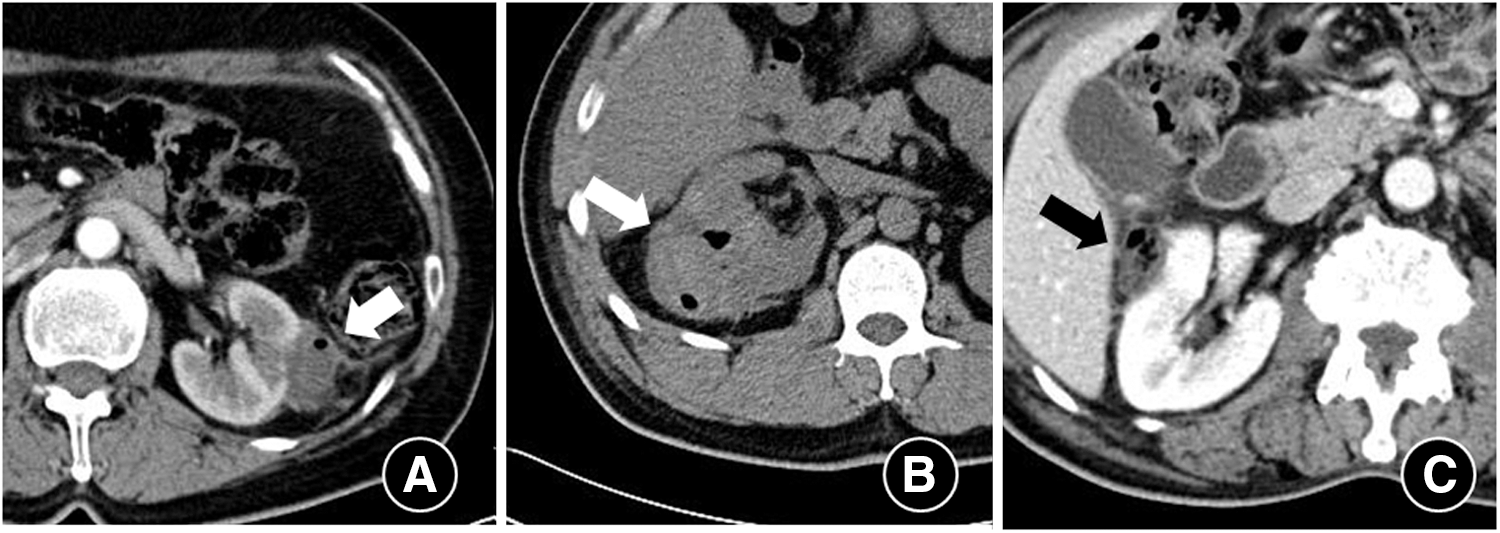
Various gas pocket patterns and hemorrhage at the excision site that could be confused with abscess formation.
Fat at the excision site in a 49-year-old man after LPN for RCC.
Incidentally detected contrast leakage in the nephrographic phase in a 60-year-old woman after LPN for RCC.
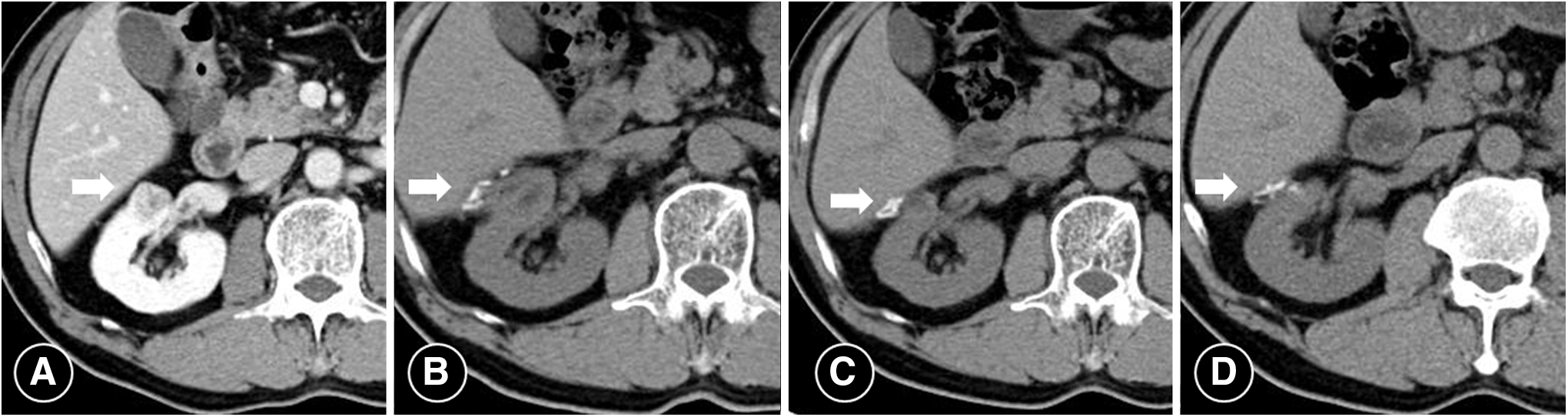
Hem-O-lok at the surgical site in a 56-year-old man after LPN for RCC.
Changes in the morphology and enhancement of mass-like lesions
Mass-like lesions were visible in 35 cases (Table 2). The mean largest axial dimensions of masses were 18.4 (range 10.7–53.1) mm in the first follow-up period (≤3 months), 11.6 (range 2.0–18.9) mm in the second follow-up period (4–9 months), and 7.5 (range 1.0–15.0) mm in the third follow-up period (10–13 months).
HU = Hounsfield units.
The average change in size of bolster masses was −1.19 mm/month. In the first follow-up period (<3 months), mean pre-, early-, and delayed-contrast bolster-related mass attenuation values were 18 (range 5–32) Hounsfield units (HU), 21 (range 11–33) HU, and 19 (range 8–35) HU, respectively. In the second follow-up period (4–9 months), mean pre-, early-, and delayed-contrast bolster-related mass attenuation values were 20 (range 5–41) HU, 22 (range 4–36) HU, and 20 (range 10–45) HU, respectively. In the third follow-up period (10–13 months), mean pre-, early-, and delayed-contrast bolster-related mass attenuation values were 21 (range 7–33) HU, 27 (range 8–51) HU, and 29 (range 9–45) HU, respectively.
The size of postoperative mass-like lesions decreased over time. However, the overall change in enhancement of mass-like lesions was not significant over time.
Postoperative changes in other findings
Foci of gas were noted in 16 patients at the resection site in the first follow-up period (<3 months), as late as 40 days after the procedure. No such finding was noted in later follow-up periods. The Hem-O-lok material was visible in 32 patients in the first follow-up period. All 32 patients were imaged at greater than 12 months and the CT density of these areas averaged 112 HU (range 76–699 HU).
A positive surgical margin was present in 3 of 86 (3.4%) patients undergoing LPNs and all cases were positive at the parenchymal margin. In one case of tumor recurrence, evidence of nodular enhancement was seen at the surgical site. Recurrent tumor showed mass at the excision sites with strong contrast enhancement and increased size on subsequent follow-up CT scans (Fig. 4). In a recurrent case, microscopic examination revealed a clear cell renal carcinoma, grade 3, stage pT1a. The carcinoma invaded the renal parenchymal resection margin, which was positive.
Discussion
Nephron-sparing surgery or PN is preferred for the treatment of early-stage RCC, especially for patients in whom preservation of renal function is a relevant clinical consideration. LPN is steadily gaining ground as an alternative to the more conventional OPN for T1a stage unilateral RCC. 6 LPN is a safe and reliable procedure that offers multiple advantages over the open approach while providing similar oncologic outcomes. The smaller incision and the reduced risk of hemorrhage led to smaller scars, less pain, and shorter recovery times. 7 –10
In comparison with OPN, LPN has a longer and shallower learning curve for urologists, with definite disadvantages being the absence of depth and tactile perception, along with limited range of movement at the surgical site. Major concerns in LPN include the increased warm ischemic time, residual tumor at the excision site, and postoperative complications. These concerns can be minimized by maximizing hemostasis following the excision of the tumor and reducing the rate of postoperative hemorrhagic events. Thus, a wide variety of hemostatic tools have been transferred from open procedure or developed specifically for use during LPN. 11
CT is the most important imaging technique in postoperative surveillance. Postoperative changes in CT findings after LPN for renal tumors depend mainly on surgical techniques and the hemostatic materials used. Because of the differing presentation of abnormal changes following LPN and their similarities to other disease entities, such as tumor recurrence, abscess, and surgical complications, urologists and radiologists should be cognizant of common pitfalls to avoid inadvertent misdiagnosis.
As OPN and LPN procedures gain acceptance and frequency of use, it is important that urologists and radiologists be familiar with the imaging features of postsurgical complications, as well as with normal findings, after PN. After OPN for a small peripheral tumor, a wedge-shaped defect in the renal parenchyma is typically visible on CT and magnetic resonance images. In some cases, surgeons pack perinephric fat into the surgical bed to help achieve hemostasis. The fatty packing material later may be mistaken for a fatty mass, such as an angiomyolipoma. 1
In our study, to categorize these various findings, we classified them according to their specific CT characteristics.
Mass-like lesions
A mass-like lesion is defined as a lesion that shows increased attenuation at the excision site, but no significant enhancement or mass effect. These changes may be caused by various factors, such as surgical damage and the presence of subclinical leakage of blood or urine into the excision site. These mass-like lesions can be caused by a surgical bolster. A rolled oxidized cellulose bolster (Surgicel is knitted into a fabric similar to gauze) applied directly to the site of bleeding can serve as a hemostatic agent. The bolster binds to hemoglobin and facilitates thrombus formation. Platelet aggregation and adjacent foreign body reactions also contribute to its hemostatic properties. It has the ability to cause a space-occupying effect; cellulose becomes engorged, forming a gelatinous mass, when it is exposed to blood. 12,13 Bolsters of bioabsorbable agents can also induce foreign body reactions and form granulomas, mimicking residual tumor. These lesions are frequently interpreted as tumor recurrence, caused by their morphology and enhancement characteristics, because of an absence of awareness of the placement of this sealing agent. 5 A mass-like lesion is formed by intermediate-attenuating tissue with mild delayed enhancement, which has been shown to decrease in size in sequential CT studies.
Deepa and colleagues reported 19 patients who had imaging studies performed more than once and found that there was a decrease in size of the postoperative bolster-related mass with time; the average change was −0.53 mm/month. In our study, the size of postoperative mass-like lesions decreased over time; the average change in size was −1.19 mm/month (Fig. 4). The overall change in the enhancement of mass-like lesions was not significant over time. However, in case of local recurrence at the surgical site, marked enhancing recurrent nodules, above 100 HU, increased by 0.1 mm/month. These findings are not seen in postoperative changes. However, to the best of our knowledge, there are no previous reports on changes in local recurrent tumor size after a PN. Currently, we have a difficulty to explain how the recurrent tumor grew over time. Sowery and Siemens characterized tumor growth in patients managed conservatively for small renal cell masses; they reported an average growth of 0.86 cm/year. 14
Perinephric stranding
Stranding represents a residual postsurgical inflammatory response such as desmoplasia, idiopathic fibrosis, or autoimmune response that evolves in the fibrosclerotic tissue. The renal fascia is often involved in the inflammatory process and appears thickened and retracted toward the surgical site. This sign is specific and can be encountered in a variety of surgical and pathologic conditions, such as pyelonephritis and ureteral obstruction, which are probably the result of similar inflammatory processes. 15
Parenchymal defects
Parenchymal defects can be seen in cases of enucleation of an exophytic peripheral renal mass. Parenchymal defects seen on postoperative CT images usually show no significant change, except a tendency to shrink over time because of scar retraction, on sequential CT studies. However, hematomas and fluid collection at the surgical site may have the appearance of parenchymal defects. Parenchymal margin status is crucial for the evaluation of surgical margins and the identification of residual or recurrent cancers. An ill-defined margin and the presence of enhancing tissue at the surgical excision site are considered to represent tumor recurrence or residual tumor. 4
Secondary formation of gas foci
In our series, 16 cases showed uni- or multifocal collection of gas surrounded by postoperative hematomas at the site of excision. Air is likely trapped within the interstices of the gauze (oxidized cellulose). Although air collection was seen as late as 40 days after the procedure, none was seen in the second follow-up period (4–9 months).
Mass-like lesions with gas can be confused with postoperative abscesses. No such case was seen on our CT scans. Some case reports have described mistaken diagnoses of abscess upon the detection of these lesions on postoperative CT scans. On postoperative CT scans, the appearance of the retained oxidized cellulose could be mistaken for a postoperative abscess, as has been described previously in the liver and brain and in thoracic and gynecologic procedures. 16 –18 The presence of an abscess should be suspected when localized fluid collection with an enhanced rim and containing gas bubbles or a gas-fluid interface is seen. To differentiate air collection consisting of a hemostatic agent containing air bubbles from that consisting of infected fluid containing gas bubbles, consideration of the imaging findings in combination with the patient's clinical signs and laboratory data is necessary.
Appearance of Hem-O-lok clip
Sutures with preplaced Hem-O-lok clips at the tail were used and secured with additional Hem-O-lok clips after the needle was passed and tension on the closure was adjusted in our procedure. The CT scan revealed multiple round radiopaque areas of 3–4 mm each located near the renal parenchyma that were not present in preoperative imaging. The positions of these densities were similar to the positions where the Hem-O-loks were applied, so we believe that these radiopaque objects were Hem-O-loks. The Hem-O-lok material was visible in 32 patients in the first follow-up period. All 32 patients were imaged at greater than 12 months and the CT density of these areas averaged 112 HU (range 76–699 HU). The Hem-O-lok seemed radiopaque and mimicked a calcified density.
Complications related to LPN
Reported complication rates for LPN range from 4% to 37%. Complication rates can be influenced by various factors, including patient status, tumor size and region, surgeon skill and experience, and surgical approach (transperitoneal/retroperitoneal). Commonly reported complications include urinary leak or fistula, bleeding, acute renal failure, and infection. These complications usually occur in the early postoperative period. Most complications can be managed by conservative methods or, at most, endoscopy or interventional radiological procedures.
Limitations of our study include the use of different hemostatic agents during operations and the heterogeneity of data obtained in the follow-up period. In addition, we had no control group, such as a conventional PN with no use of hemostatic agents, so it is not clear whether the results are related to the technique or hemostatic effects.
Conclusions
A combination of perinephric strands and postsurgical fluid collection (53.4%), mass-like lesions (40.6%), foci of gas (40.6%), and Hem-O-lok clips on the parenchymal closure (37.2%) are common visible signs on the initial follow-up CT images after LPN. However, these findings are not of concern regarding tumor recurrence. Recurrences showed masses at the excision site with strong contrast enhancement and they grew over time, especially in the corticomedullary phase.
Knowledge of CT imaging features and changes in hemostatic agents after LPN is important in interpreting postoperative CT scans, as postoperative changes can be confused with tumor recurrence and can mimic abscesses. Familiarity with normal postoperative imaging features, as well as the features that are indicative of complications, is important for appropriate postoperative management. An understanding of the various findings will help to avoid unnecessary repetition of examinations.
Footnotes
Acknowledgment
This study was supported by a grant from Kosin University College of Medicine (2015).
Author Disclosure Statement
No competing financial interest exists.